
Abstract
Serum sodium concentration within the normal range could act as an indicator of age-related changes such as decrease in muscle strength and impairment of capillary function. Since endothelial injury stimulates endothelial repair by enhancing CD34-positive cell production, the level of serum sodium may be inversely associated with that of circulating CD34-positive cells, thus indicating the degree of age-related endothelial injury. We conducted a cross-sectional study of 246 elderly Japanese men aged 60–69 years. Subjects were stratified by hypertension status because hypertension should act as a strong confounding factor for the analyses performed in this study. Serum sodium concentration was positively associated with handgrip strength in non-hypertensive subjects [standardized parameter estimate (β) = 0.29; p = 0.003], but not for hypertensive subjects (β = 0.01; p = 0.878), while it was inversely associated with circulating CD34-positive cell levels in non-hypertensive subjects [simple correlation coefficient (r) = − 0.28; p = 0.002] but not for hypertensive subjects (r = − 0.07; p = 0.454). For non-hypertensive elderly subjects, serum sodium concentration within the normal range is positively associated with handgrip strength and inversely associated with CD34-positive cells, thus partly indicating the degree of age-related endothelium injury. These associations could prove to be an efficient tool for clarifying the background mechanism governing the decrease in age-related muscle strength.
Similar content being viewed by others

Introduction
Elderly men with low serum sodium levels within the normal range (136–138 mEq/L) showed higher risks of major cardiovascular events and total mortality than those with low serum sodium levels within the upper normal range (139–143 mEq/L)1. This study also showed a positive association between serum sodium level and muscle mass evaluated on the basis of mid-arm muscle circumference. Since hyponatremia is a multifactorial condition related to aging2,3,4,5,6,7, a serum sodium level within the normal range could act as an indicator of age-related change.
Capillary function, known as a function of microcirculation is associated with cardiovascular risk factors8,9.
In addition, sarcopenia is associated with impairment of capillary function10 and handgrip strength, a predictor of age-related disability, is an efficient tool for evaluating the decrease in muscle strength and function in the elderly11.
Serum sodium levels within normal range could therefore also be positively associated with handgrip strength by indicating age-related disruption of microcirculation.
Further, CD34-positive cell concentration is a known factor contributing to endothelial repair12, while endothelial injury in turn should stimulate CD34-positive cell production13,14,15,16. Serum sodium levels can therefore be inversely associated with CD34-positive cell concentration because higher serum sodium levels might indicate a reduction in endothelial injury, resulting in diminished production of CD34-positive cells.
However, hypertension is well known to be a strong endothelium impairment factor17 that induces the reduction of circulating CD34-positive cells due to consumption18,19,20. Consequently, hypertension could act as a strong confounding factor on those associations. To clarify those associations, we conducted a cross-sectional study of 246 Japanese elderly men aged 60–69 who participated in an annual health check-up in 2014–2015.
Methods
Study population
The total number of male residents of Goto city aged 60–69 (estimated by the National Institute of Population and Social Security Research in March 2013) was 3264 in 201521. The study population comprised 274 male residents aged 60–69 years from the Goto city located in the western part of Japan, who underwent an annual medical check-up between 2014 and 2015 as recommended by the Japanese government. Subjects with high (> 145 mEq/L, n = 10) and low (< 135 mEq/L, n = 1) sodium levels were excluded from the study population. To avoid the influence of chronic inflammatory disease and paralysis caused by stroke, subjects with a high white blood cell count (WBC) (≥ 10,000 cells/μL) (n = 1) and history of stroke (n = 13) were also excluded from the analysis. Subjects without handgrip strength data (n = 3) were also excluded. The remaining patients, 246 men with a mean age of 65.4 years (standard deviation): 2.6; range 60–69) were enrolled in the study.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Ethics Committee for Human Use of Nagasaki University (project registration number 14051404). Written consent forms were available in Japanese to ensure comprehensive understanding of the study objectives, and informed consent was provided by the participants.
Data collection and laboratory measurements
Body weight and height were measured with an automatic body composition analyzer (BF-220; Tanita, Tokyo, Japan), followed by calculation of body-mass index (BMI; kg/m2). Systolic (SBP) and diastolic blood pressure (DBP) were recorded at rest. Hypertension was defined as a SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg, as in our previous studies that used circulating CD34-positive cells18,19,20.
