
Abstract
Study design:
An experimental, cross-sectional study.
Objective:
To investigate effects of external information or external cues on gait performance in independent ambulatory incomplete spinal cord injury (iSCI) patients (American Spinal Injury Association C or D, and functional independence measure walking scores=5–7).
Setting:
A university hospital, Thailand.
Method:
Gait performance was assessed in 29 patients with iSCI under four conditions including self-determined fastest walking speed, and fastest walking with the use of visual, auditory and visuotemporal cues. Average gait speed, stride length, cadence and percent step symmetry of these conditions were compared.
Results:
The use of external cues facilitated subjects to walk faster with a greater stride length, cadence and percent step symmetry than their own determination. The visuotemporal cue assisted subjects to increase their walking speed by 0.17 m s−1. The visual cue helped subjects to walk with a significantly greater stride length than the self-determined fastest pace condition (P<0.05). However, the visual cue made subjects walk with the lowest cadence and significantly lower than the visuotemporal cue condition (P<0.05).
Conclusion:
External information helped subjects to reorganize movement characteristics and perform a more efficient spatiotemporal gait pattern. The findings imply a significant role of external information on gait performance in patients with iSCI.
Similar content being viewed by others


Introduction
An important goal of patients with incomplete spinal cord injuries (iSCI) is the ability to walk again.1, 2 Although 80% of the patients can regain locomotory function, only a few of them can become functional walkers.3 They normally walk at a slow speed with long cycle duration and short stride length. An alteration of walking speed is considered a dominant change in these patients.4 Norris et al.5 indicate that walking speed is a crucial parameter to determine health status and ability to perform daily activities of an individual. An increment of walking speed commonly leads to the improvement of lower-extremity force production, walking distance and quality of walking such as step rhythm, foot placement, step symmetry and weight shift.6 An increase of 0.05–0.1 m s−1 in walking speed has clinical meaning. The change of 0.05 m s−1 in walking speed is regarded as having minimal clinical meaning, and 0.1 m s−1 is often considered to be a clinically useful improvement.5, 7 Step symmetry is also another vital parameter helping patients to have a safe and reciprocal gait pattern.8
An important challenge for patients with iSCI undergoing rehabilitation is the absence or reduced availability of normal afferent feedback systems. Therapists have to search for an alternative route helping the patients to generate an optimal movement pattern. External information applied to improved movement control during walking commonly include visual and auditory cues.9, 10 However, these cues facilitated patients to modify their movements according to the information provided. Visual cues are mostly applied to provide spatial adjustment (step length) whereas auditory cues are likely used for temporal adjustment (cadence). Thus, using these cues enable patients to increase their walking speed.11 However, patients with neurological disorders have various individual constraints. They may prefer to execute a particular task using different strategies. This study investigated effects of external cues in helping patients with iSCI to reorganize their spatiotemporal characteristics related to walking performance. We hypothesized that external cues would help patients to walk better than their own determination. In addition, we further hypothesized that an external cue without specific characteristics of movement adjustments would facilitate patients to generate better spatiotemporal characteristics than the cues with specific movement adjustment.
Materials and methods
Subjects
The study recruited patients with iSCI (American Spinal Injury Association (ASIA) C and D) who were able to walk independently with or without walking devices (functional independence measure (FIM) walking scores=5–7). Subjects were excluded if they had any other conditions that may affect walking such as pain or inflammation in the joints of the lower limbs. Subjects had to read and sign informed consent documents approved by the ethics committee of Khon Kaen University before taking part in the study.
Experimental protocol
Subjects participated in the study for 2 consecutive days. On the first day, subjects underwent screening tests to assess injury severity (ASIA impairment scale), the FIM walking scores and other conditions that may affect participation the study. On the second day, subjects’ walking abilities were tested under four conditions (with and without external cues) along an 8-m walkway with a sufficient period of rest between trials. First, subjects walked at their self-determined fastest walking speed (the uncued condition). The finding of this test was used to calculate appropriate cadence (for the auditory cue condition) and applied as a baseline ability of each subject. Then subjects continued the other trials with the use of three different external cues including visual, auditory and visuotemporal cues. Details of each tested condition are as follows:
• The visual cue condition
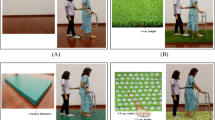
Subjects walked at their fastest speed and stepped each pace in accordance with colored tapes that were attached on the floor at an interval equal to 40% of the subject's height (Figure 1a).10, 11 Distance between the tapes provided an appropriate spatial adjustment (step length) for subjects to perceive by visual perception as the so-called ‘visual cue.’

