
Abstract
COPD is associated with disturbed tissue repair, possibly due to TGF-β-regulated miRNA changes in fibroblasts. Our aim was to identify TGF-β-regulated miRNAs and their differential regulation and expression in COPD compared to control fibroblasts. Small RNA sequencing was performed on TGF-β-stimulated and unstimulated lung fibroblasts from 15 COPD patients and 15 controls. Linear regression was used to identify TGF-β-regulated and COPD-associated miRNAs. Interaction analysis was performed to compare miRNAs that responded differently to TGF-β in COPD and control. Re-analysis of previously generated Ago2-IP data and Enrichr were used to identify presence and function of potential target genes in the miRNA-targetome of lung fibroblasts. In total, 46 TGF-β-regulated miRNAs were identified in COPD and 86 in control fibroblasts (FDR < 0.05). MiR-27a-5p was the most significantly upregulated miRNA. MiR-148b-3p, miR-589-5p and miR-376b-3p responded differently to TGF-β in COPD compared to control (FDR < 0.25). MiR-660-5p was significantly upregulated in COPD compared to control (FDR < 0.05). Several predicted targets of miR-27a-5p, miR-148b-3p and miR-660-5p were present in the miRNA-targetome, and were mainly involved in the regulation of gene transcription. In conclusion, altered TGF-β-induced miRNA regulation and differential expression of miR-660-5p in COPD fibroblasts, may represent one of the mechanisms underlying aberrant tissue repair and remodelling in COPD.
Similar content being viewed by others


Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by a variable extent and combination of (small) airway disease and emphysema. It is a major and still growing cause of death worldwide1,2. One of the features underlying the development of COPD is aberrant tissue repair and remodelling3, leading to a disturbed extracellular matrix (ECM) homeostasis. In COPD patients, narrowing of the (small) airways is observed, due to airway wall fibrosis4. In contrast, proper tissue repair is diminished in the parenchyma contributing to the development of pulmonary emphysema4,5. Malfunction of lung fibroblasts through dysregulation of the TGF-β signalling pathway may be pivotal to this aberrant tissue repair and remodelling5. Lung fibroblasts are the principal cells in controlling ECM homeostasis by producing ECM proteins, matrix metalloproteases and tissue inhibitors of matrix metalloproteases. Transforming growth factor-β (TGF-β) is the main inducer of ECM production in lung fibroblasts. TGF-β levels are increased in COPD5,6,7,8 and alterations in the TGF-β signalling pathway have been demonstrated in COPD compared to control fibroblasts9.
MicroRNAs (miRNAs) regulate the vast majority of cellular processes and pathways by negatively influencing protein expression of multiple target genes10. These small non-coding RNAs play a role in various human diseases11. Several studies suggested that miRNAs contribute to COPD pathogenesis based on differential expression in e.g. whole blood, bronchoalveolar lavage cell fraction and lung tissue from COPD patients compared to smoking controls12,13. Previously, Ikari et al. compared miRNA expression changes between COPD and control fibroblasts (n = 5 per group)14 and selected miR-503, which was decreased in COPD fibroblasts, for further validation15. MiR-503 was demonstrated to enhance the production of VEGF, a direct target of miR-50315. Apart from these findings on miRNA expression in lung fibroblasts, limited information on differential miRNA expression in COPD fibroblasts is available. In our previous study, we identified 29 TGF-β-regulated miRNAs in primary parenchymal lung fibroblasts from control subjects16. Of these miRNAs, miR-455-3p and miR-21-3p were shown to target genes that are involved in the TGF-β and WNT signalling pathways, indicating a role of these miRNAs in tissue repair16. We hypothesize that TGF-β-regulated changes in miRNA expression in lung fibroblasts are involved in the pathogenesis of COPD.
To better understand the alterations in the TGF-β-regulated tissue repair response in COPD, it is of interest to identify miRNAs that are regulated by TGF-β in COPD and control lung fibroblasts and to identify miRNAs that are differentially regulated by TGF-β in COPD compared to control fibroblasts. In the present study, we used small RNA sequencing analysis; (1) to identify TGF-β-regulated miRNAs in clinically well-characterized severe COPD and control fibroblasts, (2) to identify which miRNAs are differentially regulated by TGF-β between COPD and control fibroblasts and (3) to determine miRNAs differentially expressed between COPD and control fibroblasts.
Results
Subject characteristics
Clinical characteristics of the 30 lung fibroblast and 35 lung tissue donors are shown in Table 1. Six of the lung fibroblasts donors in the control group were current smokers. The other 24 lung fibroblasts donors and all lung tissue donors were ex-smokers. No differences were identified in age and number of pack-years between controls and COPD patients, and also not between lung fibroblast and lung tissue donors.
Differentially expressed miRNAs in response to TGF-β stimulation
As a control of successful TGF-β stimulation we first analysed the expression of fibronectin-1 (FN1), collagen type I alpha I (COL1A1), and alpha-smooth muscle actin (α-SMA), three known TGF-β-induced genes. A significant upregulation was observed for all three genes in both COPD and control fibroblasts (Supplementary Figure 1, p < 0.001). The total number of reads obtained of each sample and the percentages of reads mapping to miRBase Release 21 are shown in Supplementary Table 1. The ten most abundant miRNAs (Fig. 1) were expressed at similar levels in lung fibroblasts from control and COPD fibroblasts, either with or without TGF-β stimulation. The majority of the reads in all four groups were derived from miR-21-5p. Together, the top-10 most abundant miRNAs accounted for approximately 65% of all reads in unstimulated and TGF-β-stimulated lung fibroblasts (Fig. 1).

