
Abstract
Chronic lymphocytic leukaemia (CLL) is characterised by a heterogeneous clinical course. Such heterogeneity is associated with a number of markers, including TP53 gene inactivation. While TP53 gene alterations determine resistance to chemotherapy, it is not clear whether they can influence early disease progression. To clarify this issue, TP53 mutations and deletions of the corresponding locus [del(17p)] were evaluated in 469 cases from the O-CLL1 observational study that recruited a cohort of clinically and molecularly characterised Binet stage A patients. Twenty-four cases harboured somatic TP53 mutations [accompanied by del(17p) in 9 cases], 2 patients had del(17p) only, and 5 patients had TP53 germ-line variants. While del(17p) with or without TP53 mutations was capable of significantly predicting the time to first treatment, a reliable measure of disease progression, TP53 mutations were not. This was true for cases with high or low variant allele frequency. The lack of predictive ability was independent of the functional features of the mutant P53 protein in terms of transactivation and dominant negative potential. TP53 mutations alone were more frequent in patients with mutated IGHV genes, whereas del(17p) was associated with the presence of adverse prognostic factors, including CD38 positivity, unmutated-IGHV gene status, and NOTCH1 mutations.
Similar content being viewed by others


Introduction
Decades of biological and molecular studies have provided extensive information for the understanding of chronic lymphocytic leukaemia (CLL), although many questions remain unanswered and the disease is still considered to be virtually incurable1. Despite the morphological and phenotypic homogeneity of CLL cells, the clinical course of the disease is highly heterogeneous ranging from rapid disease progression, requiring early treatment, to decades of survival with no treatment need2. This clinical course probably reflects the molecular heterogeneity of the disease. Over 80% of CLL cases harbour karyotype aberrations at diagnosis, the most frequent being partial deletions at 13q (~ 55%), 11q (~ 15%), 17p (~ 8%), and gain of chromosome 12 (~ 15%)3. In addition, specific gene mutations (e.g. TP53, SF3B1, BIRC3, NOTCH1, ATM) have been reported4. The incidence of TP53 tumour suppressor gene mutations is low at diagnosis (~ 5 to 7%), but it rises as the disease progresses and reaches approximately 40% in refractory CLL5,6,7,8,9. The European Research Initiative on CLL (ERIC) group recommends TP53 mutational screening for all patients before therapy start to avoid treatment protocols that are ineffective in patients with TP53 alterations10. Furthermore, since mutational status of the immunoglobulin heavy-chain variable region gene (IGHV) and complex karyotype are relevant to improve risk stratification11, Baliakas et al.12, have recently incorporated these two markers, and TP53 mutations into a novel prognostic model.
The TP53 tumour suppressor gene encodes a tetrameric transcription factor that controls different pathways, through its ability to transactivate a plethora of downstream effector genes, many of which are relevant for carcinogenesis13. Disruption of the P53 protein pathway, which may involve different mechanisms, is highly selected in most tumour types and is frequently due to alterations of both alleles, e.g. deletion of one allele [del(17p)] and mutation of the second allele. Donehower et al., performed a comprehensive assessment of the P53 pathway involvement in 32 cancers reported by The Cancer Genome Atlas (TCGA) and found that in cancers with TP53 mutations, there was a loss of the second allele due to mutation, chromosomal deletion, or copy-neutral loss of heterozygosity in 91% of the cases14. The current literature strongly supports the central role of TP53 alterations in CLL15. Approximately 90% of CLL patients with del(17p) carry a TP53 mutation and ~ 60% of patients with TP53 mutations also harbour del(17p), as detected by FISH16,17,18,19. Even in the absence of a del(17p), TP53 mutations appear to have an equally profound impact on outcome and are more frequent in patients with a poor prognosis and a higher genetic complexity8,20. Moreover, CLL sub-clones carrying TP53 mutations can be positively selected upon treatment, ultimately becoming the prevalent expansion of an initially minor mutant component 4,17,21,22.
The mere presence of TP53 mutations is not synonymous per se of the complete inactivation of the P53 pathway, since mutant P53 proteins are functionally and structurally heterogeneous23 and may impact on important clinical variables, in multiple, often subtle ways, as revealed by cell-based assays and animal models24. Moreover, while it is widely accepted that alterations of the TP53 gene may influence the clinical course of CLL by causing resistance to chemotherapy, their impact on clonal expansion and disease progression is still not fully defined, especially in the earliest stages of the disease. With the aim of clarifying these points, we studied TP53 alterations in patients enrolled in the O-CLL1 trial (clinicaltrial.gov identifier NCT00917540). In this observational protocol, Binet stage A CLL patients from several Italian Institutions were prospectively enrolled within 12 months of diagnosis (median: 2.3 months) and their evolution was followed. Because the aim of the protocol was to study the disease since the early stages, patients at more advanced stages (Binet stage B and C) were excluded from recruitment. A total of 469 patients from this well characterised cohort were investigated for TP53 mutations using next generation sequencing (NGS) and for del(17p) using FISH. The possible influence of the TP53 alterations on the time to first treatment (TTFT) and on the expansion of individual clones or sub-clones was also investigated.
Results
Incidence and characterization of the TP53 mutational status in O-CLL1 patients
Binet stage A CLL patients from the O-CLL1 trial25, were characterised for cellular, molecular, and cytogenetic features at diagnosis (Supplementary Table 1A). TP53 mutational status was determined by NGS on highly purified (> 95%) CLL B-cells from 475 patients. FISH analysis was used to determine the presence of del(17p) in 469 out of these 475 patients (Supplementary Table 1B). TP53 alterations [del(17p) and/or TP53 mutations] were identified in 31 patients. In five patients a TP53 variant allele frequency (VAF) of approximately 50% was suggestive of a germline variant. A subsequent analysis of non-tumour samples revealed the presence of the same TP53 mutation. Therefore, these were classified as TP53 germ-line variants (Supplementary Table 1B). The remaining 26 patients were characterised by the presence of: (1) only a TP53 mutation (group Mut/noDel = 15 cases), (2) a TP53 mutation along with the deletion of del(17p) (group Mut/Del = 9 cases), and (3) del(17p) with no TP53 mutation (group noMut/Del = 2 cases) (Table 1). The overall incidence of somatic TP53 alterations in the O-CLL1 cohort [mutations: 5%; 24/469; del(17p): 2.3%; 11/469] and their distribution relative to del(17p) were similar to that of previous reports4,16,17,21. The VAF in the Mut/noDel group was below 50% and significantly lower (23.8 ± 18.4 vs 65.7 ± 35.7, P = 0.001) than that observed in the Mut/Del group. In addition, certain adverse prognostic factors, such as CD38 expression (P = 0.0006), unmutated-IGHV (UM-IGHV) gene status (P = 0.003), and NOTCH1 mutations (P = 0.0415) were significantly less frequent in the cases with TP53 mutation only (Table 1). Conversely, a favourable prognostic factor, such as del(13q), showed a trend toward a higher frequency only in Mut/noDel cases (P = 0.06) (Table 1).