Blood samples were collected in an EDTA-2K tube, a heparin sodium tube, a siliconized tube and a sodium fluoride tube. Platelet levels and white blood cells (WBC) in samples from the EDTA-2K tube were measured at SRL, Inc. (Tokyo, Japan) with an automated procedure.
Fresh samples from the heparin sodium tube were used within 24 h of collection to determine the number of circulating CD34-positive cells by means of BD Trucount technology (Beckton Dickinson Biosciences; San Jose, CA), an accurate and reproducible single platform assay conforming to the International Society of Hematotherapy and Graft Engineering (ISHAGE) guidelines22 and supported by automated software on the BD FACSCanto II system.
Triglycerides (TG), HDL-cholesterol (HDLc), serum creatinine, γ-glutamyltranspeptidase (γ-GTP), hemoglobin A1c (HbA1c) as well as electrolyte—potassium (K), phosphorus (P), calcium (Ca) and sodium (Na)—concentrations were measured with standard laboratory procedures at SRL, Inc. (Tokyo, Japan). Glomerular filtration rate (GFR) was estimated by means of an established method modified as recently proposed by the working group of the Japanese Chronic Kidney Disease Initiative23. With this adapted version, GFR (mL/min/1.73 m2) was defines as 194 × (serum creatinine (enzyme method))−1.094 × (age)−0.287.
Handgrip strength was determined with a handgrip dynamometer (Smedley, Matsumiya Ika Seiki Seisakujo, Tokyo, Japan) as the grip strength from two measurements obtained for each hand, from which the maximum value was used.
Statistical analysis
Characteristics of the study population stratified by hypertension status were expressed as mean ± standard deviation except for TG, γ-GTP and circulating CD34-positive cells. Since these factors showed a skewed distribution, the characteristics of the study population were expressed as medians [first quartile, third quartile], followed by logarithmic transformation. A χ2 test was performed to calculate the p value of each variable on the basis of hypertension status. Simple correlation analysis and multiple linear regression analysis of handgrip strength with sodium concentration or CD34-positive cell levels were performed after adjustments for confounding factors and stratification by hypertension status. For this study it was assumed serum sodium indicates age-related endothelial injury, which stimulates CD34-positive cell production. Therefore, to avoid the influence of over-adjustment on the multiple regression analysis, we performed a separate analysis to evaluate the association of serum sodium concentration and circulating CD34-positive cell levels with handgrip strength. For the multiple linear regression analysis, adjustments were then made for age, SBP (mmHg), antihypertensive medication use (yes/no), BMI (kg/m2), HDLc (mg/dL), TG (mg/dL), HbA1c (%) γ-GTP (U/L), WBC (cells/μL), GFR (mL/min/1.73m2), K (mEq/L), Ca (mg/dL) and P (mg/dL).
CD34-positive cells constitute a factor that is known to contribute to endothelial repair12 in conjunction with platelets13,14,24,25, while the number of platelets indicates the activity of vascular repair18,19. Furthermore, aggressive endothelial injury could cause reduction in CD34-positive cells due to consumption, but this type of reduction may not affect platelets18,19,26. Therefore, we calculated simple correlation coefficients for these factors.
All statistical analyses were performed with the SAS system for Windows (version 9.4: SAS Inc., Cary, NC, USA). Values of p < 0.05 were considered statistically significant.
Results
Among present study population, 125 are diagnosed as having hypertension.
Characteristics of study population by hypertension status.
Characteristics of the study population by hypertension status as displayed in Table 1 show that 125 subjects were diagnosed with hypertension. Compared with non-hypertensive subjects, hypertensive subjects showed significantly higher values for systolic blood pressure, diastolic blood pressure, antihypertensive medication use, BMI, and significantly lower values for serum K.
Correlations between handgrip strength and relevant factors for subjects without hypertension
Results of simple correlation analysis show that handgrip strength is significantly positively associated with serum sodium concentration but not with circulating CD34-positive cell levels for subjects without hypertension. Even with further adjustments for other possible variables, these correlations remain unchanged (Table 2).
