
Abstract
Study design:
A survey administered to 66 individuals with spinal cord injury (SCI) implementing a choice-based conjoint (CBC) analysis. Six attributes with three levels each were defined and used to generate choice sets with treatment scenarios. Patients were asked to choose the scenario that they preferred most.
Objectives:
To determine the utility weights for treatment characteristics as well as the overall preference for the three types of neural prostheses (NP), that is Brindley, rhizotomy-free Brindley, and pudendal nerve stimulation. Earlier studies have revealed the importance of restoration of bladder function, but no studies have been performed to determine the importance of NP features.
Setting:
Two academic affiliated medical systems’ SCI outpatient and inpatient rehabilitation programs, Cleveland, OH.
Methods:
CBC analysis followed by multinomial logit modeling. Individual part-worth utilities were estimated using hierarchical Bayes.
Results:
Side effects had the greatest significant impact on subject choices, followed by the effectiveness on continence and voiding. NPs with rhizotomy-free sacral root stimulation were preferred (45% first choice) over pudendal afferent nerve stimulation (39% second choice) and sacral root stimulation with rhizotomy (53% third choice). Almost 20% did not want to have an NP at all times.
Conclusion:
CBC has shown to be a valuable tool to support design choices. The data showed that persons would prefer a bladder NP with minimally invasive electrodes, which would give them complete bladder function, with no side effects and that can be operated by pushing a button and they do not have to recharge themselves.
Similar content being viewed by others

Introduction
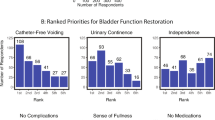
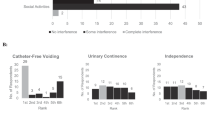
Restoration of bladder function is of high importance for people with spinal cord injury (SCI), because it has a profound negative impact on the quality of life.1 Restoration of bladder function is especially important for paraplegics, for who it is the second highest priority.2, 3, 4
A number of different implantable neural prosthetic approaches show potential and are in development to restore bladder function for individuals with SCI.5 The Brindley approach using sacral root stimulation is most widely used and appears clinically and cost-effective.6, 7, 8 However, clinical acceptance has been limited by individuals choosing not to have this treatment, especially in the United States.
Pudendal afferent nerve stimulation can provide both bladder inhibition9 and micturition10 at a peripheral location. Afferent stimulation combined with sacral root bladder stimulation may provide function without rhizotomy.11, 12 Electrical pudendal nerve block combined with sacral bladder drive has shown effective voiding in animal experiments.13
The characteristics and features of the different neural prostheses (NP) differ from each other, and it is not known how strongly individuals weigh these characteristics when ultimately choosing a given NP solution. Therefore, knowledge of the preferences and concern that potential users have will aid the design and development of NPs and improve clinical implementation.
The purpose of this study was to determine the importance of factors that affect preferences of individuals with SCI for potential NPs to restore bladder function using conjoint analysis.14, 15 By asking patients to choose between two treatment scenarios built of multiple characteristics (attributes), it is possible to imitate possible consumer decisions. Hence, we can calculate preferences of new NP solutions by using the weights of the separate treatment characteristics. An earlier application of conjoint analysis for the treatment of upper limb function in SCI was published by Snoek et al.4
Choice-based conjoint (CBC) analysis, or discrete choice modeling, reveals trends in consumer preferences for competing products.14, 15 In a CBC, products are presented as bundles of attributes, presenting real as well as hypothetical product profiles. The analysis decomposes the resulting judgments into estimated individual-level part-worth utilities for the individual attributes. This study is innovative in its goal to reveal user preferences for devices in development. Eventually, an advanced appreciation of potential user preferences will improve the design of NPs to restore bladder function, which in turn will influence the acceptance of users toward these techniques.
Materials and methods
Setting up a CBC requires several subsequent analytical and design steps including attribute selection, design choice, and survey format.