Influence of the TP53 status on the TTFT in O-CLL1 patients
Next, the influence of the TP53 status on TTFT was evaluated in the O-CLL1 cohort. After a median follow-up of 86 months, TTFT data were available for 462/469 patients, including the 5 cases with a TP53 germline variant. The TTFT of patients with somatic TP53 mutations (Mut = Mut/noDel + Mut/Del: 24 patients) was not statistically different from that of cases with wild-type TP53 (WT/noDel: 431 patients) (HR = 1.5, 95% CI 0.8–2.7, P = 0.7). In contrast, the TTFT was significantly shorter when patients with del(17p) (Del = Mut/Del + noMut/Del: 11 patients) were compared to those without deletion (noDel: 446 patients, excluding the 5 with TP53 germline variant) (HR = 5.2, 95% CI 2.4–11.2, P < 0.0001). A multivariate analysis, in which only the presence of del(17p) and of TP53 mutations were introduced, indicated that the presence of the del(17p) at diagnosis constituted a significant risk factor for a shorter TTFT (HR 6.1, 95% CI 2.2–17.0, P = 0.001), independently of the presence of a TP53 mutation (HR 0.8, 95% CI 0.4–1.8, P = 0.6). The cohort analysed was also stratified according to the presence/absence of TP53 mutations and/or del(17p) in different combinations (see Fig. 1). The 9 Mut/Del and the 2 WT/Del patients had a significantly shorter TTFT than the 431 WT/noDel cases, whereas a somatic TP53 mutation in the absence of del(17p) (Mut/noDel: 15 patients) was not predictive of a shorter TTFT. A similar result was obtained when the five cases with germ-line allelic variants were compared with the WT TP53 cases. Subsequently we addressed the issue of whether the VAF in the Mut/noDel cases could have an influence on the prediction of the TTFT. To this end Mut/noDel cases were stratified according to high (> 10%) and low (< 10%) VAF values and the TTFT of the two groups was analysed. No significant differences were detected in the TTFT in the two groups of patients. The clinical impact of TP53 mutations with different VAF also was analysed in the group of cases with mutated IGHV genes to eliminate a possible confounding factor represented by a strong predictor of prognosis such as IGHV gene mutation status. In this group, there were 9 patients with a VAF > 10% and 4 patients with a VAF < 10%. However, no statistically significant differences in the TTFT were observed (P = 0.5) (Supplementary Fig. 1). Therefore, the size of the subclone characterised by the presence of a TP53 mutation did not appear to influence the TTFT in Binet stage A CLL. The presence of del(17p), although mostly associated with a TP53 mutation, appears to be more deleterious than the presence of the a TP53 mutation itself in determining a shorter TTFT.

Analysis of the prognostic impact of TP53 alterations in the O-CLL1 cohort. Kaplan–Meier curves of cases differently clustered on the basis of the presence of a TP53 mutation and del(17p). O-CLL1 patients were divided in different groups: WT/noDel patients with neither a TP53 mutation nor del(17p); Mut/noDel and Mut (germline)/noDel, patients with a TP53 mutation (somatic or germline, respectively) and without del(17p); Mut/Del, patients that show both a TP53 mutation and del(17p); WT/Del, patients harbouring only del(17p).
Functional studies on mutant P53 proteins from O-CLL1 patients
Next, the functional properties of the P53 proteins encoded by the TP53 mutations detected in our cohort were investigated. A well-established yeast-based functional assay was employed, using four reporter strains. These strains have a different P53 Response Element (RE), which is derived from the promoter of one of four human P53 effector, i.e. P21, BAX, MDM2, and PUMA, respectively. The residual transactivation ability of the mutant P53 proteins compared to that of the WT protein (set as the 100% value) was measured at 30 °C and 37 °C (Table 2). With a threshold of residual WT P53 activity of 20%, all mutant P53 proteins (excluding those encoded by TP53 germline variants) were found inactive at 37 °C, whereas some activity was observed at 30 °C (Table 2; Supplementary Fig. 2A). In fact, five mutants encoded P53 proteins with residual activity (p.Ala161Thr, p.Pro191del, p.Arg213Leu, and p.Arg282Trp within the Mut/noDel group and p.Val272Leu within the Mut/Del group). Of note, the P53 protein encoded by all TP53 germline variants (p.Asn235Ser, p.Arg283Cys, and p.Gly360Val) behaved similarly to the WT P53 and were active at both 30 °C and 37 °C (Supplementary Table 3).
Mutant P53 proteins were also transiently expressed in HCT116 TP53−/− cells and were tested for their ability to transactivate the luciferase reporter gene carrying a fragment of the P21 promoter (Supplementary Fig. 2B). The results obtained were consistent with those obtained in yeast at 30 °C, confirming that some mutants (e.g. p.AlaA161Thr, p.Pro191del and p.Arg282Trp) had a partial activity. Finally, the TP53 germ-line allelic variants identified in our cohort were found to encode proteins with a high functional efficiency of transactivation (p.Asn235Ser, p.Arg283Cys, and p.Gly360Val) in both mammalian cell- and yeast-based assays (Supplementary Fig. 2B and Supplementary Table 3).
It is known that certain mutant P53 proteins have the capacity of inhibiting the activity of the WT protein when heterozygous at TP53 locus [i.e. they are Dominant Negative (DN)]26. Therefore, the DN potential of each mutant P53 protein of the Mut/noDel group was determined using one of the reporter strains (i.e. yLFM-P21-5′) (Table 3). None of the mutant P53 proteins with partial residual function (i.e. p.Ala161Thr, p.Pro191del, p.Arg213Leu, p.Val272Leu and p.Arg282Trp) exhibited DN potential (Table 3). Of note, all of the TP53 germline variants identified in patients without del(17p) encoded a recessive mutant P53 (Supplementary Table 4).
Influence of the residual transactivation ability and DN potential of mutant P53 proteins on TTFT in O-CLL1 patients
Given the functional heterogeneity of P53 proteins in our cohort, we asked whether such heterogeneity could influence the TTFT. This analysis was carried out on the Mut/noDel patients’ group (15 cases). Neither the transactivation ability (Fig. 2A) nor the DN potential (Fig. 2B) appeared to affect the Kaplan–Meier curves of these patients’ groups, which were similar to those of the WT/noDel patients (431 patients). Although potentially interesting, these tests could not be carried out in the Mut/Del patients’ group since the residual transactivation activity was < 20% in 8/9 available cases and ≥ 20% in a single case. Thus, this issue warrants re-evaluation in a larger study sample.

Influence of residual functionality of mutated P53 proteins on TTFT in O-CLL1 patients. Kaplan–Meier curves of cases belonging to the MUT/noDel group, clustered on the basis of (A) residual transactivation ability of the mutated P53 protein (≥ 20% versus < 20% with respect to WT P53) as determined in the yeast reporter strain yLFM-P21-5′; (B) dominant-negative (DN) or recessive (rec) classification of the mutated P53 protein, as determined in the yeast reporter strain yLFM-P21-5′.