Correlations between handgrip strength and relevant factors for subjects with hypertension
Simple correlation analysis findings show that handgrip strength is significantly positively associated with circulating CD34-positive cell levels but not with serum sodium concentration for subjects with hypertension. Even with further adjustments for other possible variables, these correlations remain unchanged (Table 3).
Simple correlation analysis of circulating CD34-positive cell levels and platelet concentration, and of circulating CD34-positive cell levels and serum sodium concentration by hypertension status
Simple correlation analysis findings demonstrate that for subjects without hypertension, circulating CD34-positive cell levels are significantly positively correlated with platelet concentration but inversely correlated with serum sodium concentration. For subjects with hypertension, no significant correlations were obtained (Table 4).
Discussion
The major findings of the present study are that for non-hypertensive subjects, independent of known cardiovascular risk factors, serum sodium concentration is significantly positively associated with handgrip strength while significantly inversely associated with circulating CD34-positive cell levels whereas no such significant correlations exist for hypertensive subjects.
A previous Japanese meta-analysis study reported a scatter plot of age compared with handgrip strength based on a meta-regression analysis where handgrip strength (kg) = 78.74 − 0.62 × age (years) for men27. As the age range for the present target population was 60–69 years, the reference values of handgrip strength calculated using the above formula ranged from 36.0 to 41.5 kg. The mean (standard deviation) handgrip strength values in all the subjects in the present study were 38.8 (6.0) kg. Therefore, we believe that the representative subjects were secured in the present study population.
A previous study with 3099 elderly men aged 60–79 years without a history of cardiovascular disease (CVD) showed a positive association between serum sodium level and muscle mass1. In our study, we found further evidence that independent of known cardiovascular risk factors, the normal range of serum sodium levels is positively associated with handgrip strength limited to elderly men without hypertension.
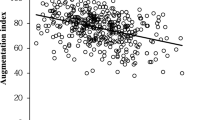
Figure 1 shows the major findings of the present study that serum sodium level was significantly positively associated with handgrip strength in non-hypertensive subjects but not in hypertensive subjects. In the non-hypertensive subjects, serum sodium level was significantly inversely associated with CD34-positive cells but not in the hypertensive subjects. Figure 2 shows the potential mechanism underlying the present results.

Associations observed in the present study.

Possible mechanism underlying the association between serum sodium level and handgrip strength.
Hyponatremia is the most common electrolyte disorder in the geriatric age group28. Even though the most important cause of hyponatremia in the elderly is syndrome of inappropriate secretion of anti-diuretic hormone (SIADH)2, hyponatremia is frequently multifactorial2,3,4,5,6,7 and entails several causative factors such as medication (thiazide and loop diuretics, proton pump inhibitors, non-steroidal anti-inflammatory agents), cardiac failure, chronic kidney disease, chronic liver disease, respiratory infections, volume overloaded and dehydration3,7 (Fig. 2-3). Since those factors are common in elderly subjects, serum sodium levels within the normal range could function as an indicator of general age-related physiological change instead of indicating a specific disease (Fig. 2-α).
Further, handgrip strength is an efficient tool to evaluate the decrease in muscle strength and function due to its use as a predictor of old disability11. Therefore, serum sodium concentration within normal range could be associated with handgrip strength by indicating age-related physical change.
In our study, however, a positive correlation between serum sodium concentration and handgrip strength was observed only for subjects without hypertension (Tables 2, 3, Fig. 2c,g).
Blood flow to the skeletal muscle is a potentially important factor in maintaining muscle function in the elderly29, possibly by maintaining protein metabolism30,31. Previously, handgrip strength was found to be inversely associated with microcirculation disruption evaluated using the cardiovascular index (CAVI) in subjects with non-hypertension but not in subjects with hypertension8,32 (Fig. 2-7).
Hypertension and decreased muscle strength and function are known to be age-related diseases and are reportedly exacerbated by the disruption of the microvascular endothelium and impairment of blood flow resulting from an increase in age-related agents such as inflammatory agents33 and oxidative stress29 (Fig. 2-1). The condition of the microvascular endothelium might therefore play an important role in the correlations between serum sodium concentration and handgrip strength.
