
Abstract
Study design:
Clinical cohort study.
Objective:
To evaluate if the impact of the severity of the trauma as a possible confounding factor influences the neurological and functional recovery in paraplegia during the course of a 6-month follow-up period after injury.
Setting:
Spinal Cord Injury Center, Heidelberg University Hospital, Germany.
Methods:
A retrospective monocentric analysis, from 2002 to 2008, of the Heidelberg European Multicenter Study about spinal cord injury database was performed. We included 31 paraplegic patients (neurological level T1–T12) who were assigned either to a monotrauma (polytraumaschluessel (PTS) 1) or to a polytrauma (PTS⩾2) group. The American Spinal Injury Association Impairment Scale, lower extremity motor score, pin prick, light touch and the spinal cord independence measure (SCIM) were obtained at five distinct time points after trauma. Data were analyzed using Mann–Whitney U-test (α<0.05).
Results:
The changes in lower extremity motor score, pin prick and light touch showed no significant differences in both groups over the whole evaluation period. Polytraumatic paraplegics showed a significantly delayed increase of SCIM between 2 and 6 weeks compared with monotraumatic patients, followed by a quantitative increase in the subitems bladder management, bowel management, use of toilet and prevention of pressure sores between 3 and 6 months (P=0.031). The mean length of primary rehabilitation in the polytrauma group was 5.5 vs 3.6 months in monotrauma.
Conclusions:
The prognosis of polytraumatic paraplegics in terms of neurological recovery is not inferior to those with monotrauma. Multiple-injured patients need a prolonged hospital stay to reach the functional outcome of monotraumatic patients.
Similar content being viewed by others


Introduction
Statistical details report on polytrauma as the most common cause of death in people aged 45 years, with a peak at the age of 20 years.1 Injuries of thoracic vertebrae in multiple-trauma patients are often accompanied by severe thoracic injuries and sensorimotor deficits. Until now, the factor polytrauma, defined as injuries to other body systems in addition to spine injury,2, 3 has not been analyzed with regard to the neurological and functional status in traumatic paraplegia. Recently, spinal fractures in multiple-injured patients were analyzed based on the German Trauma Society's Trauma Register, which constitutes a prospective, standardized and anonymous documentation on severely injured patients. Out of 8057 patients 10% with severe spine trauma were identified, and of these 47% had neurological deficits at the date of injury.4 However, follow-up of these patients was not undertaken and, therefore, the dynamics of recovery in multiple-injured paraplegic patients remains still unclear.
Permanent damage of the central nervous system, caused by traumatic brain injury or a complete or incomplete injury of the spinal cord, results in long-term consequences with a high economic impact. Spinal cord injuries (SCIs) are devastating events for the patient and his environment. Further, clinical recovery after acute SCIis a multidimensional process. Therefore, the acquisition of functional and neurological data of SCI patients, as well as neurological and functional recovery, is of central importance for basic research in the long-term process.5 Pollard and Apple6 pointed out that the knowledge of specific factors in tetraplegic patients, which may be associated with neurological recovery, is essential in order to make any prognostic statement. Neurological recovery, defined by the American Spinal Injury Association (ASIA) Impairment Scale (AIS),7 can influence the functional status and consequently the rehabilitation outcome.5 The majority of outcome studies on patients with spine injuries focus mainly on the success of operative stabilization, clearance of the spinal canal or rapidity of the performed operation.8, 9 However, experimental and clinical studies have suggested that acute SCI is a two-step process involving primary and secondary mechanisms. Primary injury of the spinal cord refers to the initial mechanical damage by direct compression due to bone fragments or soft tissue causing damage of neural elements and blood vessels. The secondary mechanism follows the primary injury, including a cascade of biochemical and cellular processes extending throughout the initial lesion.10
The primary aim of our study was to evaluate if the impact of the severity of the trauma as a possible confounding factor influences the neurological and functional recovery in monotraumatic and polytraumatic SCI patients.
The second objective was to compare neurological and functional parameters in a group of paraplegic patients with an isolated vertebral fracture and with multiple injuries during the course of a 6-month follow-up period.