Multivariate analysis
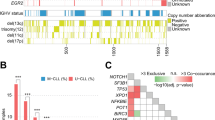
CD38 and ZAP-70 expression, β2-microglobulin (β2M) serum levels, Rai stage, IGHV mutational status, del(11q), NOTCH1 and SF3B1 mutations, MBL classification were confirmed to have a significant prognostic power on univariate analysis27 (Supplementary Table 5). A Cox multivariate analysis was then performed by introducing into the model markers indicative of TP53 alterations together with the variables with a significant prognostic power for TTFT determined in the univariate analysis. Both del(17p) together with TP53 mutations, and del(17p) alone, retained an independent prognostic power, whereas TP53 mutation alone did not. Other markers with an independent prognostic power were IGHV mutational status, del(11q), NOTCH1 mutation, β2M levels, and Rai stage (Fig. 3).

Analysis of the prognostic impact of TP53 alterations in O-CLL1 cohort study. Cox multivariate analysis of biological and clinical variables found to be significant on univariate analysis. Presence of a TP53 mutation associated with del(17p) was forced in the model as measure of P53 dysfunction.
Changes in the TP53 alterations pattern with time
TP53 mutational status was re-assessed in 171 patients after 36 months from diagnosis or at the time of therapy need. Of these, 140 re-tested at 36 months after diagnosis, did not present any new TP53 alteration. Another 23 cases, without TP53 alterations at diagnosis, were retested at the time of therapy need; again, no new TP53 alterations were recorded. Eight cases with a TP53 mutation at diagnosis were re-tested at 36 months (6 cases) or at the time of therapy need (2 cases). All of the 8 cases with a somatic TP53 mutation continued to express the same mutation seen at diagnosis, although with some changes in their VAF (Fig. 4). The 163 patients, negative for somatic TP53 mutations at diagnosis, still presented WT TP53 gene (or the same germline TP53 allelic variant) after 36 months. None of these 161 patients harboured del(17p) at diagnosis or at re-testing. The two cases re-tested at the time of therapy need presented p.Arg175His or p.Val157Asp, respectively. Of these, one [with p.Arg175His, and a del(17p) both at diagnosis and at re-testing] exhibited an over fourfold VAF increase, while the other [with p.Val157Asp mutation and no del(17p) also at re-testing] did not manifest any change in VAF.

Determination of variant allele frequency (VAF) at 36 months after diagnosis or at progression in O-CLL1 cohort study. TP53 mutational status was re-assessed in 171 patients by NGS after 36 months from the initial test or at disease progression. Presented are the 8 cases with a TP53 mutation at diagnosis, which continued to express the same mutation, albeit with some degree of clonal expansion. FISH analysis for del(17p) was repeated in all cases after 36 months (36 m, red bars) or at the time of therapy need (prog, red bars): none of the cases negative for del(17p) (Mut/noDel) became del(17p) positive. Percentage increase in the VAF of the samples analysed at 36 m/prog, compared to the samples at T0 (grey bars), are indicated in the figure only for cases in which it clearly occurred (CA0082, DD0478, GM0252, PA0254, PG0028). The increment was calculated according to the formula: (VAF 36 m/prog–VAF T0)/VAF 36 m/prog × 100. Of the two cases that experienced progression, PG0028 presented an increase of the percentage of del(17p) positive cells and of VAF (78%). The other case (AA0396) showed no increase in VAF.
Discussion
The present study investigated the influence on disease progression of TP53 alterations in Binet A CLL patients, enrolled in the multicentre prospective observational O-CLL1 trial with a long follow-up (median ~ 7 years). This influence was measured by determining the TTFT, which represents a rather accurate approach to assess disease progression. TP53 mutations and del(17p) were determined in 98.7% of patients (469/475). There are differences in the thresholds distinguishing positive from negative cases for the FISH and NGS analysis (i.e. measurement of del(17p) and TP53 mutations, respectively) due to the different sensitivity of each methodology. Since the sensitivity is somewhat imbalanced in favour of NGS, it cannot be excluded that certain patients harbour a del(17p), in addition to the TP53 mutation, but that the former lesion goes undetected by FISH being present at sub-threshold level in a small sub-clonal component. Therefore, all the categories of TP53 alterations dealt within the present paper refer to those detected within these technical limits. This admittedly may represent a limitation, especially in cases with VAF < 10%.
The overall incidence of somatic TP53 mutations [5% (24/469 patients)] and del(17p) [2.3% (11/469 patients)] in the O-CLL1 cohort and their relative distribution are similar to that of previous reports4,16,17,21. The majority of TP53 mutations were point mutations, causing a single amino-acid substitution in the P53 protein DNA binding domain. This was true for both the Mut/noDel and the Mut/Del patient groups. Although over 2,000 amino acid substitutions caused by a point mutation in the TP53 gene have been identified, 3 amino acid substitutions (p.Arg175His, p.Pro278Arg, and p.Ile195Thr) were shared by the Mut/noDel and Mut/Del patients’ groups.
The biological features of Mut/Del and Mut/noDel CLL patients were significantly different, since adverse prognostic factors, such as CD38 positivity (P = 0.006), UM-IGHV gene status (P = 0.003), and NOTCH1 mutations (P = 0.0415), were less frequently observed in the Mut/noDel patients’ group. We also observed that the TTFT of patients with mutated or WT TP53 gene was similar (P = 0.7), a finding which is in line with that of Brieghel et al.28, who demonstrated that TP53 mutations, determined by NGS, did not influence the clinical course of patients, in the absence of del(17p); this was true for cases with high (VAF ≥ 10%) and low (VAF < 10%) TP53 mutation burden28. We also did not find differences in the TTFT of Mut/noDel patients when they were stratified into two groups based upon high or low VAF, and this was also true for the patients with TP53 mutations from the mutated IGHV group stratified according to VAF values. Therefore, the size of the cell sub-clone bearing the TP53 mutations does not appear to influence disease progression for Binet stage A CLL patients. In this study, the TTFT of the patients with del(17p) was significantly shorter than that of patients without deletion (P < 0.0001), while del(17p) concomitant with a TP53 mutation represented, an additional and independent prognostic factor associated with shorter TTFT in multivariate analyses. However, in interpreting these data, it should be noted that most patients with del(17p) also had a TP53 mutation, and that only two cases had del(17p) without a TP53 mutation. Therefore, it is difficult to precisely evaluate the contribution of del (17p) alone to disease progression with this low number of cases. However, it is of note that Yu et al.29 reported that Mut/Del CLL patients had a TTFT shorter than that of the Mut/noDel patients. Moreover, Hoechstetter et al.30 showed that del(17p) is the highest weighted factor of the six considered in a multivariate analysis to predict TTFT and OS in Binet stage A CLL, although it requires the cooperation of additional factors to determine progression.
Unlike that reported in this and in the other studies quoted above, Dicker et al.18 and Rossi et al.5 reported that TP53 mutations alone were capable of predicting a shorter TTFT. These discrepancies are difficult to explain also given the differences in methodologies used, clinical study design, and cohorts investigated. However, it is worth underlining that a predominance of Binet B and C stage patients was included in those studies, whereas we focused on Binet A cases only.
