
Abstract
Background:
Traumatic spinal-cord herniation after nerve root avulsion is rare. We report on the first patient with spinal-cord herniation associated with pseudomeningocele in the lower conus medullaris region after nerve avulsion.
Case:
This 72-year-old man presented with progressive pain in the left leg and motor weakness after two traumatic accidents. Constructive interference in steady-state (CISS) imaging showed the attachment of the spinal cord to the wall of a herniated pseudomeningocele and associated syringomyelia at the level of T12. At the time of surgery, a herniated pseudomeningocele was observed. The lateral portion of the spinal cord that had herniated into the pseudomeningocele was detached from its wall; this was followed by repair of the dural defect. A redundant nerve root was observed inside the pseudomeningocele, suggesting nerve root avulsion as the primary lesion. To facilitate cerebrospinal fluid drainage from the syringomyelia, we next performed dorsal root entry zone (DREZ)tomy to the pseudomeningocele. Postoperatively, he manifested significant clinical improvement.
Conclusions:
This is the first report of spinal cord herniation after nerve root avulsion in the conus medullaris region. CISS imaging is highly useful for the demonstration of spinal cord herniation, syringomyelia and pseudomeningocele. To restore neurological function in patients with progressive symptoms, we recommend surgical treatment.
Similar content being viewed by others


Introduction
Spinal cord herniation is a rare but well-documented entity, which results in various neurological symptoms. It is classified as idiopathic, iatrogenic and traumatic. Traumatic spinal-cord herniation is less well documented in the literature.1, 2 Among the 13 cases of traumatic spinal-cord herniation reported earlier, only three were associated with nerve root injury;1 all patients manifested brachial plexus injury.
To our knowledge, there have been no reports of traumatic spinal-cord herniation associated with pseudomeningocele in the conus medullaris region. Here we report on a patient with traumatic spinal-cord herniation after lower-thoracic nerve-root avulsion.
Case report
Thirty years earlier, this 72-year-old patient had a rear-end collision by a motor car when he was driving his car, wherein he twisted his trunk resulting in numbness and radiating pain on his left side. He consulted his physician and was treated conservatively, which gradually increased his leg pain. In the second car accident, he received a strong side-impact collision by a motor car, and severely twisted his thigh and leg, resulting in backache and severe radiating pain on his left thigh and leg. This history suggests a left thoracic nerve-root and spinal-cord injury resulting from the first accident, and a deterioration involving left-lumbar nerve irritation after the second accident. When he was hospitalized at our institute, his chief complaint was increasing radiating pain in his left side with spastic gait. We noted motor weakness (manual muscle test: iliopsoas 4/5, extensor hall. br. 1/5) restricted to his left lower extremity. There was no motor weakness in his upper extremity and right lower extremity. In the left knee, deep-tendon reflex had diminished, whereas it had increased during the left-ankle deep-tendon test and was normal on the right side. The plantar reflex on his left side was positive. Temperature and pinprick responses were decreased below T12; there was hypalgesia below L1 on the left side. Magnetic resonance imaging (MRI) showed a herniated pseudomeningocele and a syringomyelia at the T11/12 level (Figure 1). To show neural structures with increased sensitivity, we used constructive interference in steady-state (CISS) imaging.3, 4 CISS image minimizes the pulsatile cerebrospinal fluid (CSF) by acquiring the sequence with flow compensation applied over each transgressive–regressive cycle (T–R cycle), resulting in a higher intrinsic resolution between neural structures, CSF and lesions surrounded by CSF. In this case, CISS images well demonstrated the attachment of the spinal cord to the wall of a herniated pseudomeningocele; there was a root fiber exiting from the syringomyelia into the herniated pseudomeningocele (Figure 2). On the basis of these preoperative findings, we decided to perform a surgery.

Preoperative magnetic resonance (MR) images ((a) Sagittal T1 weighted, (b) Sagittal T2 weighted) showed syringomyelia at the T11/12 level. Postoperative MR images ((c) Sagittal T1 weighted, (d) Sagittal T2 weighted) showed disappearance of the syringomyelia.