Platelets are the first circulating blood cells that interact with an injured endothelium34 (Fig. 2-4). In addition, we reported elsewhere that the number of platelets indicates the activity of vascular repair18, while platelet-rich plasma could enhance the proliferation of bone marrow mesenchymal stem cells, which are known to be multi-potent stem cells25. Furthermore, CD34-positive cells are known to contribute to endothelial repair12 in conjunction with platelets13,24 (Fig. 2-5), while the number of circulating CD34-positive cells could indicate the capability of endothelial maintenance19,20,35. This means that platelets could be positively associated with circulating CD34-positive cell levels, as observed in our subjects without hypertension (Table 4; Fig. 2a). However, since the production of circulating CD34-positive cells must be stimulated by endothelial injury, the level of circulating CD34-positive cells could indicate the degree of age-related endothelial injury (Fig. 2-5). In our current study, we identified a significant inverse correlation between serum sodium concentration and circulating CD34-positive cell levels in subjects without hypertension (Table 4; Fig. 2b,f). For subjects without hypertension, serum levels of sodium could therefore be inversely associated with age-related endothelial injury (Fig. 2-β).
Furthermore, hypertension is a well-known strong endothelial impairment factor17 that causes aggressive endothelium repair, which in turn may cause a reduction in circulating CD34-positive cells due to consumption18,26 (Fig. 2-8), although this type of reduction may not affect platelets18,19,36. This explains why, even if CD34-positive cell levels are significantly positively associated with platelets in non-hypertensive subjects, no significant correlation was observed for hypertensive subjects (Table 4; Fig. 2a,e).
Reduction of circulating CD34-positive cells due to consumption might therefore determine the number of circulating CD34-positive cells in subjects with hypertension but not in those without hypertension. Lower levels of circulating CD34-positive cells in hypertensive subjects might indicate the existence of aggressive endothelial repair induced by severe endothelial injury, both of which are harmful factors for maintaining muscle strength. As a result, we detected a positive association between handgrip strength and circulating CD34-positive cells in hypertensive but not in non-hypertensive men (Tables 2, 3; Fig. 2d,h), as we did in a previous study37. In this case, CD34-positive cell levels indicate the appropriateness of endothelial repair (Fig. 2-γ).
Aggressive endothelial repair, which induces reduction of circulating CD34-positive cells due to consumption, could be associated with hypertension19 (Fig. 2-8). However, previous studies revealed a positive association between handgrip strength and blood pressure in older participants38,39 (Fig. 2-9). In our study, even if the power did not reach significance, the subjects with hypertension showed slightly stronger handgrip strength than those without hypertension (Table 1). Hypertension is a well-known cardiovascular risk factor40 (Fig. 2-6), and low handgrip strength has been reported to be positively associated with CVD41 (Fig. 2-2). As CD34-positive cells are positively associated with handgrip strength in hypertension (Table 3; Fig. 2h), active appropriate endothelial repair stimulated by endothelial injury might play an important role in maintaining muscle strength in hypertensive subjects, while low-grade endothelial injury might be critical for maintaining muscle strength in the absence of hypertension. Therefore, even serum sodium levels within the normal range could act as an indicator of general age-related physiological changes in non-hypertensive subjects (Fig. 2-α), including handgrip strength (Table 2; Fig. 2c). Under the influence of hypertension, serum sodium level was no longer associated with handgrip strength because hypertension itself could act as a confounding factor in this association (Table 3; Fig. 2g). A previous study revealed that active endothelial repair should have a beneficial influence on maintaining muscle strength in elderly patients with hypertension42,43 that could support this mechanism. Further investigation to clarify the mechanism by which hypertension possesses a beneficial influence on maintaining muscle strength is necessary.
Unlike a general epidemiological study, which reveals the risk factors for the same unfavorable conditions as those of our subjects, our current study was used a multi-faceted analysis of a simple target population. Therefore, our study not only identified the simple risk factors but also clarified the possible background mechanism of age-related physical change.