Walking tests with the use of external cues. (a) The visual cue condition. (b) The auditory cue condition. (c) The visuotemporal cue condition.
• The auditory cue condition
Subjects walked at their fastest speed and stepped each foot according to the rhythm of the metronome that was set 25% faster than the baseline cadence of the subject (Figure 1b).11, 12 The beat of the metronome provided an appropriate temporal adjustment (cadence) for the subject to perceive by auditory perception as the so-called ‘auditory cue.’
• The visuotemporal cue condition
The test requires a ‘ball-moving machine’ (Figure 2), which is adapted from Majsak et al.,13 to provide temporal information for subjects to perceive by visual perception, as the so-called ‘visuotemporal cue.’ During the test, subjects had to walk as fast and safely as they could to grasp a tennis ball at the contact zone (Figure 1c). The contact zone is a 10-cm area in the middle of the moving track, which is indicated by a black tape marker (Figure 2). Subjects began to walk when they first saw the ball appear from behind the barrier. Each subject performed five trials. The first two trials were used to determine a suitable ball speed for the subject to successfully grasp the ball at the contact zone. After sufficient rest, subjects continued the other three trials with a short resting period between trials.

The ball-moving machine.
To reduce crossover effects, sequences of the external cue conditions were randomly ordered by using the Latin square. Subjects performed five trials of each condition with a physiotherapist walking alongside the subjects for safety reasons. The first two trials served as practice sessions for subjects to become familiar with the test conditions. For the visuotemporal cue, the first two trials were used to determine the fastest ball speed at which the subjects were able to successfully intercept the ball at the contact zone. After sufficient rest, subjects continued the other three trials, which were used for data recording of that condition with a period of rest between trials.
To avoid acceleration and deceleration effects, gait performances of each condition were recorded in the middle of the 3-m walkway. Walking characteristics of subjects were analyzed by using manual digitization, which was described by Said et al.15 The method has high validity (ICC3,1=0.95–0.99) compared to the PEAK motion analysis and high reliability (r=0.96, ICC3,1=0.94). It is a convenient method to use in a rehabilitation ward. To avoid bias of the researcher while working on manual digitization, the color tapes (visual cues) were left on the floor in every condition. However, this may result in subjects confusion with the cues. Thus, they were instructed to look forward while testing the other conditions.
Outcome measures
Outcomes of this study were spatiotemporal parameters related to walking performance including walking speed (m s−1), stride length (m), cadence (steps min−1) and percent step symmetry.
Statistical analyses
The study applied descriptive statistics to explain demographics of the subjects. One-way analysis of variance with repeated measures was used to compare the spatiotemporal variables among the conditions. All possible pairwise comparisons were analyzed by using the post hoc (Tukey) analysis. The level of significant differences was set at P<0.05.
Results
Subjects
Thirty-five patients with iSCI agreed to participate in the study. Six of them were excluded because of incomplete tests (four subjects because of increased spasticity, lower limb pain and technical errors), brain lesion involvement (one subject) and having cauda equina syndrome (one subject). Finally, there were 29 subjects that completed the study. Their average age and postinjury time was 44.03±15.23 years (range 16–67 years) and 37.69±53.90 months (range 1–264 months), respectively. Most subjects were at a chronic stage of spinal cord injury (range 7–264 months) and required walking devices for routine walking (Table 1). The neurological examination found decreased ASIA motor scores and sensation (Table 2) whereas some subjects showed increased muscle tone in supine position (Table 1). Other demographic characteristics of subjects are presented in Table 1.
Effects of the external cues on gait performance
The study evaluated effects of the visual, auditory and visuotemporal cues on four dependent spatiotemporal variables related to gait performance. These variables included walking speed, stride length, cadence and percent step symmetry. The findings on each variable are as follows.
Effects of external cues on walking speed
Subjects walked with the visuotemporal cue (median=0.57 m s−1) faster than they walked with the auditory and visual cues, and without external cue (median=0.43, 0.40 and 0.40 m s−1, respectively). Gait speed for the visuotemporal cue condition was 0.17 m s−1 greater than their self-determined fastest speed, which is a clinically useful improvement.5 However, there were no statistically significant differences among the conditions (Figure 3).

Walking speed when subjects walked with and without external cues. SF, self-determined fastest walking speed; V, visual cue condition; A, auditory cue condition; VT, visuotemporal cue condition.
Effects of external cues on stride length
Subjects walked with the visual and visuotemporal cues at a longer stride length (median=0.95 and 0.90 m, respectively) than when they walked with the auditory cue and without external cue (median=0.80 and 0.79 m, respectively). Stride lengths of the visual cue condition were significantly different from the uncued conditions (P<0.05; Figure 4).