Materials and methods
This study was conducted at the Spinal Cord Injury Center (University Hospital Heidelberg, Germany) specialized in the acute management and rehabilitation of SCI patients. In the context of a multicenter study (European Multicenter Study about spinal cord injury, http://www.emsci.org),11 standardized data of neurological, neurophysiological and functional investigations are collected in acute SCI patients, with the intention to document spontaneous neurological recovery effects.12 Meanwhile, all acute SCI patients are documented by 18 European centers according to a standardized investigation protocol including the neurological examinations proposed by the ASIA.7
The purpose of this study is to establish a multicenter basis for future therapeutic interventions in human SCI. All subjects underwent acute care management and spine surgery (decompression and stabilization). Patients with acute SCI are tested and documented within a fixed time schedule after SCI and must comply with clearly defined inclusion and exclusion criteria. Inclusion criteria are traumatic or single-event ischemic paraplegia or tetraplegia, and a first set of assessments within the first 6 weeks after incidence. Exclusion criteria constitute—besides single-event ischemic—non-traumatic paraplegia or tetraplegia, neurological diseases or injuries other than SCI or reduced cooperation (for example, sedation and intubation). The collected data from each of the 18 centers are sent to the coordinating center into a central database, with the intention to plan and realize prospective studies investigating outcome measures, mechanisms of spontaneous recovery or the efficiency of new treatment strategies. The ASIA examinations were performed by two trained ASIA experts in order to minimize inter-rater reliability.
The ASIA assessment protocol consists of two sensory examinations, a motor examination and a classification framework (the impairment scale) to quantify the severity of the SCI.
The SCI database of the center of Heidelberg (n=330, acquisition period in relation to date of injury from 2002 to 2008, including traumatic and non-traumatic SCI patients) has been used for further analysis. Out of a total of 154 traumatic SCI patients, 91 were tetraplegic and 63 were paraplegic, with a neurological level between Th1 and Th12. Inclusion criteria constituted traumatic, early surgically (<24 and 24–72 h) treated paraplegic patients with a neurological level between Th1 and Th12. Further, patients with multiple injuries to other body systems, including a thoracic spine fracture, or paraplegic patients with an isolated vertebral fracture (Th1–Th12) and with a complete neurological and functional follow-up at least over 6 months were included. Patients over 60 years suffering from neurological (for example, traumatic brain injury and epilepsy) or psychiatric diseases resulting in non-reliable results were excluded.
A total of 31 paraplegic patients (neurological level T1–T12) were assigned according to the polytraumaschluessel (PTS)13 either to a monotrauma (PTS=1, n=10) or to a polytrauma (PTS⩾2, n=21) group. The PTS,13 which represents a validated classification tool in multiple-injured patients, was used due to its simple handling and the retrospectively comparable reliability with the injury severity score.14 This quantitative scoring system categorizes the degree of injury of the five body regions: cranium (polytraumaschluessel subitem Schädel, PTSS), thorax (polytraumaschluessel subitem thorax), abdomen (polytraumaschluessel subitem Abdomen, PTSA), extremities (polytraumaschluessel subitem Extremitäten, PTSE), pelvis/spine (polytraumaschluessel subitem Becken/Wirbelsäule, PTSB), and includes additionally the age of the patient. The summation of point values of each body region after finishing diagnostic investigations provides information about the severity of sustained injuries and patients’ prognosis.13
Radiological documents of the patients were reviewed by a blinded examiner (TG) and the fracture classified among the Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification.15 Compression fractures were classified as AO type A fractures, flexion/distraction fractures as AO type B and rotational instable fractures as AO type C fractures. Additionally to the European Multicenter Study about spinal cord injury protocol, the PTS and the AO classification were assessed in all included patients in order to define the severity of trauma and the type of fracture.
The AIS, lower extremity motor score, pin prick, light touch and the spinal cord independence measure (SCIM)16 were obtained at five distinct time points (2 weeks, 4–6 weeks, 3 months, 6 months and 1 year after SCI) after trauma according to the European Multicenter Study about spinal cord injury protocol. The SCIM16 is at present the only comprehensive rating scale that measures the ability of patients with spinal cord lesions to perform everyday tasks. The SCIM includes three subscales: self-care (subscore 0–20), respiration and sphincter management (subscore 0–40) and mobility (subscore 0–40). The total score ranges from 0 to 100.
Data were analyzed using SPSS 15.0 (SPSS, Chicago, IL, USA). Standard deviation (s.d.) was shown as plus or minus (±). Differences between groups, were analyzed by the non-parametric Mann–Whitney U-test. The level of significance was assigned at 5%.
