
Abstract
Background:
To assess over the past year the sexuality of male patients with spinal-cord injury (SCI) over 50 years of age with spinal lesions of at least 20 years.
Methods:
Subjects were stratified in two groups: 44 individuals under 60 years and 55 individuals over 60 years. A detailed sexual anamnesis was taken for all, and the SF-36 Health Survey questionnaire was completed, with questions 13 and 14 concerning overall sexual life answered through the International Index of Erectile Function.
Results:
The younger group reached a median score of +50 for each domain of the SF-36; however, the differences between the two groups are not statistically relevant. The physical domain of the SF-36 showed a median score of 43.2 for the younger versus 41.1 for the older, whereas the mental domain showed 44.8 and 43.1, respectively. In the first group, 29/44 (65.9) individuals claimed erectile dysfunction versus 43/55 (78.1%) in the second, whereas 34/44 (77.2%) of the first group reported having sexual intercourse versus 13/55 (23.6%) with P<0.01 (χ2 test). In the 2nd, 29/55 (52.7%) individuals reported physical intimacy without sexual intercourse. For each group, the overall sexual satisfaction is statistically correlated to the duration of the relationship (linear progression test P<0.05).
Conclusions:
Median quality of life was high. Sexual intercourse is fundamental only for males of the first group. Most aging couples presented a different way of thinking about sex without the need for intercourse. Physicians should acquire knowledge about sexuality and aging in SCI patients.
Sponsorship:
This study was not sponsored.
Similar content being viewed by others

Introduction
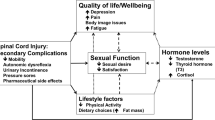
Spinal-cord injury (SCI) is an important cause of disability, which affects all aspects of a patient's life including sexuality. It may cause serious problems to quality of life, self-perception and life satisfaction of the patients. Sexuality is an important component of emotional and physical intimacy that men and women experience through their lives. As we age, we change. Such re-evaluation goes on for everyone, non-disabled and disabled alike. These adjustment concern sexual relationships and functioning. Menter has developed a model of aging that predicts functional decline of the individual with the duration of SCI. This model consists of the following three phases: acute restoration, maintenance and decline.1 Decline occurs as a result of degenerative effects of overuse syndromes and the physiologic aging process, in which an individual has to start modifying how they live using additional equipment and attendant care and reduce activity. A number of studies have validated the presence of this functional decline, which may begin as early as 10–15 years after injury or as late as 20 years after injury, depending on the unique set of circumstances.2, 3 The prevalence of sexual dysfunction increases as men and women age; about 40–45% of adult women and 20–30% of adult men have at least one manifest sexual dysfunction.4 In people with SCIs, the median percentage of sexual dysfunction is higher compared with the general population of the same age; in fact, a vast majority of men with both complete and incomplete SCI require treatment for erectile impairment.5 At this time, there is not much available data focused on the sexual life of SCI patients over 50 years of age with long-term lesions, although literature reports that about 60% of the elderly population expresses an interest in maintaining sexual activity.6 Overall life expectancies for subjects with SCI is continuing to increase, and in the last two decades, tremendous advances have been made in improving the quality of life for these individuals through new and better treatments in particular for erectile dysfunction.7, 8 Moreover, studies demonstrate that the presence of a supportive partner represents a determinant factor in whether someone with SCI will find sex satisfying.9 At the same time, Western societies have witnessed a tremendous cultural and social transformation in sexuality, a process Sigusch refers to as ‘the neosexual revolution’, meaning that people with chronic pathologies can achieve a good quality of life only if they have a satisfactory sexual life as well.10
The aim of this study is to elicit specific information about sexual life from men over 50 with SCI of 20 years or more to determine valid strategies, both preventive and restorative for having a long-lasting and satisfactory sexual life.
Methods
Through our database, we identified 110 male subjects aged over 50 who had an SCI of at least 20 years at the moment of the inclusion of the study. All patients were in a long-term follow-up in our Spinal Unit concerning spasticity/pain, skin care, bowel management and bladder and sexual function. Ninety-nine participants were included. Patients were divided into two groups according to age: the first group contained 44 individuals aged under 60 and the second group contained 55 subjects aged over 60. Median ages were 54.6 (range 52–58) and 66.4 (range 61–77), respectively. During the visit, all patients answered questions about their sexuality including questions 13 and 14 of International Index of Erectile Function (IIEF) composed of 15 questions concerning overall sexual satisfaction. In addition, they filled out the SF-36 Health Survey using the 0–100 scores providing information on health-related quality of life.11 Data were collected from personal interviews conducted by SCI physicians in our hospital, including demographics. Audio taping and field notes were utilized to gather data. Exclusion criteria: subjects who did not have a partner or did not answer all the questions on sexuality, and individuals who responded to less than half of the items on each SF-36 scale. Moreover, subjects with congenital spinal cord malformations were excluded. The investigators used consensus validation to complete data analysis, and all research findings were reviewed by the study participants for validation. In the statistical study of the data, we consider only those values with P<0.05 as significant.