Although our present study employs a small sample size, it is the largest study in the world that deals with circulating CD34-positive cells among the general population who are selected in a strict manner as like previous of our study18,19,20,26,36,37.
The clinical implication of our findings is that serum sodium concentration, which is a factor measurable in daily clinical practice, could act as an indicator of age-related endothelial injury and a predictor of age-related disability in non-hypertensive subjects.
A few potential limitations of this study warrant consideration. Because the study population comprised subjects who underwent an annual health-checkup, selection bias may exist since the subjects were likely have a higher than average self-interest in their health. Although serum sodium concentration is inversely associated with circulating CD34-positive cell levels among subjects without hypertension, no data were available for the evaluation of endothelial function. As aging is the main contributing factor to decline in endothelial function44, further analyses that include endothelial function-related data such as flow-mediated dilation (FMD) will be necessary. Unknown confounding factors such as medication status and duration of medication for hypertension, diabetes, dyslipidemia, inflammatory disease, and thyroid disease, could influence the present study. Further investigation with consideration of this information is necessary.
In conclusions, independent of known cardiovascular risk factors, serum sodium concentration is significantly positively associated with handgrip strength and significantly inversely associated with circulating CD34-positive cell levels for non-hypertensive subjects whereas no such significant correlations were observed for hypertensive subjects.
References
Wannamethee, S. G. et al. Mild hyponatremia, hypernatremia and incident cardiovascular disease and mortality in older men: A population-based cohort study. Nutr. Metab. Cardiovasc. Dis. 26, 12–19. https://doi.org/10.1016/j.numecd.2015.07.008 (2016).
Soiza, R. L. et al. Syndrome of appropriate antidiuretic hormone: Difficulties with diagnosing syndrome of inappropriate antidiuretic hormone in older people. Int. Med. J. 41, 295 (author reply 296). https://doi.org/10.1111/j.1445-5994.2010.02388.x (2011).
Gankam, K. F. et al. Mild hyponatremia and risk of fracture in the ambulatory elderly. QJM. 101, 583–588. https://doi.org/10.1093/qjmed/hcn061 (2008).
Clayton, J. A. et al. Severe hyponatraemia in medical in-patients: Aetiology, assessment and outcome. QJM. 99, 505–511. https://doi.org/10.1093/qjmed/hcl071 (2006).
Shapiro, D. S. et al. Severe hyponatraemia in elderly hospitalized patients: Prevalence, aetiology and outcome. Int. Med. J. 40, 574–580. https://doi.org/10.1111/j.1445-5994.2010.02217.x (2010).
Cumming, K. et al. Prevalence, incidence and etiology of hyponatremia in elderly patients with fragility fractures. PLoS One. 9, e88272. https://doi.org/10.1371/journal.pone.0088272 (2014).
Ayus, J. C. et al. Is chronic hyponatremia a novel risk factor for hip fracture in the elderly?. Nephrol. Dial. Transplant. 27, 3725–3731. https://doi.org/10.1093/ndt/gfs412 (2012).
Shiba, T. et al. Arterial stiffness shown by the cardio-ankle vascular index is an important contributor to optic nerve head microcirculation. Graefes Arch. Clin. Exp. Ophthalmol. 255, 99–105. https://doi.org/10.1007/s00417-016-3521-9 (2017).
Laucevičius, A. et al. Association of cardio-ankle vascular index with cardiovascular risk factors and cardiovascular events in metabolic syndrome patients. Medicina (Kaunas). 51, 152–158. https://doi.org/10.1016/j.medici.2015.05.001 (2015).
Wang, H. et al. Apoptosis in capillary endothelial cells in ageing skeletal muscle. Aging Cell. 13, 254–262. https://doi.org/10.1111/acel.12169 (2014).
Fried, L. P. et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 56, 146–156. https://doi.org/10.1093/gerona/56.3.m146 (2001).
Shi, Q. et al. Evidence for circulating bone marrow-derived endothelial cells. Blood. 92, 362–367 (1998).
Stellos, K. et al. Platelet-derived stromal cell-derived factor-1 regulates adhesion and promotes differentiation of human CD34+ cells to endothelial progenitor cells. Circulation 117, 206–215. https://doi.org/10.1161/CIRCULATIONAHA.107.714691 (2008).