Results
Patient characteristics
Extraction from the database resulted in a sample of 31 paraplegic patients with a thoracic spine fracture and paraplegia, 24 male and 7 female patients, who were rehabilitated between 2002 and 2008 at the Spinal Cord Injury Center (University Hospital Heidelberg, Heidelberg, Germany) after operative stabilization in a primary trauma center. The admission from the trauma center to the spinal cord injury center was realized during the first 2 weeks after injury. The stabilization of the spinal column was mainly performed during the first and third days after injury. All patients received decompression of the spinal cord. Dorsal stabilization was the mainly performed operative procedure in 24 patients. The last follow-up examination was in December 2008. The average age of patients was 33±12.5 (15–52) years; whereas no comorbidities were present in 23 patients, diabetes without polyneuropathy (n=3), hepatitis B (n=2), cardiovascular disease (n=1), gastroduodenal disease (n=1) and hypophysis insufficiency (n=1) were documented in 8 patients. The PTS in all patients had a mean of 29±9.4 points (interval: 16–46 points) and the PTST, a variable of the PTS for the thorax, had a mean of 12±5.6 points. Patient characteristics after being assigned to either the monotrauma (PTS=1, n=10) or the polytrauma (PTS⩾2, n=21) group are shown in Table 1.
Mechanism of injury
The most common cause of accident mechanism was traffic accident in 23 (74%), whereby 5 patients (16%) had an accident as drivers and 6 patients (19%) as front seat passengers. Further, 9 patients (29%) suffered injury from motorcycle accident and 3 patients (10%) from bicycle accident. A fall from heights ⩾3 m occurred in 3 patients (10%) and a fall from heights <3 m in 4 patients (13%). Ski accident was the cause of spine fracture and paraplegia in 1 (3%) patient (Figure 1).

Accident mechanisms of the examined polytraumatic and monotraumatic patients with paraplegia.
Neurological recovery
Complete neurological follow-up included a 6-month follow-up period in the polytrauma and monotrauma groups. Additionally, polytrauma SCI patients had their latest follow-up examination 1 year after injury. The changes in the AIS at 2–4 weeks (first examination) and at 6 months or 1 year (last examination) after polytrauma and monotrauma revealed an approximately similar distribution of complete paraplegia. In all, 6 (60%) patients of the monotraumatic group compared with 14 (67%) patients of the polytraumatic group showed complete paraplegia that persisted after this period. This distribution of ASIA A patients was shown in both groups (Figure 2) to be independent of the severity of fracture. The changes in lower extremity motor score, pin prick and light touch (Figures 3 and 4) showed no significant differences in both groups over the whole evaluation period (P>0.05).

Changes in the AIS at the first examination (2–4 weeks) and latest examination (6 months or 1 year) after accident in polytrauma and monotrauma.

(a) Course of lower extremity motor score (LEMS) within 1 year in polytraumatic paraplegic patients. (b) Course of LEMS within 6 months in monotraumatic paraplegic patients (p00=minimum, p25=25% percentile, p50=median, p75=75% percentile, p100=maximum and n=number of the patients). p00, p25 and the median were all located at baseline because 50% of the patients had zero points in the LEMS.

(a–d) Course of light touch (LT) and pin prick (PP) within 1 year in polytraumatic paraplegic patients and within 6 months in monotraumatic spinal cord injured patients (p00=minimum, p25=25% percentile, p50=median, p75=75% percentile, p100=maximum and n=number of the patients).
Functional recovery
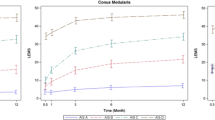
Between 3 and 6 months the SCIM revealed significant differences (P=0.031), but almost the same SCIM score was reached in the monotrauma group at 6 months (75.7±19.2) and in the polytrauma group at 1 year (71.2±12.3) after the trauma (Figure 5). Polytraumatic paraplegics showed a significantly delayed increase of SCIM between 2 and 6 weeks, revealed a higher functional gain between 3 and 6 months, and had a longer mean length of primary rehabilitation (5.5 (±2.1) vs 3.6 (±2.1) months), when compared with monotraumatic paraplegics. The difference of means revealed a quantitative increase in the subitems bladder management, bowel management, use of toilet and prevention of pressure sores in the polytrauma compared with the monotrauma group. Patients who had assisted intermittent catheterization and a residual urine volume of >100 ml were able to handle intermittent self-catheterization between 3 and 6 months. Irregular timing of bowel movements improved to regular bowel movements with and without assistance. Further, patients were able to use the toilet independently with and without adaptive devices, and they were independently in bed mobility, which prevents pressure sores (Table 2).