Stride lengths when subjects walked with and without external cues. SF, self-determined fastest walking speed; V, visual cue condition; A, auditory cue condition; VT, visuotemporal cue condition.
Effects of external cues on walking cadence
Cadences of the visuotemporal and auditory cue conditions (median=77.91 and 67.35 steps min−1, respectively) were higher than those of the uncued condition (median=63.78 steps min−1). On the contrary, cadences of the visual cue condition (median=55.94 steps min−1) were lower than those of the uncued condition. A significant difference was found between the visuotemporal and the visual cue conditions (P<0.05; Figure 5).

Walking cadences when subjects walked with and without external cues. SF, self-determined fastest walking speed; V, visual cue condition; A, auditory cue condition; VT, visuotemporal cue condition.
Effects of external cues on percent step symmetry
Walking with the external cues resulted in a more symmetrical step length (median=86.57, 91.53 and 89.29% for the uncued, visual, auditory and visuotemporal cues, respectively) than walking without external cues (82.86%; Figure 6). However, there were no significant differences among the conditions (P>0.05).

Percent step symmetry when subjects walked with and without external cues. SF, self-determined fastest walking speed; V, visual cue condition; A, auditory cue condition; VT, visuotemporal cue condition.
Discussion
The study investigated effects of external information on gait performances of independent ambulatory iSCI subjects. The subjects demonstrated better spatiotemporal characteristics when they walked with the external cues than when they walked without external cues. The findings may imply that subjects had some capability that they were unable to access and generate of their own volition without additional cues. External information helped them to reorganize and execute a more efficient walking pattern. This may be because of the impairment of the somatosensory and motor systems as a result of SCI. Normally, the somatosensory system works as the internal reference of movement correction, with damage to this system limiting the ability of subjects to modify their movements according to the task demands.14 Appropriate external information acts as extrinsic feedback supplementary to the reduction of internal information. In addition, external information facilitates the intrinsic dynamics of the movement system through synchronizing or entraining the phase couplings among body segments.17 As a result, the use of external information assisted subjects to efficiently reorganize their movements and generate a higher level of capability than their own determination, despite having impairment of the motor and sensory systems.
The findings are consistent with the results of previous studies that have investigated effects of external information in patients with Parkinson's disease, stroke and normal subjects.10, 12, 15 Wagenaar and Beek17 report the successful application of the perception–action coupling by means of using external information (for example, visual, auditive or tactile) in patients with gait disorders. Researchers suggest that disorders of the physiological system are the consequences of not only the structural abnormality but also the abnormality of spatiotemporal organization.16, 18 An application of external information may provide subjects with appropriate temporal and spatial cues leading subjects to efficiently alter their movement. However, the wide variability seen in this study may be because of the diversity of subjects’ individual constraints (Table 1).
Among the external cues used in this study, the visuotemporal cue seemed to be the best form of information for gait speed and cadence. The visual cue is suitable for stride length whereas the auditory cue is useful for step symmetry. This may be because of different forms of information having their own characteristics thus helping subjects to generate different movement strategies. Gibson19 indicates that information is specific where the nature of information helps individuals to determine levels of force generation for the action. The visual cue provided spatial information, thus helping subjects to walk with the greatest stride length (Figure 4), but with the lowest walking speed and cadence (Figures 3 and 5). The auditory cue provided external rhythm to the subjects. Hence, they were able to walk at a higher cadence than their self-selected fast pace or when using the visual cue, however, without any increase in stride length. Walking at a short stride length may result in subjects demonstrating a more symmetrical step length. In contrast to the former two cues, the visuotemporal cue is a form of external information without specific characteristics for subjects to follow. Time from the starting to intercepting points provided temporal information that challenged subjects to perform optimal movements to successfully catch the ball at the contact zone. Such information may allow subjects to reorganize their movements according to their individual constraints. Thus, they were able to generate their highest capability and demonstrated marked improvement of both spatial and temporal characteristics. However, this information has an accelerative effect, thus it may not be suitable to use in patients with significant spasticity.