The mutant P53 proteins encoded by TP53 mutations detected in this study were investigated further for their transactivation ability and DN potential. Although mutant P53 proteins appeared to be functionally heterogeneous, such heterogeneity was not associated with differences in TTFT within the Mut/noDel patients’ group. However, the interpretation of these data requires caution because of the relatively low number of Mut/noDel cases and further analyses in larger cohorts seem to be needed. Furthermore, it is worth recalling that mutant P53 proteins can acquire new functions favouring tumour cell expansion. These properties, indicated collectively as gain of function24, may in principle be present in CLL patients and perhaps have a higher incidence in more advanced cases. These too deserve analyses in large cohorts of patients.
IGHV mutational status represents a valuable prognostic marker for risk progression and outcome11. In the O-CLL1 cohort, the majority of cases with del(17p) had unmutated IGHV genes, whereas the majority of Mut/noDel cases had mutated IGHV genes. This finding may concur to explain why Mut/noDel cases progressed more slowly to the more advanced stages requiring therapy (Table 1). Furthermore, Mut/noDel cases were mostly negative for other unfavourable prognostic markers, whereas this was not the case for the group of patients with del(17p) (Mut/Del and WT/Del) (Table 1). These considerations may also help explain the discrepancies in the prognostic role of TP53 mutations between this study and those including Binet B and C patients. Since unmutated-IGHV cases are likely to progress more rapidly towards advanced stages31,32, it is possible that cases with mutated IGHV genes and TP53 mutations, that may not progress, are less frequently found in cohorts comprising numerous advanced cases.
Re-evaluation of 171 patients from this study following a 36 months interval or at the time of therapy need did not reveal any changes in TP53 alterations status. Specifically, there was neither an acquisition/loss of a TP53 mutation nor of del(17p). Only in one patient an expansion of a sub-clone carrying a non-functional TP53 mutation was observed at progression.
In conclusion, the present study based on a clinically and molecularly well-characterised Binet stage A CLL cohort demonstrates that the occurrence of del(17p) significantly predicted TTFT, while that of a TP53 mutation alone, was unable of such prediction.
Materials and methods
All methods were carried out in accordance with relevant guidelines and regulations.
Patients and CLL cells preparation
Only previously untreated Binet stage A CLL patients not requiring therapy according to NCI guidelines were prospectively enrolled within 12 months of diagnosis (O-CLL1 protocol, clinicaltrial.gov identifier NCT00917540). This protocol was presented by the Gruppo Italiano Studio dei Linfomi (GISL) on behalf of several Italian participating institutions and approved by the Ethics Review Committee (Comitato Etico Provinciale, Modena, Italy). Written informed consent was obtained from all patients in accordance with the declaration of Helsinki. The ethics committees from each participating centre (listed in the acknowledgements) approved this study. The median time between diagnosis and patient enrolment in the study was 2.3 months. A total of 420 (89.6%) and 386 (82.3%) patients had follow-up data at 1- and 2-year, respectively. Recruitment began in January 2007 and the criteria for CLL diagnosis employed followed the 1996 NCI/WG guidelines requiring > 5000 lymphocytes/µL in the peripheral blood. One hundred thirty-six cases (26%) fulfilled the definition of MBL (i.e. < 5.0 × 109 B lymphocytes/L in the peripheral blood and no apparent lymph node, spleen, or liver enlargement) according to the more recent NCI/IWCLL classification33. Treatment was decided uniformly for all participating centres based on documented progressive and symptomatic disease according to National Cancer Institute-sponsored working guidelines33. CLL cell phenotypes, CD38, and ZAP-70 expression, and IGHV mutational status assessment was centralised in the laboratory in Genoa, while all FISH assays were performed in Milan.
The median age of the entire cohort was 61.2 years, 214 cases (41%) were female. Finally, at the time of the present analysis, 179 cases (35.2%) progressed and were treated.
Ethical parameters
Ethical parameters, included in the synopsis of O-CLL1 protocol, clinicaltrial.gov identifier NCT00917540 were the following: It is responsibility of the investigator(s) to submit a copy of the protocol and detailed patient information sheet-consent form to an Independent Ethics Committee or Institutional Review Board in order to obtain independent approval to conduct the study. It is responsibility of the investigator(s) to ensure that the study is conducted in full conformance with the principles of the current version of the Declaration of Helsinki and to ensure that the study is performed in accordance with the international Good Clinical Practice (GCP) standards and according to all local laws and regulations concerning clinical studies).
CLL cells preparations
Peripheral blood mononuclear cells (PBMCs) from patients with CLL were isolated by Ficoll-Hypaque (Seromed, Biochrom) density gradient centrifugation. CD19-positive CLL cells were enriched by negative selection with the EasySep-Human B-cell Enrichment Kit without CD43 depletion (STEMCELL Technologies, Voden Medical Instruments S.p.A.), using the fully automated protocol of immunomagnetic cell separation with RoboSep (Stem Cell Technologies). The percentage of purified B Cells (CD19+) exceeded 95%, as detected by flow cytometry34.
CD38 and ZAP-70 determination, FISH analyses, NOTCH1 and SF3B1 mutations, and IGHV gene analysis
Heparinized blood samples were obtained and immediately shipped to the Genoa laboratory at room temperature, to arrive on the same or the following day; the cells were immediately processed. In these conditions, repeated quality control tests indicated minimal cell apoptosis or necrosis as measured by flow cytometric analysis using annexin V or propidium iodide (PI) staining. CD38 positive leukemic cells were measured by triple staining with CD19 fluorescein isothicyanate (FITC), CD38 phycoerythrin (PE), and CD5 Cy-Chrome (Becton Dickinson & Co., Sunnyvale, CA, USA). The cells were analysed using a FACS Calibur flow cytometer (Becton Dickinson & Co.) as previously described35. ZAP-70 was determined by flow-cytometry. CLL cells were first incubated with CD3 PE-CY7, CD19 PE and CD5 allophycocyanin (APC) monoclonal antibodies (mAbs) (Becton Dickinson & Co.), fixed, permeabilised with Fix and Perm reagents (Caltag Laboratories) and exposed to a ZAP-70 FITC (Upstate, Lake Placid, NY, USA) or an isotype control mAb (mouse IgG2a FITC; Becton Dickinson). Cytogenetic abnormalities involving deletions at chromosomal loci 11q22.3, 13q14.3, 17p13.1, and trisomy 12 were evaluated by FISH in a purified CD19+ population, as previously described36. The FISH study was performed using the protocol provided by the manufacturer of the multicolour probes LSI D13S25/LSI 13q34, LSIp53/CEP17, LSI ATM/CEP11, and CEP12 (Abbot Park, IL, USA). A total of 200 interphase nuclei were analysed for each probe set. The cut-off points (mean + 3 standard deviations) for positive values assessed on peripheral mononuclear cells from ten control subjects were 3.4%, 1.7%, 3.8% and 3.4% for + 12, del(11q), del(13q), and del(17p), respectively36.