Stellos, K. et al. Expression of stromal-cell-derived factor-1 on circulating platelets is increased in patients with acute coronary syndrome and correlates with the number of CD34+ progenitor cells. Eur. Heart J. 30, 584–593. https://doi.org/10.1093/eurheartj/ehn566 (2009).
Seitz, G. et al. The role of sphingosine 1-phosphate receptors in the trafficking of hematopoietic progenitor cells. Ann. N Y Acad. Sci. 1044, 84–89. https://doi.org/10.1196/annals.1349.011 (2005).
Golan, K. et al. S1P promotes murine progenitor cell egress and mobilization via S1P1-mediated ROS signaling and SDF-1 release. Blood 119, 2478–2488. https://doi.org/10.1182/blood-2011-06-358614 (2012).
Nakamura, S. et al. A novel vascular modulator, hepatocyte growth factor (HGF), as a potential index of the severity of hypertension. Biochem. Biophys. Res. Commun. 242, 238–243. https://doi.org/10.1006/bbrc.1997.7800 (1998).
Shimizu, Y. et al. Platelets as an indicator of vascular repair in elderly Japanese men. Oncotarget 7, 44919–44926. https://doi.org/10.18632/oncotarget.10229 (2016).
Shimizu, Y. et al. Platelets and circulating CD34-positive cells as an indicator of the activity of the vicious cycle between hypertension and endothelial dysfunction in elderly Japanese men. Atherosclerosis 259, 26–31. https://doi.org/10.1016/j.atherosclerosis.2017.02.016 (2017).
Shimizu, Y. et al. Circulating CD34-positive cells, glomerular filtration rate and triglycerides in relation to hypertension. Atherosclerosis 243, 71–76. https://doi.org/10.1016/j.atherosclerosis.2015.08.035 (2015).
National Institute of Population and Social Security Research [Home page on the Internet]. http://www.ipss.go.jp/pp-shicyoson/j/shicyoson13/3kekka/Municipalities.asp.
Sutherland, D. R. et al. The ISHAGE guidelines for CD34+ cell determination by flow cytometry. International Society of Hematotherapy and Graft Engineering. J. Hematother. 5, 213–226. https://doi.org/10.1089/scd.1.1996.5.213 (1996).
Imai, E. et al. Prevalence of chronic kidney disease in the Japanese general population. Clin. Exp. Nephrol. 13, 621–630. https://doi.org/10.1007/s10157-009-0199-x (2009).
Daub, K. et al. Platelets induce differentiation of human CD34+ progenitor cells into foam cells and endothelial cells. FASEB J. 20, 2559–2561. https://doi.org/10.1096/fj.06-6265fje (2006).
Zou, J. et al. The effects of platelet-rich plasma on the osteogenic induction of bone marrow mesenchymal stem cells. Connect Tissue Res. 55, 304–309. https://doi.org/10.3109/03008207.2014.930140 (2014).
Shimizu, Y. et al. Hepatocyte growth factor and carotid intima-media thickness in relation to circulating CD34-positive cell levels. Environ Health Prev. Med. 23, 16. https://doi.org/10.1186/s12199-018-0705-4 (2018).
Kamide, N. et al. Reference values for hand grip strength in Japanese community-dwelling elderly: A meta-analysis. Environ Health Prev. Med. 20, 441–446. https://doi.org/10.1007/s12199-015-0485-z (2015).
Soiza, R. L. et al. Management of hyponatraemia in older people: Old threats and new opportunities. Ther. Adv. Drug Saf. 2, 9–17. https://doi.org/10.1177/2042098610394233 (2011).
McCully, K. K. et al. The application of blood flow measurements to the study of aging muscle. J. Gerontol. A Biol. Sci. Med. Sci. 50, 130–136. https://doi.org/10.1093/gerona/50a.special_issue.130 (1995).
Fry, C. S. et al. Skeletal muscle protein balance and metabolism in the elderly. Curr. Aging Sci. 4, 260–268. https://doi.org/10.2174/1874609811104030260 (2011).