Determination of attributes
NP options chosen for this study were pudendal nerve stimulation and sacral root stimulation with a dorsal rhizotomy (as used in the Brindley sacral anterior root stimulator) as well as sacral root stimulation with a rhizotomy alternative (rhizotomy-free Brindley), like high-frequency nerve blocks. The latter is still being developed. After surveying and interviewing patients, six attributes each having three levels were chosen to describe the NP alternatives. The final set of attributes was defined by the research team after consultation with physicians, researchers, and persons with SCI (Table 1).
Survey design
A fractional factorial study design was used for the survey and implemented with commercial software (Sawtooth Software, Sequim, Washington, USA). Taking into account level balance, utility balance, and orthogonality,16 the number of random scenarios was set to 14, which creates nearly perfect level balance and orthogonality. Two versions of a paper-and-pencil survey were made to minimize order effects. Each survey included 14 randomly generated choice sets and four fixed choice sets.
In addition to the 14 random scenarios, four-fixed scenarios were added to the survey. Three were added to directly compare the three potential NP solutions, thereby providing a measure of validity. The outcome of the direct comparison should result in a logical order of the potential NP solutions. In addition, the three fixed scenarios and an extra, fourth, fixed scenario were used to test for consistency. The latter compared an ‘ideal’ option to a ‘worst-case’ option, and the respondent had to choose the ‘ideal’ option to pass the consistency test.
Subject selection and sample size
Persons with SCI at least 6 months post-injury were recruited at the SCI outpatient clinic and inpatient acute rehabilitation programs at two Medical Centers (Metrohealth Medical System and Louis Stokes VA). Institutional review board approval was obtained at both sites, and informed consent was obtained before completing the survey. Also, all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. Required sample size was prospectively estimated to be 54.17
Patient interviewing
All patients were interviewed face-by-face except for eight subjects who returned the survey through mail. Before completing the survey, patients were informed about the experiment and the available treatment options. It was explained that voiding using a rhizotomy-free Brindley would be as good as a standard Brindley system. Only the degree of continence would be less.
Patients were then forced to pick one of the offered scenarios to obtain the maximum amount of information. However, each choice set was followed by an opt-out question to allow patients to withdraw from any treatment (Figure 1).

Example of a choice set including two scenarios and an opt-out question. Surveys were designed with 14 random choice sets.
Data analysis
Individual and utility weights were determined using a hierarchical Bayes modeling analysis. This method uses conditional probability to calculate part-worth utilities.18 Average utility weights were determined using multinominal aggregate logit model, which treats conjoint data as discrete choices, depending on sample characteristics, relative importance of attributes and personal preference (Sawtooth Software; https://www.sawtoothsoftware.com).
Responses from the three fixed scenarios of the direct comparison and the fixed comparison were evaluated. Subjects who failed both consistency tests were excluded from the analysis. Individuals who always chose no treatment demonstrated a dominant preference against NP and were analyzed separately. After obtaining part-worth utilities, the overall preference for each NP solution was determined, and described in the following equation:

Where the three types of NP were described using the six attributes.
The study was not designed to allow for subgroup analyses. However, in our analysis we did explore possible differences between complete and incomplete lesions as well as between para- and tetraplegics.
Results
In both medical centers, 90 people were ultimately approached to participate in the study. Nine people refused to participate and 81 people entered the study. Sixty-two of them were interviewed face-to-face and 19 surveys were taken home. Eight of 19 surveys taken home were completed and returned to the research office. However, four were dropped from further analysis because of inconsistencies. So, a total of 70 persons (78%) completed the survey, and 66 (73%) of these surveys were used for analysis.
The surveys on average took 40 min to complete. Subject demographics and characteristics of the 66 complete surveys analyzed are shown in Table 2. The subjects generally matched the national demographics.19 As expected, fewer women were recruited from the VA Medical Center.
