
Abstract
Study design:
Experimental rat study.
Objective:
To investigate changes in motor unit number estimation (MUNE) value of the medial gastrocnemius (MG) muscle after thoracic spinal cord transection in rats and to correlate the MUNE with hindlimb motor function recovery.
Setting:
China Rehabilitation Research Center, Beijing, China.
Methods:
Twelve rats were subjected to spinal cord transection or sham surgery and then evaluated by MUNE and the Basso, Beattie and Bresnahan (BBB) behavioral scale 56 days after the surgery.
Results:
The MUNE values of the MG muscle were significantly decreased from baseline at 14–49 days after surgery. However, they returned to near pre-injury levels after 56 days. Rats recovered progressively from the severely impaired hindlimb motor function induced by spinal cord injury, as indicated by a gradual increase in BBB score during days 3–49 after surgery. However, this behavioral recovery was only partial and reached a plateau on day 49. Finally, there was a U-shape-like correlation between changes in MUNE values and BBB scores after thoracic spinal cord transection.
Conclusions:
Time-dependent changes in the functional motor unit number may occur in spinal segments caudal to the transection level, and MUNE could be a useful method to evaluate motor function recovery.
Similar content being viewed by others

Introduction
Spinal cord injury (SCI) leads to acute functional defects and numerous chronic neurological alterations distal to the site of lesion. Some previous studies1, 2, 3 have suggested that these changes may be associated with neurological plasticity or functional reorganization of intrinsic spinal cord circuitry after SCI, whereas others4 have proposed that trans-synaptic degeneration may also be involved. Neuronal structural and/or functional changes caudal to SCI may contribute to the failure of neurological regeneration and reorganization.
Since motor unit number estimation (MUNE) was first introduced by McComas et al.5 in the early 1970s, it has become a useful electrophysiological method for quantitatively measuring the number of functional lower motor neurons.6 For diseases such as amyotrophic lateral sclerosis, which affects the anterior horn cells, MUNE has been suggested to be a sensitive and reliable follow-up tool for detecting physiological events that are associated with disease progression in both patients and animal models.7, 8 However, no MUNE study has been carried out in an animal model of SCI. The goal of our study was to examine changes in MUNE values of the medial gastrocnemius (MG) muscle after thoracic spinal cord transection in rats and determine whether these changes are associated with motor function recovery caudal to the level of SCI.
Materials and methods
Animals
Experiments were conducted on 12 adult (250–300 g) female Sprague–Dawley rats. Rats were housed individually, with food and water provided ad libitum, and kept on a 12-h light–dark cycle. We certify that all applicable institutional and governmental regulations concerning the ethical use of animals were followed during the course of this research.
Thoracic spinal cord transection
Rats were anesthetized using chloral hydrate (360 mg kg−1, intraperitoneally), and a laminectomy was performed at T8 vertebra to remove the vertebral bone overlying the spinal cord, exposing a circle of dura. The spinal column was stabilized by clamping the T7 and T9 vertebrae. Then, irridectomy scissors were used to completely transect the spinal cord at T8, and gel foam was placed into the lesion site. Age-, sex-, and weight-matched controls were only laminectomized. After the surgery, bladders of the rats were manually expressed twice daily until it was no longer necessary, and oral antibiotics were given in cases of suspected urinary tract or bladder infection. Rats were assigned to different groups through a randomized block design.
Behavioral analysis
The Basso, Beattie and Bresnahan9 (BBB) scale is a neurological rating scale that quantifies the use of hindlimbs in open field locomotion after SCI. The scores range from 0 (complete hindlimb paralysis) to 21 (normal hindlimb locomotion). Rats were tested weekly according to this scale until they were killed.
MUNE methods
Electrophysiological measurements were performed weekly by a standard two-channel electrophysiological stimulation and recording device (Nihon Kohden, Tokyo, Japan). M-potential was recorded from the MG muscles, with the active needle electrode (30-gauge) inserted into the middle part of the muscle, perpendicular to the long axis. The reference electrode and the ground electrode were inserted subcutaneously on the Achilles tendon and the back, respectively. surface-represented motor unit action potentials (S-MUAPs) and compound motor action potentials were recorded with a gain of 100–200 μV per division and were evoked by 0.01-ms constant current square waves repeated at 0.7 Hz, as proposed by Wang and Delwaide.8 Recordings were filtered with a bandpass from 30 Hz to 3 kHz. The increments of stimulus intensity were 0.2 mA.