IGHV mutational status was assessed using cDNA, as previously described37. Sequences were aligned to the IMGT directory and analysed using IMGT/VQUEST software. SF3B1 (exons 14, 15, and 16, including splice sites; RefSeq NM_012433.2) genes were analysed by PCR amplification and Sanger sequencing of high molecular weight genomic DNA extracted from CD19+ purified B-cells (> 95%) as previously described38. The NOTCH1 c.7541_7542delCT mutation was tested by NGS using Roche 454 technology and subsequently validated by Amplification Refractory Mutation System (ARMS)-PCR as previously described39.
Evaluation of TP53 mutations
The TP53 mutational status of all cases (n = 475) was analysed by NGS using Roche Junior (Roche-454 Life Sciences, Penzberg, Germany) in 250 cases as previously described40 and by the Ion Torrent platforms (Thermo Fisher Scientific Carlsbad, CA) in 241 cases (see https://tools.thermofisher.com/content/sfs/manuals/MAN0013432_Ion_AmpliSeq_Library_Prep_on_Ion_Chef_UG.pdf for further details). Sixteen cases were tested using both platforms with 100% concordance. Briefly, TP53 libraries were prepared using genomic DNA extracted from CD19+ purified B cells (QIAamp DNA Blood Mini Kit, Qiagen Hilden, Germany) according to the respective protocols (see above) and then sequenced with both NGS platforms taking into account the achievement of a threshold of 500 reads for each TP53 amplicon. Cases with VAF ≥ 2% were considered positive for TP53 mutation; in addition, samples with TP53 variant < 10% VAF were re-evaluated by a second NGS run. The panel utilized for the Ion torrent NGS study was the Ion AmpliSeq™ TP53 Panel comprising 24 primer pairs across 2 pools that provides 100% of coverage of exons 2–11 and exon–intron boundaries (± 30 bp padding). The TP53 primer panel applied to Roche NGS technology spanned exons 4 to 940. Of the 171 cases sequenced (131 with Roche J, 51 with Ion Torrent, 11 were subsequently analysed using both sequencing approaches with concordant results), TP53 status was determined not only at the time of diagnosis, but also after 36 months or at the time of therapy need. Any TP53 variant identified [exonic, intronic and frequent SNPs (e.g. Pro72Arg)] identified by NGS, was recorded for each sample. For all samples in which the variant was verified, and the VAF was approximately 50%, suggesting a germline origin, the patient-matched normal tissue DNA was subsequently analysed by NGS. For patients CG0015 and RA0023, DNA was obtained from buccal swabs (3 separate swabs per patient). For GS0473, RC0479, and NF0056 non-tumour DNA was obtained from CD3+ cells obtained by triple staining with CD19, CD5, and CD3 mAbs (Becton Dickinson) followed by cell sorting (FACS ARIA II, Becton Dickinson) of CD3+ CD5+ cells to avoid any contamination of CD19+ CD5+ neoplastic cells10. No mutations in exons 2, 3, or 11 were identified by Ion Torrent NGS among the 241 CLL cases analysed using this platform, while in only one case (1/241, 0.4%) a germline variant, was discovered in exon 10. This suggests that there was a number of mutated samples, possibly not being detected by sequencing of exons 4–9 with the Roche platform, that was negligible or non-existing, and that the results obtained with the two methods were comparable. Overall, sequencing of the entire coding portion of the gene using the Ion AmpliSeq™ TP53 Panel indicated that exons 4–8 were the most recurrently mutated. The functional analysis, performed using a yeast-based assay, was applied, to those TP53 variants causing either amino-acid substitutions or coding for a truncated P53 protein.
Evaluation of P53 function in a yeast-reporter assay
Yeast strains and media
The yLFM-P21-5′, yLFM-PUMA, yLFM-MDM2P2C, and yLFM-BAX A + B yeast strains were used to assess the functionality of TP53 variants: all strains were isogenic except for the different P53 response element (RE) located upstream of the luciferase reporter gene (LUC1). Cells were grown in YPDA medium (1% yeast extract, 2% peptone, 2% dextrose, 200 mg/L adenine) or in selective medium (with or without 2% agar) containing dextrose or raffinose as a carbon source plus adenine (200 mg/L), but in the absence of tryptophan and/or leucine (Sigma-Aldrich, Saint Louis, Missouri, USA; Biokar Diagnostics, Allonne, France). Galactose (Sigma-Aldrich, Saint Louis, Missouri, USA) was added to the medium to modulate P53 expression under the inducible GAL1,10 promoter.
Yeast vectors
For the transactivation assay, human WT and mutant P53 proteins were expressed using a pTSG-based vector (TRP1). The P53 mutants were constructed in the pTSG-based vector (through SgraI/StuI digestion and subsequent ligation) (New England Biolabs) from available pLS-based vector26,41. When cloned mutants were not available, P53 mutants were firstly constructed in a pLS- or pTS-based vector exploiting in vivo yeast homologous recombination, as previously described42 and then cloned (through SgraI/StuI or XhoI/NotI digestion and subsequent ligation) (New England Biolabs) in the pTSG-based vector.
For the dominance assay, P53 mutant protein was expressed using a pLS- or pTS-based vector; the pLS89 (TRP1) or pLLS89 (LEU2) expressing WT P53 protein under the inducible GAL1,10 promoter was co-transformed in yeast, based on the previously used selection marker. Plasmid pRS314 (TRP1) and pRS315 (LEU2) were used as empty vectors. The list of primers used to construct pLS- or pTS-based P53 mutant vectors is available upon request.
Yeast functional assay
Quantitative functional assays (evaluation of transactivation ability and DN potential) were performed according to the miniaturized protocol we developed43. The transactivation activity of a mutant P53 was measured by calculating the percentage with respect to WT P53 (set as 100%); the DN potential was calculated by comparing the net activity of WT and mutant P53 co-expression with respect to the expression of WT P53 alone (set as 100%). A mutant P53 was defined as recessive or dominant when the net activity was above or below 100%, respectively.
Evaluation of P53 function in a mammalian reporter-assay
Cell line and media
HCT116 TP53−/− cells (human colon carcinoma) were obtained from Dr. B. Vogelstein (The Johns Hopkins Kimmel Cancer Center, Baltimore, MD). Cells were grown in RPMI containing 10% foetal bovine serum, L-glutamine, and a penicillin–streptomycin antibiotic mixture (Euroclone, Milano, Italy), and maintained at 37 °C in 5% CO2 at 100% humidity.
Mammalian expression and reporter vectors
A pCIneo-based (Promega) vector was used to express WT and mutant P53 in mammalian cells. Plasmids expressing mutant P53 were constructed as previously described42. The pGL3-1138 and the pRL-SV40 plasmids were used as reporter (P21 promoter) and normalization vectors, respectively44.
Mammalian functional assay
HCT116 TP53−/− cells transfected with pCI-neo-based P53 expression vectors, the reporter, and normalization plasmids, were collected and washed with cold PBS. Lysis was performed in 1X PLB buffer (Passive Lysis Buffer, Promega). Luciferase assays were conducted as previously described45.