(a, b) Course of spinal cord independence measure II (SCIM II) within 1 year in polytraumatic paraplegic patients and within 6 months in monotraumatic spinal cord injured patients (p00=minimum, p25=25% percentile, p50=median, p75=75% percentile, p100=maximum and n=number of the patients).
Discussion
The AO classification is useful in correlating fracture type with the frequency of neurological deficits. Madert and Eggers17 report on neurological deficits, representing only 1% in compression fractures (type A) and 17% in rotatory instable C fractures.
The present study confirmed the hypothesis that the severity of spinal fracture, represented by the AO classification, does not go along with a higher incidence of complete and persisting paraplegia in the polytrauma group.
We found a similar distribution of complete paraplegia, 60% in the monotraumatic and 67% in the polytraumatic paraplegics during the course of a 6–12-month evaluation period. Therefore, polytrauma is not a confounding factor in terms of neurological recovery. However, Hebert et al.2 have shown that spinal trauma is the major contributor to persistent disability measured by functional independence measure.18 Further, poorer short- and long-term outcomes were found in patients with traumatic spine injury and polytrauma. In accordance with our study, average age and cause of injury were similar and a greater length of rehabilitation was documented in polytraumatic patients with spinal fractures. In their study population, 64.7% had no neural injury and the remainder had some degree of neurological impairment. A negative correlation between the injury severity score and the lower extremity motor score on admission was found at the time of injury. Unfortunately, no sensible examination, ASIA classification or further neurological follow-up was performed. For this reason, the process of neurological recovery remains uncertain in this collective.
The neurological course of multiple-injured patients and monotraumatic spinal cord injured patients is so far not yet evaluated. From our data we can conclude that all patients who had a C fracture and an AIS A did not show any neurological improvement during 1 year.
A weak point of our study is the absence of preoperative ASIA investigations from the trauma centers. However, it is a common problem that multiple-injured patients are often not adequately examinable due to intubation, traumatic brain injury or sedation. The main injured part of our patients was operated between 0 and 3 days after injury. For this reason, confounding factors such as time interval between injury and operation or surgical intervention were not included in the analysis.
Further, the AIS classification is highly influenced by factors that influence the reliability of scoring sacral segments, for example, assessment of anal sensation.19 As anal sensation disappeared between the first and the second assessment post injury, one patient regressed from AIS B to AIS A and remained AIS A until the last assessment (Figure 2). Two patients converted from AIS A to AIS B and to AIS C. Spiess et al.19 pointed out that ‘a change in the sacral segments is a prerequisite for a change from AIS A to AIS B and vice versa’.
In analyzing the effects of neurological medications, spontaneous conversion of complete to incomplete paraplegia must be strictly separated from pharmacological effects. Though the sample size of our groups is small, our results suggest that the factor polytrauma does not seem to impede neurological recovery. However, further research in a larger patient group is necessary to confirm this statement.
The PTS was used to split the groups into monotraumatic patients with paraplegia and an isolated vertebral fracture, and polytraumatic paraplegics. In its original form, due to anatomical orientation the PTS is practical, transparent and easily calculated.20 The judgement of the examiner can affect the evaluation of the injury of individual body regions strongly and a precise objective anatomical evaluation is preferable.21 Teijink et al.14 proved that the injury severity score compared with the PTS retrospectively showed no better reliability.
It is important to acknowledge that neurological recovery does not always produce sufficient functional gain. Therefore, functional outcome measures, such as the SCIM, were developed specifically for SCI patients and validated as an important tool to measure quantitative functional recovery.16
We showed that between 3 and 6 months the SCIM revealed significant differences (P=0.031) in polytraumatic paraplegics compared with their counterparts. This reveals the importance of rehabilitation in multiple-injured patients with paraplegia to reach the maximum quantitative increase in learning self-catheterization, bowel management, use of toilet and prevention of pressure sores. A positive consequence could be a decrease of re-hospitalization, an increased independence in daily life activities or psychological factors.
Conclusions
Our results suggest that the prognosis of polytraumatic paraplegics in terms of neurological recovery is not inferior to those with monotrauma. Multiple-injured patients need a prolonged hospital stay to reach the functional outcome of monotraumatic patients.