Attribute and level weights
To visualize the relative preference for every individual level of all attributes, the levels were plotted on a scale from 0 to 1 (Figure 2). The level with the most positive part-worth utility (no side effects) was set at 1, and the level with the most negative part-worth utility (side effects due to rhizotomy) was set at 0. The range between the first and third level of the same attribute also gives insight in the weight of the attribute. Figure 2 shows that ‘Side effects’ had the greatest impact on the preference for a treatment, followed by the effects on continence and voiding.

Relative importance of each of the attributes obtained from the 53 patients that did consider treatment (that is non-dominant responders). High values indicate that the level is preferred, for example level 1 is the most preferable level and level 3 is the least preferable (see Table 1). The steeper the slope between levels and the larger the range, the higher is the relative importance of that attribute.
Explorative analysis did not show any remarkable differences in attribute weights between para- and tetraplegic patients. There seemed to be some difference between completely (N=17) and incompletely (N=36) paralysed patients. Voiding was valued higher in completely paralysed patients and restoring continence was valued higher in incompletely paralysed patients. However, given the limited number of patients, this difference should be interpreted with caution.
The relative importance of each attribute determined by the conjoint analysis is also shown in Table 3. Thirteen respondents were dominant against an NP. They also had significantly different preferences, for example they gave a higher weight to invasiveness of the procedure (0.30) than the non-dominant group (0.10). Their decision not to choose a treatment may therefore partly be explained by fear of surgery. As dominant responders would probably not choose an NP, all other analyses were done for the non-dominant respondents.
Direct comparison of NP options
The results of the direct comparisons of the chosen options are shown in Figure 3 and Table 4. In Figure 3, preferences of patients toward each of three NP options is predicted. In this study, the least preferred option is the Brindley system followed by the pudendal nerve stimulation. The most preferred system is a Brindley system that includes an alternative to the dorsal rhizotomy.

Preference for three separate neural prostheses. The figure is based on non-dominant patients only, and individual utility weights (Figure 2) are used to generate overall preferences. The figure is scaled using the least (Brindley) and most (Brindley and nerve block) preferred scenario.
The outcome of the direct comparison should result in a ranking of the NP (that is if Brindley without rhizotomy>pudendal nerve then Brindley without Rhizotomy>conventional Brindley). If the subject seems to have answered the questions randomly, this is considered inconsistent. Three (5.7%) of the 53 respondents failed the consistency test for this direct comparison. The rhizotomy-free Brindley choice was the most preferred option, followed by pudendal nerve afferent stimulation. The currently available Brindley device was chosen last in 56.6% of all cases. If we were interested in the market potential based on these comparisons, the rhizotomy-free Brindley would be preferred in 59.3% of the patients, the pudendal stimulation 37.4% and the current Brindley device only 3.3%. We may conclude that the overall outcome of the direct comparison equaled the outcome of the CBC.
Discussion
Earlier studies have shown that restoration of bladder function would be highly appreciated by people with SCI.2, 3 However, like in other examples of assistive technologies, the demand for interventions is not well correlated with the actual use.
A number of NP in development show potential; however, user preferences are needed to focus device design and development.
This study was the first to specifically investigate user preferences for NPs to restore bladder function, to support design choices in the development of new generations of NP. Survey research like CBC is increasingly being used in healthcare to evaluate acceptance of devices or services that are available, thereby determining the potential market for a product.
The advantage of confronting respondents with realistic scenarios in a CBC is that also more subtle differences in importance can be revealed, and trade-offs can be determined. These trade-offs would not have been obtained by using a numerical rating scale. In general, the findings in the CBC are consistent with what we know from interviewing patients and with the overall data provided in Table 4.