Statistical analysis
Statistical analyses were performed as previously described25,27. Briefly, SPSS for Windows, v13.0, 2004 software (SPSS, UK) was used for all the analyses. We performed, statistical comparisons, for categorical variables, using two-way tables for the Fisher's exact test, while multiway tables were used for the Pearson's Chi-square test. TTFT analyses were performed using the Kaplan–Meier method in patients with a minimum follow-up. Using the log‐rank test, we calculated the statistical significance of associations between individual variables and survival. We investigated the prognostic impact for the outcome variable by univariate and multiple Cox regression analysis. Data were expressed as hazard ratio (HR) and 95% confidence interval (CI). A value of P < 0.05 was considered statistically significant.
References
Chiorazzi, N., Rai, K. R. & Ferrarini, M. chronic lymphocytic leukemia. N. Engl. J. Med. 352, 804–815 (2005).
Gentile, M. et al. Validation of a biological score to predict response in chronic lymphocytic leukemia patients treated front-line with bendamustine and rituximab. Leukemia 32, 1869–1873 (2018).
Döhner, H. et al. Genomic aberrations and survival in chronic lymphocytic leukemia. N. Engl. J. Med. 343, 1910–1916 (2000).
Nadeu, F. et al. Clinical impact of clonal and subclonal TP53, SF3B1, BIRC3, NOTCH1, and ATM mutations in chronic lymphocytic leukemia. Blood 127, 2122–2130 (2016).
Rossi, D. et al. The prognostic value of TP53 mutations in chronic lymphocytic leukemia is independent of Del17p13: Implications for overall survival and chemorefractoriness. Clin. Cancer Res. 15, 995–1004 (2009).
Zenz, T. et al. TP53 mutation profile in chronic lymphocytic leukemia: Evidence for a disease specific profile from a comprehensive analysis of 268 mutations. Leukemia 24, 2072–2079 (2010).
Pospisilova, S. et al. ERIC recommendations on TP53 mutation analysis in chronic lymphocytic leukemia. Leukemia 26, 1458–1461 (2012).
Stilgenbauer, S. et al. Gene mutations and treatment outcome in chronic lymphocytic leukemia: Results from the CLL8 trial. Blood 123, 3247–3254 (2014).
Buccheri, V. et al. Prognostic and therapeutic stratification in CLL: Focus on 17p deletion and p53 mutation. Ann. Hematol. 97, 2269–2278 (2018).
Malcikova, J. et al. ERIC recommendations for TP53 mutation analysis in chronic lymphocytic leukemia—Update on methodological approaches and results interpretation. Leukemia 32, 1070–1080 (2018).
Sutton, L.-A. et al. Immunoglobulin genes in chronic lymphocytic leukemia: Key to understanding the disease and improving risk stratification. Haematologica 102, 968–971 (2017).
Baliakas, P. et al. Cytogenetic complexity in chronic lymphocytic leukemia: Definitions, associations, and clinical impact. Blood 133, 1205–1216 (2019).
Lane, D. P. p53, guardian of the genome. Nature 358, 15–16 (1992).
Donehower, L. A. et al. Integrated analysis of tp53 gene and pathway alterations in the cancer genome atlas. Cell Rep. 28, 1370-1384.e5 (2019).
Lodé, L., Cymbalista, F. & Soussi, T. Genetic profiling of CLL: A ‘TP53 addict’ perspective. Cell Death Dis. 7, e2042–e2042 (2016).
Zenz, T. et al. Monoallelic TP53 inactivation is associated with poor prognosis in chronic lymphocytic leukemia: Results from a detailed genetic characterization with long-term follow-up. Blood 112, 3322–3329 (2008).
Malcikova, J. et al. Monoallelic and biallelic inactivation of TP53 gene in chronic lymphocytic leukemia: Selection, impact on survival, and response to DNA damage. Blood 114, 5307–5314 (2009).
Dicker, F. et al. The detection of TP53 mutations in chronic lymphocytic leukemia independently predicts rapid disease progression and is highly correlated with a complex aberrant karyotype. Leukemia 23, 117–124 (2009).
Zainuddin, N. et al. TP53 mutations are infrequent in newly diagnosed chronic lymphocytic leukemia. Leuk. Res. 35, 272–274 (2011).
Sutton, L.-A. & Rosenquist, R. The complex interplay between cell-intrinsic and cell-extrinsic factors driving the evolution of chronic lymphocytic leukemia. Semin. Cancer Biol. 34, 22–35 (2015).
Rossi, D. et al. Clinical impact of small TP53 mutated subclones in chronic lymphocytic leukemia. Blood 123, 2139–2147 (2014).
Puente, X. S. et al. Non-coding recurrent mutations in chronic lymphocytic leukaemia. Nature 526, 519–524 (2015).
Leroy, B. et al. The TP53 website: An integrative resource centre for the TP53 mutation database and TP53 mutant analysis. Nucleic Acids Res. 41, D962-969 (2013).
Bisio, A., Ciribilli, Y., Fronza, G., Inga, A. & Monti, P. TP53 mutants in the tower of babel of cancer progression. Hum. Mutat. 35, 689–701 (2014).
Morabito, F. et al. Clinical monoclonal B lymphocytosis versus Rai 0 chronic lymphocytic leukemia: A comparison of cellular, cytogenetic, molecular, and clinical features. Clin. Cancer Res. 19, 5890–5900 (2013).
Monti, P. et al. dominant-negative features of mutant TP53 in germline carriers have limited impact on cancer outcomes. Mol. Cancer Res. 9, 271–279 (2011).
Lionetti, M. et al. Frequency and clinical relevance of coding and noncoding NOTCH1 mutations in early stage Binet A chronic lymphocytic leukemia patients. Hematol. Oncol. https://doi.org/10.1002/hon.2722 (2020).
Brieghel, C. et al. Deep targeted sequencing of TP53 in chronic lymphocytic leukemia: Clinical impact at diagnosis and at time of treatment. Haematologica 104, 789–796 (2019).
Yu, L. et al. Survival of Del17p CLL depends on genomic complexity and somatic mutation. Clin. Cancer Res. 23, 735–745 (2017).
Hoechstetter, M. A. et al. Prognostic model for newly diagnosed CLL patients in Binet stage A: Results of the multicenter, prospective CLL1 trial of the German CLL study group. Leukemia https://doi.org/10.1038/s41375-020-0727-y (2020).
Best, O. G. et al. A subset of Binet stage A CLL patients with TP53 abnormalities and mutated IGHV genes have stable disease. Leukemia 23, 212–214 (2009).
Trbusek, M. et al. missense mutations located in structural p53 DNA-binding motifs are associated with extremely poor survival in chronic lymphocytic leukemia. JCO 29, 2703–2708 (2011).
Hallek, M. Chronic lymphocytic leukemia: 2020 update on diagnosis, risk stratification and treatment. Am. J. Hematol. 94, 1266–1287 (2019).