References
Champion HR, Copes WS, Sacco WJ, Lawnick MM, Keast SL, Bain Jr LW et al. The major trauma outcome study: establishing national norms for trauma care. J Trauma 1990; 30: 1356–1365.
Hebert JS, Burnham RS . The effect of polytrauma in persons with traumatic spine injury. A prospective database of spine fractures. Spine 2000; 25: 55–60.
Blauth M, Knop C, Bastian L, Krettek C, Lange U . Complex injuries of the spine. Orthopäde 1998; 27: 17–31.
Schinkel C, Frangen TM, Kmetic A, Andress HJ, Muhr G, AG Polytrauma der DGU . Spinal fractures in multiply injured patients: an analysis of the German Trauma Society's Trauma Register. Unfallchirurg 2007; 110: 946–952.
Curt A . Neurologische und funktionelle Erholung nach Querschnittlähmung. Verlaufs- und Beurteilungsstandards in der Paraplegiologie. Orthopäde 2005; 34: 106–112.
Pollard ME, Apple DF . Factors associated with improved neurological outcomes in patients with incomplete tetraplegia. Spine 2003; 28: 33–38.
Marino RJ . International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association: Chicago, 2000.
Boerger TO, Limb D, Dickson RA . Does ‘canal clearance’ affect neurological outcome after thoracolumbar burst fractures? J Bone Joint Surg Br 2000; 82: 629–635.
Rahimi-Movaghar V . Efficacy of surgical decompression in the setting of complete thoracic spinal cord injury. J Spinal Cord Med 2005; 28: 415–420.
Ambrozaitis KV, Ambrozaitis KV, Spakauskas B, Vaitkaitis D . Pathophysiology of acute spinal cord injury. Medicina (Kaunas) 2006; 42: 255–261.
Curt A, Van Hedel HJ, Klaus D, Dietz V, EM-SCI Study Group. Recovery from a spinal cord injury: significance of compensation, neural plasticity, and repair. J Neurotrauma 2008; 25: 677–685.
Curt A, Schwab ME, Dietz V . Providing the clinical basis for new interventional therapies: refined diagnosis and assessment of recovery after spinal cord injury. Spinal Cord 2004; 42: 1–6.
Oestern HJ, Tscherne H, Sturm J, Nerlich M . Klassifizierung der Verletzungsschwere. Unfallchirurg 1985; 88: 465–472.
Teijink JA, Dwars BJ, Patka P, Haarman HJ . Scoring multitrauma patients: which scoring system? Injury 1993; 24: 13–16.
Magerl F, Aebi M, Gertzbein SB, Harms J, Nazarian S . A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 1994; 3: 184–201.
Catz A, Itzkovich M . Spinal cord independence measure: comprehensive ability rating scale for the spinal cord lesion patient. J Rehabil Res Dev 2007; 44: 65–68.
Madert J, Eggers C . Strategy for managing injuries of the thoracic spine T1–11. Trauma Berufskrankh 2007; 9: 231–236.
van der Putten JJMF, Hobart JC, Freeman JA, Thompson AJ . Measuring change in disability after inpatient rehabilitation: comparison of the responsiveness of the Barthel Index and the Functional Independence Measure. J Neurol, Neurosurg Psychiatry 1999; 66: 480–484.
Spiess MR, Müller RM, Rupp R, Schuld C, van Hedel HJ, EM-SCI Study Group. Conversion in ASIA Impairment Scale during the first year after traumatic spinal cord injury. J Neurotrauma 2009; 26: 2027–2036.
Oestern HJ, Kabus K, Neumann C . Der Hannoversche Polytraumaschlüssel. Hefte zu Unfallheilkunde 1991; 220: 210–215.
Oestern HJ, Kabus K . Comparison of different trauma scoring systems. A review. Unfallchirurg 1994; 97: 177–184.
Acknowledgements
We thank Mrs S Gantz for her statistical support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Putz, C., Schuld, C., Gantz, S. et al. The effect of polytrauma as a possible confounder in the outcome of monotraumatic vs polytraumatic paraplegic patients: a clinical cohort study. Spinal Cord 49, 721–727 (2011). https://doi.org/10.1038/sc.2010.181
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.181
Keywords
This article is cited by
-
Observational study of the effectiveness of spinal cord injury rehabilitation using the Spinal Cord Injury-Ability Realization Measurement Index
Spinal Cord (2016)
-
Impact of multiple injuries on functional and neurological outcomes of patients with spinal cord injury
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2013)