In this survey, we included 66 patients of whom two-thirds were not informed about the possibilities of NP. Thirteen patients (20%) did not choose any treatment involving implantation of neural electrodes. Reasons ranged from ‘afraid of surgery’ to ‘rather hoping that function will come back by itself’. This was also confirmed by the data in Table 3. It appears that the two attributes most affecting dominance were ‘side effects’ and ‘invasiveness’. Dominant respondents had fewer bladder problems (5.7% vs 15.4%), and were more likely to have had their injury for 1 year or less, or for >15 years (84.6% vs 52.8%). In the non-dominant individuals (80% of our sample), ‘side effects’ had the absolute highest relative importance (Figure 2; Table 3), followed by the device effectiveness measures ‘effect on continence’ and ‘effect on voiding’. All attributes had significant impact on overall preference, except for costs. Individuals weighed side effects or device effectiveness relatively greater than invasiveness. Therefore, device designs that require an invasive procedure have a large acceptance, as long as there are no severe side effects and bladder function is completely restored. Also, people with SCI generally have more problems with incontinence, than with using a catheter. That the difference between the most positive and intermediate level of ‘effect on continence’ was larger than that between the intermediate and third level implies that respondents highly appreciate even a minor positive effect on continence.
For 56.6% of the respondents, the Brindley system or sacral root stimulation with rhizotomy was the least preferred choice (Table 4). Obviously, this may be explained by the major side effects. However, it must be said that these side effects are not always relevant to all patients. In patients without sensation, reflex erections or reflex defaecation, this should not be considered a side effect as they do not loose anything. Actual choices made by patients may therefore differ from these group weights obtained from the experiment. Looking at the first and second choice, 48.9% of the respondents preferred the sacral root stimulation with an alternative for rhizotomy over pudendal nerve stimulation. So although rhizotomy was less preferred due to the side effects, people focused mainly on the effects on bladder function, and therefore chose to have a more invasive treatment with better effects.
The outcomes of the direct comparison and the random choice tasks (CBC data) both revealed that the side effects due to rhizotomy have the largest relative importance, followed by the effects on bladder function. This finding implies that the survey is valid. However, looking at the individual level, only 41.5% of the outcome of the direct comparison matches the CBC data of that individual. This can be explained as only three fixed choice sets were used in the direct comparison, compared with 14 random choice sets to obtain the CBC data.
The relative importance of ‘user friendliness’ and ‘cost to the user’ were relatively low. It also was not consistent with what was expected. The data suggest that respondents did not prefer to use an external device to operate the NP. However, the data should be interpreted with caution. One explanation for ‘cost’ being rated low is that the levels were not chosen appropriately and that a wider range of cost levels would have led to different results. The argument to include costs was that we intended to estimate the marginal value of additional R&D effort to develop a rhizotomy-free Brindley system. In other words, are patients prepared to pay out-of-pocket for next generation NPs. The levels for ‘costs’ were chosen based on a small preliminary sample of persons with SCI that were informed about the option to restore bladder function with an NP. It has to be concluded that these levels did not really force patients to consider costs as an important attribute. It also means that it is not possible to estimate the marginal value of device improvements.
As expected, this study revealed that persons with SCI would prefer a bladder NP with minimally invasive electrodes that gives them complete bladder function, with no side effects and that can be operated by pushing a button and they do not have to recharge themselves. Developing a ‘perfect’ device with all these characteristics is challenging.
Conclusion
CBC is a suitable method to measure user preferences of devices under development, revealing even subtle differences between levels using a relatively small sample size. These subtle differences would probably not have been revealed using a more straightforward 10-point scale rating method. As expected, this study revealed that the side effects of rhizotomy limit the clinical implementation of sacral root stimulation devices and that persons prefer a bladder NP with minimally invasive electrodes that gives them complete bladder function, with no side effects and that can be operated by pushing a button and they do not have to recharge themselves. Insight from these data will assist in the design and development of NP to restore bladder function for individuals with SCI.
References
Roach MJ, Frost F, Creasey G . Social and personal consequences of acquired bowel dysfunction for persons with spinal cord injury. J SCI Med 2000; 23: 263–269.
Anderson KD . Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma 2004; 21: 1371–1383.