The amplified multiple points stimulation method and associated algorithms have been described previously.10, 11 The compound muscle action potential of the MG muscle was obtained using a supramaximal stimulation (20–25% above the maximal intensity).12, 13 The cathode of the stimulating electrodes was inserted subcutaneously close to the sciatic nerve at the proximal thigh, and the anode was placed subcutaneously 1 cm proximally. Individual motor unit responses were obtained by adjusting the stimulating electrode and isolating threshold responses with distinct morphologies. Given the small size of the animals, the area of potential stimulation was restricted from the proximal thigh to the popliteal fossa, but three to five stimulation sites could usually be studied in each animal. At each stimulation site, the stimulus intensity was increased by increments to the level at which the first and then the second, and sometimes the third subsequent S-MUAPs were elicited in an all-or-nothing manner. Peak-to-peak amplitudes were determined for each S-MUAP and then averaged to yield the mean S-MUAP amplitude. The MUNE value was estimated by dividing the amplitude of the maximal compound motor action potential by the averaged amplitude of S-MUAP.
Statistics
Data are presented as mean±s.d. Statistical analysis was performed using paired t-tests, one-way analysis of variance, and the Pearson correlation coefficient. The level of significance was set at P<0.05.
Results
Recovery of the hindlimb motor function after thoracic spinal cord transection
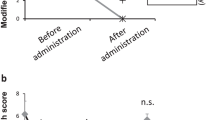
All transected rats showed a dramatic decrease in BBB score (from 21/21 to ⩽1/21) in both hindlimbs at 3 days after surgery, confirming the expected behavioral deficit after a complete thoracic spinal cord transection. The rats experienced a partial recovery of hindlimb motor function over time, as indicated by the progressive increase in BBB scores measured from days 3 to 56 after surgery (Figure 1). Sham surgery controls did not have any functional deficits, as indicated by a BBB score of 21/21. In the group maintained for 56 days, the BBB scores measured at 3, 7, 14, 21, 28, 35 and 42 days after surgery were significantly less than that measured at 49 days (P=0.000–0.027), suggesting significant hindlimb motor function recovery by 49 days. The hindlimb motor function recovered quickly within the first 2 weeks after injury, as indicated by significant differences in BBB scores between 3 and 7 days, and between 7 and 14 days (P=0.043 and 0.025, respectively). No additional increase in BBB score was observed at 42 days, as compared with the score at 56 days. (P=0.058), indicating that the partial recovery of hindlimb motor function may reach a plateau level. All transected rats were able to move two or three joints of the hindlimbs without weight support by 56 days after surgery.

Time-dependent changes in Basso, Beattie and Bresnahan (BBB) scores after thoracic spinal cord transection in rats of the 56-day group. Rats showed a dramatic decrease in BBB score 3 days after thoracic spinal cord transection. However, rats displayed a progressive recovery of their hindlimb motor function between days 3 and 35 after surgery (*P=0.000–0.027, vs day 56). Recovery reached a plateau at 42 days, with no further significant improvement in function (day 42 vs day 56, P=0.058). The hindlimb motor function recovered most notably within the first 2 weeks after injury, as indicated by significant differences in BBB scores between 3 and 7 days, and between 7 and 14 days (#P=0.043 and 0.025, respectively).
Changes in MUNE values of the MG muscle after thoracic spinal cord transection
The changes in MUNE values over time after spinal cord transection took on a U-shape appearance during the period studied. In the group of rats maintained for 56 days, the MUNE value of the MG muscle decreased initially and was significantly lower than that of baseline from day 14 to day 28 after surgery (P<0.01; Figure 2). The value reached an apparent minimum at 28 days and then progressively recovered to near a pre-injury level by 56 days (P=0.065 vs pre-injury value).

The biphasic change in motor unit number estimation (MUNE) values after thoracic spinal cord transection in rats. In rats that were maintained for 56 days, the mean MUNE value of the medial gastrocnemius muscle decreased progressively from day 14 to day 28 after surgery. The decrease in MUNE value apparently reached a lower plateau at 28 days, after which it gradually recovered to near pre-injury level by 56 days. (*P=0.000–0.001 vs pre-injury value).