Results from this study indicated that external information facilitated subjects to walk faster than their own self-determined fastest pace.5 On the basis of the fact that most subjects in this study were chronic iSCI patients, the findings may infer dominant effects of external information on gait modification of patients with iSCI not only at the acute but also chronic stages of injury. Bach-y-Rita and Kercel20 report that the human movement system has great capability to use alternative sources of input. However, to confirm this effect, there is a need to further investigate potential advantages of gait training using external cues in a larger number of subjects with iSCI and other causes of gait disorders. In addition, results of this study came from subjects with various individual constraints, thus there is a need for further investigations on more homogenous groups of iSCI patients, such as patients with FIM walking scores=6 or 7, patients with paraparesis or quadriparesis, etc. Furthermore, a study on gait kinetics, gait kinematics and functional walking in homes and communities is also necessary to fulfill effects of external cues.
References
Fouad K, Pearson K . Restoring walking after spinal cord injury. Prog Neurobiol 2004; 73: 107–126.
Van der Salm A, Nene AV, Maxwell DJ, Veltink PH, Hermens HJ, Ijzerman MJ . Gait impairments in a group of patients with incomplete spinal cord injury and their relevance regarding therapeutic approaches using functional electrical stimulation. Artif Organs 2005; 29: 8–14.
Field-Fote E . Spinal cord control of movement: implications for locomotor rehabilitation following spinal cord injury. Phys Ther 2000; 80: 477–484.
Barbeau H, Ladouceur M, Norman KE, Pepin A, Leroux A . Walking after spinal cord injury: evaluation, treatment, and functional recovery. Arch Phys Med Rehabil 1999; 80: 225–235.
Norris JA, Granata KP, Mitros MR, Byrne EM, Marsh AP . Effect of augmented plantarflexion power on preferred walking speed and economy in young and older adults. Gait Posture 2007; 25: 620–627.
Field-Fote E, Tepavac D . Improved intralimb coordination in people with incomplete spinal cord injury following training with body weight support and electrical stimulation. Phys Ther 2002; 82: 707–715.
Perera S, Mody SH, Woodman RC, Studenski SA . Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc 2006; 54: 743–749.
Field-Fote E, Fluet G, Schafer S, Schneider E, Smith R, Downey P et al. The spinal cord injury functional ambulation inventory (SCI-FAI). J Rehabil Med 2001; 33: 177–181.
Azulay JP, Mesure S, Blin O . Influence of visual cues on gait in Parkinson's disease: contribution to attention or sensory dependence? J Neurol Sci 2006; 248: 192–195.
Jiang Y, Normam KE . Effects of visual and auditory cues on gait initiation in people with Parkinson's disease. Clin Rehab 2006; 20: 36–45.
Suteerawattananon M, Morris GS, Etnyre BR, Jankovic J, Protas EJ . Effects of visual and auditory cues on gait in individuals with Parkinson's disease. J Neurol Sci 2004; 219: 63–69.
Van Hedel HJ, Dietz V, Curt A . Assessment of walking speed and distance in subjects with an incomplete spinal cord injury. Neurorehabil Neural Repair 2007; 21: 295–301.
Majsak MJ, Kaminski T, Gentile AM, Flanagan R . The reaching movements of patients with Parkinson's disease under self-determined maximal speed and visually cued conditions. Brain 1998; 121: 755–766.
Beek P, van Wieringen P . Perspectives on the relation between information and dynamics: an epilogue. Hum Mov Sci 1994; 13: 519–533.
Reynolds RF, Day BL . Visual guidance of the human foot during a step. J Physiol 2005; 569: 677–684.
Said C, Goldie P, Patla A, Sparrow W, Martin K . Obstacle crossing in subjects with stroke. Arch Phys Med Rehabil 1999; 80: 1054–1059.
Wagenaar RC, Beek WJ . Hemiplegic gait: a kinematic analysis using walking speed as a basis. J Biomech 1992; 25: 1007–1015.
Wagenaar R, van Emmerik R . Dynamics of pathological gait. Hum Mov Sci 1994; 13: 441–471.
Gibson JJ . The Ecological Approach to Visual Perception. Houghton Mifflin: Boston, 1979.
Bach-y-Rita P, Kercel S . Sensory substitution and the human–machine interface. Trends Cogn Sci 2003; 7: 541–546.
Acknowledgements
This study was supported by grants from the Graduate School and Faculty of Associated Medical Sciences, Khon Kaen University, Thailand.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Amatachaya, S., Keawsutthi, M., Amatachaya, P. et al. Effects of external cues on gait performance in independent ambulatory incomplete spinal cord injury patients. Spinal Cord 47, 668–673 (2009). https://doi.org/10.1038/sc.2008.168
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2008.168
Keywords
This article is cited by
-
Immediate effects of lower limb loading exercise during stepping with and without augmented loading feedback on mobility of ambulatory individuals with spinal cord injury: a single-blinded, randomized, cross-over trial
Spinal Cord (2020)
-
Do ambulatory patients with spinal cord injury walk symmetrically?
Spinal Cord (2017)
-
Effects of a visuotemporal cue on walking ability of independent ambulatory subjects with spinal cord injury as compared with healthy subjects
Spinal Cord (2014)
-
Locomotor adaptation to resistance during treadmill training transfers to overground walking in human SCI
Experimental Brain Research (2012)
-
Comparing the efficacy of metronome beeps and stepping stones to adjust gait: steps to follow!
Experimental Brain Research (2011)