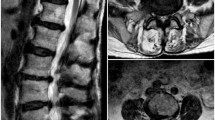
(a) Coronal construction interference in steady-state (CISS) images showing syringomyelia, pseudomeningocele and herniation of the spinal cord into the pseudomeningocele. (b) Axial CISS images show spinal cord herniation and pseudomeningocele.
Laminectomy from T11 to T12 revealed a herniated pseudomeningocele adjacent to the T11/12 facet joint. After opening the dura and arachnoid, we noted that the spinal cord was tightly attached to a pale, thick arachnoid tissue inside the herniated pseudomeningocele. The spinal cord was dissected and pulled back into the intradural space (Figure 3). We opened the pseudomeningocele by longitudinal incision. This revealed redundant nerve roots within granulomatous tissue, suggesting nerve root avulsion as the primary lesion. We addressed the swollen spinal cord by 3-mm dorsal root entry zone (DREZ)tomy; this facilitated cerebrospinal fluid (CSF) drainage from the syringomyelia and resulted in the collapse of the syrinx. The involved nerve roots exited from the syringomyelia (Figure 3). A fascia graft was sutured to the dural defect and the area was covered with a patch sprayed with fibrin glue. Pathological examination of the removed arachnoid tissue disclosed hyalinization.

Intraoperative photographs. (a) Before opening the dura, a herniated pseudomeningocele was observed adjacent to the T11/12 facet joints. (b) After opening the dura and the arachnoid, the herniated spinal cord was dissected and pulled back into the intradural space. Note the dural defect.
Postoperative MRI confirmed the disappearance of the cord deviation and intramedullary cyst (Figure 1). Although motor function was remarkably improved, he reported intermittent radiating pain for 6 weeks after surgery; at 10 weeks, it had decreased significantly. At the final observation 1 year after surgery, he had slight numbness in his left thigh without motor dysfunction.
Discussion
Spinal cord herniation is relatively rare; to our knowledge, only 110 cases have been reported to date. Traumatic spinal-cord herniation is extremely rare; our search of the literature disclosed only 13 cases reported earlier.1, 2, 5 Although the etiology of spinal cord herniation remains to be established, in most patients with the idiopathic variation the affected levels range between T4 and T7. In patients with traumatic spinal-cord herniation, there was an association with the site of injury.5 Although most earlier reported patients with traumatic spinal-cord herniation manifested deficits in the ventral or ventrolateral dura mater with tethering of the spinal cord to the dorsal aspect of adjacent vertebrae, dorsolateral spinal-cord herniation was identified in only two, including our patient.
Among the 13 patients reported earlier with traumatic spinal cord herniation, only three were associated with nerve root injury; in all, there was an association with brachial plexus injury. Ours is the first case, in which nerve root injury was associated with a site other than the brachial plexus.
CISS imaging was highly useful for the demonstration of spinal cord herniation, syringomyelia and pseudomeningocele. The sensitivity of CISS sequence is increased in neural tissues because the T2 values between the CSF and other structures are attenuated, resulting in a higher resolution of CISS images of neural structures. According to the preoperative CISS information, we performed surgical treatment, resulting in clinical improvement.
References
DaSilva VR, Al-Gahtany M, Midha R, Sarma D, Cooper P . Upper thoracic spinal cord herniation after traumatic nerve root avulsion. J Neurosurg 2003; 99: 306–309.
Francis D, Batchelor P, Gates P . Posttraumatic spinal cord herniation. J Clin Neurosci 2006; 13: 582–586.
Ikushima I, Korogi Y, Hirai T, Yamashita Y . High-resolution constructive interference in a steady state imaging of cervicothoracic adhesive arachnoiditis. Neuroradiol Comp Assist Tomograph 2007; 31: 143–147.
Ramli N, Cooper A, Jaspan T . High resolution CISS imaging of the spine. Br J Radiol 2001; 74: 862–873.
Yokota H, Yokoyama K, Noguchi H, Uchiyama Y . Spinal cord herniation into associated pseudomeningocele after brachial plexus avulsion injury: case report. Neurosurgery 2007; 60: E205.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ijiri, K., Hida, K., Yano, S. et al. Traumatic spinal-cord herniation associated with pseudomeningocele after lower-thoracic nerve-root avulsion. Spinal Cord 47, 829–831 (2009). https://doi.org/10.1038/sc.2009.38
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2009.38
Keywords
This article is cited by
-
Spinal cord herniation following cervical meningioma excision: a rare clinical entity and review of literature
European Spine Journal (2016)