Correlation between changes in MUNE and hindlimb motor function recovery after SCI
Finally, we determined whether alterations in MUNE values of the MG muscle correlate with hindlimb motor function recovery after thoracic spinal cord injury. Statistical analysis of data from the rat group maintained for 56 days indicated that the relationship between changes in MUNE values and BBB scores after SCI formed a U-shaped curve (P<0.001; Figure 3).

Correlation between changes in MUNE values and the recovery of hindlimb motor function, as assessed by the Basso, Beattie and Bresnahan (BBB) behavioral scale. In the group of rats maintained for 56 days, statistical analysis suggests a U-shaped relationship between MUNE values and BBB scores after thoracic spinal cord transection in rats (P<0.001).
Discussion
In this study, we found that the changes in MUNE values of the MG muscle after thoracic spinal cord transection in rats followed a U-shaped curve over time. In the group of rats maintained for 56 days, the preoperative MUNE value was 127±15. After surgery, this value decreased over time, reached a minimum at 28 days, and then gradually recovered until at 56 days, the MUNE value was not significantly different from baseline. The study by Kudo and Yamada14 showed that the estimated number of MG motor neurons retrogradely labeled with horseradish peroxidase was approximately 125 in adult rat. The MUNE value from the rat MG muscle was reported14 to be 109±3 on the basis of the electromyography method. The similarity of these values to our baseline MUNE value confirms that amplified multiple points stimulation is a valid method for MUNE measurement. A study that used incremental and multipoint MUNE methods in a transgenic mouse model of the lower motor neuron disease amyotrophic lateral sclerosis yielded similar results.8
There is increasing evidence for degradation of neuronal function below the level of lesion in chronic, complete SCI.15 The initial decrease in MUNE value by day 28 post-surgery in this study indicates a loss of functional motor units distal to the site of lesion during this time period. Consistent with this finding, the number of soleus motoneurons, identified by retrograde labeling with unconjugated cholera toxin B, showed a 16% decrease at 4 months after midthoracic spinal cord injury in rats.4 Cell loss or trans-synaptic degeneration has been suggested as a potential mechanism underlying the decrease in this medium-size motor neuron population. For example, a previous study showed trans-synaptic degeneration of the anterior horn motor neurons in spinal segment caudal to the transection or contusion level.16 Yet, others did not find evidence of such a change.17 Although the mechanisms underlying the initial decrease (14–28 days) and subsequent recovery of MUNE values, which we observed remain to be established in future studies, the finding that MUNE values recovered to near pre-injury level by 56 days implies that trans-synaptic degeneration might not be significant or at least that it is reversible. Interestingly, this biphasic change in MUNE values after SCI is similar to that observed after stroke, which may involve both reversible trans-synaptic degeneration and local functional depression caused by neuronal shamming dead and/or functional inactivation.18
We still observed a U-shaped relationship between the changes in MUNE values from the MG muscle and the BBB scores in this study. In particular, there was a positive correlation between the recovery of MUNE value and BBB scores after MUNE values reached a bottom plateau 28 days after surgery. As the movements of affected hindlimb of transected rats recovered gradually, the MUNE value increased correspondingly. As the MUNE value returned to near pre-injury level (49–56 days), the motor function recovery (BBB scores) also reached an upper plateau. Accordingly, MUNE could represent a useful new method for assessing the progress of motor function recovery that occurs distal to the site of SCI in rats.
Additional morphological and electrophysiological studies are needed to examine the mechanisms that underlie the time-dependent changes in MUNE value after SCI. In addition, studies in animal models of incomplete SCI will help to confirm the relevance between changes in MUNE values and the functional recovery process distal to the site of SCI.
Conclusion
To the best of our knowledge, this is the first animal study that uses MUNE to examine changes in the number of functional lower motor neurons in the spinal segment caudle to the site of transection in rats. Our findings suggest a time-dependent change in MUNE values, which is associated with motor function recovery that occurs distal to the site of SCI. We suggest that MUNE value might be an objective outcome measure for evaluating motor function recovery that occurs distal to the site of SCI.