Cutrona, G. et al. Effects of miRNA-15 and miRNA-16 expression replacement in chronic lymphocytic leukemia: implication for therapy. Leukemia 31, 1894–1904 (2017).
Cutrona, G. et al. Clonal heterogeneity in chronic lymphocytic leukemia cells: Superior response to surface IgM cross-linking in CD38, ZAP-70-positive cells. Haematologica 93, 413–422 (2008).
Fabris, S. et al. Multiplex ligation-dependent probe amplification and fluorescence in situ hybridization to detect chromosomal abnormalities in Chronic lymphocytic leukemia: A comparative study. Genes Chromosom. Cancer 50, 726–734 (2011).
Fais, F. et al. Chronic lymphocytic leukemia B cells express restricted sets of mutated and unmutated antigen receptors. J. Clin. Invest. 102, 1515–1525 (1998).
Rossi, D. et al. Mutations of the SF3B1 splicing factor in chronic lymphocytic leukemia: Association with progression and fludarabine-refractoriness. Blood 118, 6904–6908 (2011).
Lionetti, M. et al. High-throughput sequencing for the identification of NOTCH1 mutations in early stage chronic lymphocytic leukaemia: Biological and clinical implications. Br. J. Haematol. 165, 629–639 (2014).
Lionetti, M. et al. Molecular spectrum of TP53 mutations in plasma cell dyscrasias by next generation sequencing: An Italian cohort study and overview of the literature. Oncotarget 7, 666 (2016).
Monti, P. et al. Yeast as a chassis for developing functional assays to study human P53. J. Vis. Exp. https://doi.org/10.3791/59071 (2019).
Marengo, B. et al. Etoposide-resistance in a neuroblastoma model cell line is associated with 13q14.3 mono-allelic deletion and miRNA-15a/16–1 down-regulation. Sci. Rep. 8, 13762 (2018).
Andreotti, V. et al. p53 transactivation and the impact of mutations, cofactors and small molecules using a simplified yeast-based screening system. PLoS ONE 6, e20643 (2011).
Monti, P. et al. EEC- and ADULT-associated TP63 mutations exhibit functional heterogeneity toward P63 responsive sequences. Hum. Mutat. 34, 894–904 (2013).
Foggetti, G. et al. Gambogic acid counteracts mutant p53 stability by inducing autophagy. Biochim. Biophys. Acta Mol. Cell Res. 1864, 382–392 (2017).
Acknowledgements
In addition to the listed Authors, the following Investigators participated in this study as part of the Gruppo Italiano Studio Linfomi (GISL): Gianni Quintana, Divisione di Ematologia, Presidio Ospedaliero “A.Perrino”, Brindisi; Giovanni Bertoldero, Dipartimento di Oncologia, Ospedale Civile, Noale, Venezia; Paolo Di Tonno, Dipartimento di Ematologia, Ospedale di Venere, Bari; Robin Foà and Francesca R Mauro, Divisione di Ematologia, Università La Sapienza, Roma; Nicola Di Renzo, Unità di Ematologia, Ospedale Vito Fazzi, Lecce; Maria Cristina Cox, Ematologia, A.O. Sant’Andrea, Università La Sapienza, Roma; Stefano Molica, Dipartimento di Oncologia ed Ematologia, Pugliese-Ciaccio Hospital, Catanzaro; Attilio Guarini, Unità di Ematologia e Trapianto di Cellule Staminali, Istituto di Oncologia “Giovanni Paolo II”, Bari; Antonio Abbadessa, U.O.C. di Oncoematologia Ospedale “S. Anna e S. Sebastiano”, Caserta; Francesco Iuliano, U.O.C. di Oncologia, Ospedale Giannettasio, Rossano Calabro, Cosenza; Omar Racchi, Ospedale Villa Scassi Sampierdarena, Genova; Mauro Spriano, Ematologia, A.O. San Martino, Genova; Felicetto Ferrara, Divisione di Ematologia, Ospedale Cardarelli, Napoli; Monica Crugnola, Ematologia, CTMO, Azienda Ospedaliera Universitaria di Parma; Alessandro Andriani, Dipartimento di Ematologia, Ospedale Nuovo Regina Margherita, Roma; Nicola Cascavilla, Unità di Ematologia e Trapianto di Cellule Staminali, IRCCS Ospedale Casa Sollievo della Sofferenza, San Giovanni Rotondo; Lucia Ciuffreda, Unità di Ematologia, Ospedale San Nicola Pellegrino, Trani; Graziella Pinotti, U.O. Oncologia Medica, Ospedale di Circolo Fondazione Macchi, Varese; Anna Pascarella, Unità Operativa di Ematologia, Ospedale dell'Angelo, Venezia-Mestre; Maria Grazia Lipari, Divisione di Ematologia, Ospedale Policlinico, Palermo, Francesco Merli, Unità Operativa di Ematologia, A.O.S. Maria Nuova, Reggio Emilia; Luca Baldini Istituto di Ricovero e Cura a Carattere Scientifico Cà Granda-Maggiore Policlinico, Milano; Caterina Musolino, Divisione di Ematologia, Università di Messina; Agostino Cortelezzi, Ematologia and CTMO, Foundation IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milano; Francesco Angrilli, Dipartimento di Ematologia, Ospedale Santo Spirito, Pescara; Ugo Consoli, U.O.S. di Emato-Oncologia, Ospedale Garibaldi-Nesima, Catania; Gianluca Festini, Centro di Riferimento Ematologico-Seconda Medicina, Azienda Ospedaliero-Universitaria, Ospedali Riuniti, Trieste; Giuseppe Longo, Unità di Ematologia, Ospedale San Vincenzo, Taormina; Daniele Vallisa and Annalisa Arcari, Unità di Ematologia, Dipartimento di Onco-Ematologia, Guglielmo da Saliceto Hospital, Piacenza; Francesco Di Raimondo and Annalisa Chiarenza, Divisione di Ematologia, Università di Catania Ospedale Ferrarotto, Catania; Iolanda Vincelli, Unità di Ematologia, A.O. of Reggio Calabria; Donato Mannina, Divisione di Ematologia, Ospedale Papardo, Messina, Italy. For Each Institution, the Ethics Review Committee that approved the protocol is listed below. Unità di Ematologia e Trapianto di Cellule Staminali, Istituto di Oncologia “Giovanni Paolo II”, Bari comitato etico Istituto di Oncologia “Giovanni Paolo II”, di Bari, Italy; Dipartimento di Ematologia, Ospedale di Venere, Bari comitato etico Ospedale di Venere,Bari, Italy; U.O.C. Ematologia e Trapianto, Ospedale "Mons. R. Dimiccoli" -Barletta comitato etico Ospedale "Mons. R. Dimiccoli" -Barletta, Italy; Divisione di Ematologia, Presidio Ospedaliero “A. Perrino”, Brindisi comitato etico Presidio Ospedaliero “A. Perrino”, Brindisi, Italy; U.O.C. di Oncoematologia Ospedale “S. Anna e S. Sebastiano”, Caserta comitato etico Ospedale “S. Anna e