Snoek GJ, IJzerman MJ, Post MW, Stiggelbout AM, Roach MJ, Zilvold G . Choice-based evaluation for the improvement of upper-extremity function compared with other impairments in tetraplegia. Arch Phys Med Rehabil 2005; 86: 1623–1630.
Snoek GJ, van Til JA, Krabbe PF, IJzerman MJ . Decision for reconstructive interventions of the upper limb in individuals with tetraplegia: the effect of treatment characteristics. Spinal Cord 2008; 46: 228–233.
Gaunt RA, Prochazka A . Transcutaneously coupled, high-frequency electrical stimulation of the pudendal nerve blocks external urethral sphincter contractions. Neurorehabil Neural Repair 2009; 23: 615–626.
Brindley GS . The first 500 patients with sacral anterior root stimulator implants: general description. Paraplegia 1994; 32: 795–805.
Wielink G, Essink-Bot ML, van Kerrebroeck PE, Rutten FF . Sacral rhizotomies and electrical bladder stimulation in spinal cord injury. 2. Cost-effectiveness and quality of life analysis. Dutch study group on sacral anterior root stimulation. Eur Urol 1997; 31: 441–446.
Creasey GH, Dahlberg JE . Economic consequences of an implanted neuroprosthesis for bladder and bowel management. Arch Phys Med Rehabil 2001; 82: 1520–1525.
Wenzel BJ, Boggs JW, Gustafson KJ, Grill WM . Closed loop electrical control of urinary continence. J Urol 2006; 175: 1559–1563.
Boggs JW, Wenzel BJ, Gustafson KJ, Grill WM . Frequency-dependent selection of reflexes by pudendal afferents in the cat. J Physiol 2006; 15: 115–126.
Bruns TM, Bhadra N, Gustafson KJ . stimulation of proximal urethral afferents improves bladder pressures and voiding. J Neural Eng 2009; 6: 66006.
Mariano TY, Bhadra N, Gustafson KJ . Suppression of reflex urethral responses by afferent stimulation in an acute spinalized feline model. Neurourol Urodyn 2010; 29: 494–500.
Boger A, Bhadra N, Gustafson KJ . Bladder voiding by combined high frequency electrical pudendal nerve block and sacral root stimulation. Neurourol Urodyn 2008; 27: 435–439.
Ryan M, Scott D, Reeves C, Bate A, van Teijlingen ER, Russell EM et al. Eliciting public preferences for health care: a systematic review of techniques. Health Technol Assess Rep 2001; 5: 1–186.
Lancsar E, Louviere J . Conducting discrete choice experiments to inform healthcare decision making: a user's guide. Pharmacoeconomics 2008; 26: 661–677.
Huber J, Zwerina K . The importance of utility balance in efficient choice designs. J Marketing Res 1996; 33: 307–317.
Orme B . Sample size issues for conjoint analysis studies. Sawtooth Software Inc 1998. Sequim.
Lenk PJ, DeSarbo WS, Green PE, Young MR . Hierarchical Bayes conjoint analysis: recovery of partworth heterogeneity from reduced experimental designs. Mark Sci 1996; 15: 173–191.
National Spinal Cord Injury Statistical Center. Spinal cord injury: facts and figures at a glance. https://www.nscisc.uab.edu// Birmingham, Alabama, 2008.
Acknowledgements
This work was supported by the NIH DK077089, NIDRR #H133N060017 and the Department of Veterans Affairs RR&D 3675R and B6685R. Special thanks to Melissa Schmitt, Nicola Ivanovic, Betty Dunger, Gregory Numunaitis, Melvin Mejia, Fred Frost, Denise Paulsen, Carol Sams and Jeanne Marlow for their assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Sanders, P., IJzerman, M., Roach, M. et al. Patient preferences for next generation neural prostheses to restore bladder function. Spinal Cord 49, 113–119 (2011). https://doi.org/10.1038/sc.2010.65
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.65