References
Adams M, Carlstedt T, Cavanagh J, Lemon RN, McKernan R, Priestley JV et al. International spinal research trust research strategy. III: A discussion document. Spinal Cord 2007; 45: 2–14.
Berrocal YA, Pearse DD, Andrade CM, Hechtman JF, Puentes R, Eaton MJ . Increased spinal c-Fos expression with noxious and non-noxious peripheral stimulation after severe spinal contusion. Neurosci Lett 2007; 413: 58–62.
Landrum LM, Jones SL, Blair RW . The expression of Fos-labeled spinal neurons in response to colorectal distension is enhanced after chronic spinal cord transection in the rat. Neuroscience 2002; 110: 569–578.
Bose P, Parmer R, Reier PJ, Thompson FJ . Morphological changes of the soleus motoneuron pool in chronic midthoracic contused rats. Exp Neurol 2005; 191: 13–23.
McComas AJ, Fawcett PR, Campbell MJ, Sica RE . Electrophysiological estimation of the number of motor units within a human muscle. J Neurol Neurosurgery Psychiatry 1971; 34: 121–131.
Kwon O, Lee KW . Reproducibility of statistical motor unit number estimates in amyotrophic lateral sclerosis: comparisons between size and number-weighted modifications. Muscle Nerve 2004; 29: 211–217.
Felice KJ . A longitudinal study comparing thenar motor unit number estimates to other quantiMGtive tests in patients with amyotrophic lateral sclerosis. Muscle Nerve 1997; 20: 179–185.
Shefner JM, Cudkowicz ME, Brown Jr RH . Comparison of incremental with multipoint MUNE methods in transgenic ALS mice. Muscle Nerve 2002; 25: 39–42.
Basso DM, Beattie MS, Bresnahan JC . A sensitive and reliable locomotor rating scale for open field testing in rats. J Neurotrauma 1995; 12: 1–21.
Wang FC, Delwaide PJ . Number and relative size of thenar motor units estimated by an adapted multiple point stimulation method. Muscle Nerve 1995; 18: 969–979.
Albrecht E, Kuntzer T . Number of Edb motor units estimated using an adapted multiple point stimulation method: normal values and longitudinal studies in ALS and peripheral neuropathies. Clin Neurophysiol 2004; 115: 557–563.
Fang J, Shahani BT, Graupe D . Motor unit number estimation by spatial-temporal summation of single motor unit potentials. Muscle Nerve 1997; 20: 461–468.
Boe SG, Stashuk DW, Doherty TJ . Motor unit number estimation by decomposition-enhanced spike-triggered averaging: control data, test-retest reliability, and contractile level effects. Muscle Nerve 2004; 29: 693–699.
Kudo N, Yamada T . Morphological and physiological studies of development of the monosynaptic reflex pathway in the rat lumbar spinal cord. J Physiol 1987; 389: 441–459.
Dietz V, Muller R, Colombo G . Locomotor activity in spinal man: significance of afferent input from joint and load receptors. Brain 2002; 125: 2626–2634.
Eidelberg E, Nguyen LH, Polich R, Walden JG . Transsynaptic degeneration of motoneurones caudal to spinal cord lesions. Brain Res Bull 1989; 22: 39–45.
Bjugn R, Nyengaard JR, Rosland JH . Spinal cord transection—no loss of disMGl ventral horn neurons. Modern stereological techniques reveal no transsynaptic changes in the ventral horns of the mouse lumbar spinal cord after thoracic cord transection. Exp Neurol 1997; 148: 179–186.
Hara Y, Masakado Y, Chino N . The physiological functional loss of single thenar motor units in the stroke patients: when does it occur? Does it progress? Clin Neurophysiol 2004; 115: 97–103.
Acknowledgements
We gratefully thank Li-Dong Pan for technical assistance and Claire Levine, MS, for editing the paper. This research was supported by grants from the China Rehabilitation Research Center of China (2006-15).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Xiong, GX., Guan, Y., Hong, Y. et al. Motor unit number estimation may be a useful method to evaluate motor function recovery after spinal cord transection in rats. Spinal Cord 48, 363–366 (2010). https://doi.org/10.1038/sc.2009.141
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2009.141