Results
Overall, 110 potential subjects were detected in our database: three had died, two due to cardiovascular related problems and one due to bladder cancer.12 Four did not have a partner at the start of the study, two of them were widowers in the older group. Furthermore, four patients were not interested and refused participation. Ninety-nine individuals completed the study.
Details of injury
The two groups were quite homogenous with reference to the American Spinal Injury Association/International Medical Society of Paraplegia13 (see Table 1).
Demographics data
In Table 2, the degree of instruction and the occupational status of each group were reported.
The only item with a large difference in percentage between the two groups concerns disability pension. In the younger group, the subjects who received a pension were 34.1% versus 52.7% in the older group.
SF-36 Health Survey
In the younger group, the median score for all domains was over 50.
The median differences with the older group concern vitality, physical and social functioning, but it is not clinically relevant (see Figure 1). The same is true for the median SF-36 summary scores on physical and mental domains. In fact, on the physical score, patients aged under 60 had a median score of 43.29 compared with 41.01 for the subjects aged over 60, whereas on the mental domain, the younger group obtained a median score of 48.6 versus 43.06 for the older group.

The median score of the eight domains of the SF 36 Health Survey of the two groups is reported. No statistically significant difference between the two groups was found.
Evaluation of sexuality
Risk factors for sexuality
Twenty-four out of 55 SCI patients (43.6%) in the older group versus 15 out of 44 (34%) in the younger showed at least one risk factor. Twelve older subjects (50%) showed concomitant risks versus 7 in the younger group (46.6%). Of 15 subjects in the older group who suffered from chronic high blood pressure, 7 (46.6%) were using two different drugs for hypertension compared with 2 out of 7 (28.5%) in the younger group. Two patients in the older group were under pharmacological treatment—one for atrial fibrillation and the other for atherosclerosis—compared with 1 patient in the younger group under therapy for deep venous thrombosis. In the older group, three subjects were using sedatives and three others were using antidepressants for minor depression, whereas in the younger group, two were taking oral anti-anxiety and two antidepressants for minor depression. All smokers in both groups were chronic smokers (more than 3 years) and smoked at least 10 cigarettes a day. Table 3 reports the risk factors presented in both groups.
Relevant data on sexual function
The most relevant difference between the two groups was that 77.2% in first group compared with 23.6% in the older group have had sexual intercourse in the last year with P<0.01 using χ2 test. Main data on sexuality of both groups are shown in Table 4.
In Table 5, the reasons for a lack of sexual intercourse are reported.
Overall sexual satisfaction
All individuals in each group were divided into four groups according to the duration of their relationships: (A) 0–5 years, (B) 5–10 years, (C) 10–15 years, and (D) more than 15 years (see Table 6).
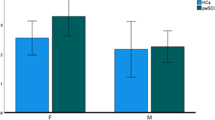
By means of IIEF questions 13 and 14, overall sexual satisfaction in each group was statistically correlated to the time of relationship (linear progression test) P<005 (see Figure 2). Particularly in the older group, 26 out of 29 patients who voluntarily preferred sexual intimacy without sexual intercourse were in the D class.

For each group, overall sexual satisfaction was statistically correlated with the duration of their relationship using linear regression test. In patients aged under 60, P<0.01, whereas in the older group, P<0.05.
Conclusion
Fifty years ago, people who had an SCI had very limited life expectancies. Today, these individuals can expect to live into their 70s and beyond, and in most cases with a good quality of life.14 Through the SF-36 Health Survey summary scores, we showed that the median differences between the two groups were not clinically relevant. The median quality of life in the older was good as well. With regard to vitality and physical and social functioning, the differences reported may be explained by the fact that most older patients had disability pensions and did not participate in part-time social work, resulting in more difficult interpersonal relationships. The presence of sexual dysfunctions is remarkable in both groups, and the higher percentage in the older group, although the increase was moderate, can be explained by more risk factors on erectile function, representing the natural course of the ageing process. Sexuality and affectivity constitute a complex phenomenon involving many spheres: biological, psychological and social, so it is not simply the act of sex.15, 16 Sexuality is important for adults with SCI , but their interests and sexual needs are variable. In fact, sexual intercourse is fundamental only for most of the subjects in the first group who more readily use specific chronic pharmacological treatments for improving their erectile function, whereas for individuals aged over 60, emotional affection is determinant for satisfactory sexuality, and most of these individuals declined appropriate pharmacological treatments to achieve valid sexual intercourse. For ageing couples to maintain mature sexual relations, it is more desirable to build the couples' relationship with physical contact through caresses and not focusing on sexual intercourse. A long relationship encourages the couple to explore and evolve other methods of intimacy. A long-lasting relationship with a partner represents a determinant factor in reaching a satisfactory sexual life as reported by other authors.17 In the older group, the partners' sexual dysfunctions and male functional bladder/bowel concerns represent possible obstacles to engaging in sexual intercourse.18 Concerning male SCI patients, another possible intervention is for the physician to inform patients of harmful life-style risks such as chronic smoking, which represents a negative factor on erectile function. Moreover, possible medical intervention can resolve erectile dysfunction that does not respond to pharmacological treatments; in our sample, 9% overall do not have sexual intercourse due to inefficacy of drugs. Hence, ageing with SCI is not something to be taken lightly, and neither is their sexuality. More research needs to be pursued in a manner that encompasses all aspects of sexual life; the fact that, in many societies, the continuance of sexuality during ageing is accepted, and in other societies sexuality is limited with ageing, suggests that cultural as well as biological factors may be key determinants in sexual behaviour in the later part of life.19, 20
To best deal with the multiple issues of the aging process, an individual with SCI needs to be cared for through an SCI system that is familiar with the ageing process and has the appropriate surveillance methodology, educational resources and interventions with regard to sexuality as well. Physicians should reserve particular attention for older individuals because for most of them erectile function intervention may not be required or needed as it does not represent the main focus of their sexuality.