S. Sebastiano”, Caserta, Italy; Divisione di Ematologia, Università di Catania Ospedale Ferrarotto, Catania comitato etico Ospedale Ferrarotto, Catania, Italy; U.O.S. di Emato-Oncologia, Ospedale Garibaldi-Nesima, Catania comitato etico Ospedale Garibaldi-Nesima, Catania, Italy, Dipartimento di Oncologia ed Ematologia, Pugliese-Ciaccio Hospital, Catanzaro comitato etico Pugliese-Ciaccio Hospital, Catanzaro, Italy; U.O.C di Ematologia , A.O. Cosenza comitato etico A.O. Cosenza, Italy; U.O.C. di Oncologia, Ospedale Giannettasio, Rossano Calabro, Cosenza comitato etico Ospedale Giannettasio, Rossano Calabro, Italy; Divisione di Ematologia, Ospedale Policlinico, Palermo, comitato etico Ospedale Policlinico, Palermo, Italy; Ematologia ospedale Goretti, Latina comitato etico ospedale Goretti, Latina, Italy; Clinica Ematologica, DIMI, Genova, comitato etico Ospedale San Martino, Genova, Italy; Oncologia medica C IRCCS Ospedale Policlinico San Martino, Genoa, Italy comitato etico IRCCS Ospedale Policlinico San Martino,Genova, Italy; Ospedale Villa Scassi Sampierdarena, Genova comitato etico Ospedale Villa Scassi, Genova, Italy; Ematologia, A.O. San Martino, Genova comitato etico A.O. San Martino, Genova, Italy; Unità di Ematologia, Ospedale Vito Fazzi, Lecce comitato etico Ospedale Vito Fazzi, Lecce, Italy; UOC di Ematologia Ospedale di Matera comitato etico Ospedale di Matera, Italy; Divisione di Ematologia, Ospedale Papardo, Messina, Italy. comitato etico Ospedale Papardo, Messina, Italy; Divisione di Ematologia, Università di Messina comitato etico Ospedale di Messina, Italy; Ematologia and CTMO, Foundation IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milano comitato etico Ospedale Maggiore Policlinico di Milano, Italy; Dipartimento di Oncologia, Ospedale Civile, Noale, Venezia comitato etico Ospedale Civile, Noale, Italy; Oncoematologia Policlinico di Modena comitato etico provinciale di Modena, Italy; Divisione di Ematologia, Ospedale Cardarelli, Napoli comitato etico Ospedale Cardarelli, Napoli, Italy; Ematologia, CTMO, Azienda Ospedaliera Universitaria di Parma comitato etico Azienda Ospedaliera Universitaria di Parma, Italy; Dipartimento di Ematologia, Ospedale Santo Spirito, Pescara comitato etico Ospedale Santo Spirito, Pescara, Italy; Unità di Ematologia, Dipartimento di Onco-Ematologia, Guglielmo da Saliceto Hospital, Piacenza comitato etico Guglielmo da Saliceto Hospital, Piacenza, Italy; Unità di Ematologia, A.O. of Reggio Calabria comitato etico A.O. of Reggio Calabria, Italy; Unità Operativa di Ematologia, A.O.S. Maria Nuova, Reggio Emilia comitato etico A.O.S. Maria Nuova, Reggio Emilia, Italy; S.C. di Ematologia e Trapianto di Cellule Staminali IRCCS-CROB di Rionero in Vulture, Potenza comitato etico IRCCS-CROB di Rionero in Vulture, Italy; Dipartimento di Ematologia, Ospedale Nuovo Regina Margherita, Roma comitato etico Ospedale Nuovo Regina Margherita, Roma, Italy; Ematologia, A.O. Sant’Andrea, Università La Sapienza, Roma comitato etico A.O. Sant’Andrea, Roma, Italy; Divisione di Ematologia, Università La Sapienza, Roma comitato etico Università La Sapienza, Roma, Italy; Unità di Ematologia e Trapianto di Cellule Staminali, IRCCS Ospedale Casa Sollievo della Sofferenza, San Giovanni Rotondo comitato etico IRCCS Ospedale Casa Sollievo della Sofferenza, San Giovanni Rotondo, Italy; Unità di Ematologia, Ospedale San Vincenzo, Taormina, comitato etico Ospedale San Vincenzo, Taormina, Italy;Unità di Ematologia, Ospedale San Nicola Pellegrino, Trani comitato etico Ospedale San Nicola Pellegrino, Trani, Italy; Centro di Riferimento Ematologico-Seconda Medicina, Azienda Ospedaliero-Universitaria, Ospedali Riuniti, Trieste comitato etico Ospedali Riuniti, Trieste, Italy; U.O. Oncologia Medica, Ospedale di Circolo Fondazione Macchi, Varese comitato etico Ospedale di Circolo Fondazione Macchi, Varese, Italy; Unità Operativa di Ematologia, Ospedale dell'Angelo, Venezia-Mestre comitato etico Ospedale dell'Angelo, Venezia-Mestre, Italy; Istituto di Ricovero e Cura a Carattere Scientifico Cà Granda-Maggiore Policlinico, Milano comitato etico Policlinico, Milano, Italy.
Funding
This work was supported by: Associazione Italiana Ricerca sul Cancro (AIRC) Grant 5 × mille n.9980, (to M.F., F.M., and A.N.); AIRC I.G. n.14326 (to M.F.), n.15426 (to F.F.), and n. 5506 (to G.F.); AIRC and Fondazione CaRiCal co-financed Multi-Unit Regional Grant 2014 n.16695 (to F.M.); Italian Ministry of Health 5 × 1000 funds 2013 (to G.F.) 2014 (to G.C, S.Z. and. A.I.), 2015 (to F.F. S.Z., and G.F.) and 2016 (to F.F., G.C. and G.F.); Italian Ministry of Health Alleanza Contro il Cancro (ACC), hematology network; Current Research 2016 to G.F.; and 2016 (to F.F. and G.C.); Compagnia S. Paolo Turin Italy project 2017.0526 (to G.F.); Gilead fellowship program 2016 (M.C) and 2017 (G.C.).
Author information
Authors and Affiliations
Contributions
M.L., G.DeL., S.M.M.C.S.F., M.B., S. Z., A.G.R., and M.D. performed biological characterization (including NGS sequencing and cytogenetic analysis) of CLL samples. PMo PMe, and AS were involved in the functional characterisation of mutant P53; M.G., A.I., A.N. M.F., and F.M. were involved at the clinical level; M.F. e F.M. were P.I. of the OCLL1 clinical Trial; FM performed statistical analysis; M.F., F.F., G.F., G.C. and F.M. conceived the study and discussed the results. G.F. and F.M. wrote the paper. All authors critically read the manuscript, suggested changes and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Monti, P., Lionetti, M., De Luca, G. et al. Time to first treatment and P53 dysfunction in chronic lymphocytic leukaemia: results of the O-CLL1 study in early stage patients. Sci Rep 10, 18427 (2020). https://doi.org/10.1038/s41598-020-75364-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-75364-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