Zhang, X. J. et al. Acute responses of muscle protein metabolism to reduced blood flow reflect metabolic priorities for homeostasis. Am. J. Physiol. Endocrinol. Metab. 294, E551-557. https://doi.org/10.1152/ajpendo.00467.2007 (2008).
Yamanashi, H. et al. Association between atherosclerosis and handgrip strength in non-hypertensive populations in India and Japan. Geriatr. Gerontol. Int. 18, 1071–1078. https://doi.org/10.1111/ggi.13312 (2018).
Payne, G. W. Effect of inflammation on the aging microcirculation: Impact on skeletal muscle blood flow control. Microcirculation 13, 343–352. https://doi.org/10.1080/10739680600618918 (2006).
Chen, J. et al. Interactions of platelets with subendothelium and endothelium. Microcirculation. 12, 235–246. https://doi.org/10.1080/10739680590925484 (2005).
Bielak, L. F. et al. Circulating CD34+ cell count is associated with extent of subclinical atherosclerosis in asymptomatic Amish men, independent of 10-year Framingham risk. Clin. Med. Cardiol. 3, 53–60. https://doi.org/10.4137/cmc.s2111 (2009).
Shimizu, Y. et al. Possible mechanism underlying the association between height and vascular remodeling in elderly Japanese men. Oncotarget 9, 7749–7757. https://doi.org/10.18632/oncotarget.23660 (2017).
Yamanashi, H. et al. Circulating CD34-positive cells are associated with handgrip strength in Japanese older men: The Nagasaki Islands Study. J. Frailty Aging. 6, 6–11. https://doi.org/10.14283/jfa.2016.107 (2017).
Ji, C. et al. Handgrip strength is positively related to blood pressure and hypertension risk: Results from the National Health and Nutrition Examination Survey. Lipids Health Dis. 17, 86. https://doi.org/10.1186/s12944-018-0734-4 (2018).
Taekema, D. G. et al. Higher blood pressure is associated with higher handgrip strength in the oldest old. Am. J. Hypertens. 24, 83–89. https://doi.org/10.1038/ajh.2010.185 (2011).
Viera, A. J. Screening for hypertension and lowering blood pressure for prevention of cardiovascular disease events. Med. Clin. North Am. 101, 701–712. https://doi.org/10.1016/j.mcna.2017.03.003 (2017).
Peterson, M. D. et al. Low normalized grip strength is a biomarker for cardiometabolic disease and physical disabilities among US and Chinese adults. J. Gerontol. A Biol. Sci. Med. Sci. 72, 1525–1531. https://doi.org/10.1093/gerona/glx031 (2017).
Shimizu, Y. et al. Association between tongue pressure and subclinical carotid atherosclerosis in relation to platelet levels in hypertensive elderly men: A cross-sectional study. Environ Health Prev. Med. 23, 31. https://doi.org/10.1186/s12199-018-0720-5 (2018).
Shimizu, Y. et al. Handgrip strength and subclinical carotid atherosclerosis in relation to platelet levels among hypertensive elderly Japanese. Oncotarget 8, 69362–69369. https://doi.org/10.18632/oncotarget.20618 (2017).
Majerczak, J. et al. Age-dependent impairment in endothelial function and arterial stiffness in former high class male athletes is no different to that in men with no history of physical training. J. Am. Heart Assoc. 8, e012670. https://doi.org/10.1161/JAHA.119.012670 (2019).
Acknowledgements
We are grateful to the staff of Goto city hall for their outstanding support. This work was supported financially by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (Nos. 18K06448 and 17H03740).
Author information
Authors and Affiliations
Contributions
Y.S. designed the study and performed the statistical analyses, interpreted the data, and drafted the manuscript or revised it. H.Y., S.F., S.Y.K. and Y.N. assisted with the design of the study, were involved in data collection, and checked the manuscript. H.Y., S.Y.K. and T.M. participated in the study concept and checked the manuscript. T.M. was the general coordinator and also designed the study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shimizu, Y., Yamanashi, H., Fukui, S. et al. Association between serum sodium level within normal range and handgrip strength in relation to hypertension status: a cross-sectional study. Sci Rep 11, 1088 (2021). https://doi.org/10.1038/s41598-020-80163-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-80163-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