References
Menter RR . Aging with spinal cord injury: CNI review. Spring 1998; 9.
Capoor J, Stein AB . Aging with spinal cord injury. Phys Med Rehabil Clin N Am 2005; 16: 129–161.
Charlifue S, Lammertse DP, Adkins RH . Aging with spinal cord injury: changes in selected health indices and life satisfaction. Arch Phys Med Rehabilitation 2004; 85: 1848–1853.
Lewis RW, Fugl-Meyer KS, Bosch R, Fugl-Meyer AR, Laumann EO, Lizza E, Martin-Morales A . Epidemiology/risk factors of sexual dysfunction. J Sex Med 2004; 1: 35–39.
Ramos AS, Samso JV . Specific aspects of erectile dysfunction in spinal cord injury. Int J Impot Res 2004; 16 (Suppl 2): 42–45.
Camacho ME, Reyes Ortiz CA . Sexual dysfunction in the elderly: age or disease? Int J Impot Res 2005; 17 (Suppl 1): S52–S56.
Derry F, Hultling C, Seftel AD, Sipski ML . Efficacy and safety of sildenafil citrate (Viagra) in men with erectile dysfunction and spinal cord injury: a review. Urology 2002; 60 (2 Suppl 2): 49–57.
Del Popolo G, Li Marzi V, Mondaini N, Lombardi G . Time/duration effectiveness of sildenafil versus tadalafil in the treatment of erectile dysfunction in male spinal cord-injured patients. Spinal Cord 2004; 42: 643–648.
Holicky R, Charlifue S . Ageing with spinal cord injury: the impact of spousal support. Disability Rehabil 1999; 21: 250–257.
Sigusch V . Social transformation of sexuality in the past decades. Overview Fortschr Neurol Pyschiatr 2000; 68: 97–106.
Forchheimer M, McAweeney M, Tate DG . Use of the SF-36 among persons with spinal cord injury. Am J Phys Med Rehabil 2004; 83: 390–395.
Strauss D, DeVivo MJ, Shavelle R . Long-term mortality risk after spinal cord injury. J Insurance Med 2000; 32: 11–16.
American Spinal Injury Association. International Standards for Neurological and Functional Classification of Spinal Cord Injury Revised 1996. American Spinal Injury Association: Chicago, 1996.
Putzke JD, Barrett JJ, Richards JS, De Vivo MJ . Age and spinal cord injury: an emphasis on outcomes among the elderly. J Spinal Cord Med 2003; 26: 37–44.
Reitz A, Tobe V, Knapp PA, Schurch B . Impact of spinal cord injury on sexual health and quality of life. Int J Impot Res 2004; 16: 167–174.
Umidi S, Pini M, Ferretti M, Vergani C, Annoni G . Affectivity and sexuality in the elderly: often neglected aspects. Arch Geront Geriatr 2007; 4 (Supp l): 413–417.
Phelps J, Albo M, Dunn K, Joseph A . Spinal cord injury and sexuality in married or partnered men: activities, function, needs, and predictors of sexual adjustment. Arch Sex Behav 2001; 30: 591–602.
Anderson KD, Borisoff JF, Johnson RD, Stiens SA, Elliott SL . The impact of spinal cord injury on sexual function: concerns of the general population. Spinal Cord 2007; 45: 328–337.
Lemaire A, Grivel T, Costa P, Lachowsky M, Elia D . Erectile dysfunction, sexuality and sociocultural aspects. Gynecol Obstet Fertil 2006; 34: 1154–1160.
Winn RL, Newton N . Sexuality in aging: a study of 106 cultures. Arch Sex Behav 1982; 11: 283–298.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lombardi, G., Macchiarella, A., Cecconi, F. et al. Sexual life of males over 50 years of age with spinal-cord lesions of at least 20 years. Spinal Cord 46, 679–683 (2008). https://doi.org/10.1038/sc.2008.37
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2008.37
Keywords
This article is cited by
-
Utilizing the Delphi Method to Assess Issues of Sexuality for Men Living with Spinal Cord Injury
Sexuality and Disability (2021)