Top-10 most abundant miRNAs in lung fibroblasts of controls and COPD patients with/without TGF-β stimulation. Relative fractions of the read counts of the top-10 most abundant miRNAs in unstimulated (Left) and in TGF-β-stimulated lung fibroblasts (Right). The read counts in control and COPD lung fibroblasts were combined, as the expression levels of these ten miRNAs were similar in control and COPD fibroblasts.
Next, we identified miRNAs that were differentially expressed upon TGF-β stimulation in lung fibroblasts from controls and COPD patients. In control subjects, we identified 86 differentially expressed miRNAs (49 up- and 37 downregulated, FDR < 0.05, Fig. 2A, Supplementary Table 2). In COPD patients, 46 miRNAs were differentially expressed upon TGF-β stimulation (33 up- and 13 downregulated, FDR < 0.05, Fig. 2B, Supplementary Table 2). The overlap between the control and COPD fibroblasts was 27 for the TGF-β-induced and 9 for the TGF-β-repressed miRNAs (Fig. 2C,D). In total, 96 miRNAs were significantly differentially expressed upon TGF-β stimulation in lung fibroblasts of controls and/or COPD patients, including the most abundantly expressed miRNAs miR-21-5p, miR-26a-5p, miR-221-3p and miR-222-3p (Supplementary Table 2). The most significantly differentially expressed miRNA for both groups was miR-27a-5p with a fold change of 4.1 in control and 3.0 in COPD fibroblasts (Fig. 2E). The TGF-β-induced differential expression of miR-27a-5p was validated in the same lung fibroblasts using RT-qPCR (p-value < 0.001, Fig. 2F).

Differentially expressed miRNAs upon TGF-β stimulation in lung fibroblasts. (A,B) Volcano plot of the 349 miRNAs included in the analyses of the small RNA sequencing data. The lowest horizontal line represents the nominal p-value cut-off of 0.05. The upper horizontal line represents the FDR of 0.05. Differentially expressed miRNAs are indicated with red dots (FDR < 0.05). (C) Overlap of the upregulated miRNAs and (D) downregulated miRNAs after TGF-β stimulation in lung fibroblasts from controls and COPD patients. (E) MiR-27a-5p expression in the lung fibroblasts from controls and COPD patients with/without TGF-β stimulation based on the small RNA sequencing data. ****FDR < 0.0001. (F) Validation of miR-27a-5p expression in lung fibroblasts from 15 controls and 12 COPD patients with and without TGF-β stimulation using RT-qPCR. The data are presented as relative expression to RNU48 (2−ΔCp). ***p-value < 0.001, ****p-value < 0.0001.
MiRNAs differentially regulated by TGF-β in COPD compared to control fibroblasts
To identify miRNAs that are differentially regulated by TGF-β in COPD compared to control fibroblasts, we performed an interaction analysis on the 96 TGF-β-regulated miRNAs identified above. We found twelve miRNAs that responded differentially to TGF-β stimulation in lung fibroblasts from COPD compared to control fibroblasts at a nominal p-value < 0.05 (Table 2). For seven of them, the change in expression induced by TGF-β was detected only in control fibroblasts while there was no change in COPD fibroblasts. For two miRNAs, an increased expression was observed in COPD upon TGF-β treatment, while there was no change in control fibroblasts. Three miRNAs showed a change in the same direction, but in different degrees.
After correcting for multiple testing, three miRNAs, miR-148b-3p, miR-589-5p and miR-376b-3p, remained significant at an FDR < 0.25 (Fig. 3). MiR-148b-3p and miR-589-5p levels were significantly decreased upon TGF-β stimulation in control fibroblasts, whereas no effect was observed in COPD fibroblasts. The levels of miR-376b-3p were significantly increased upon TGF-β stimulation in control fibroblasts, while again no change was observed in COPD fibroblasts. Despite reasonable read counts for miR-148b-3p, RT-qPCR revealed very high Cp values (34–37), precluding a reliable validation (data not shown). MiR-589-5p and miR-376b-3p had low read counts and were therefore not selected for RT-qPCR validation.

TGF-β ~ COPD interaction. Lung fibroblasts of COPD patients responded differently to TGF-β stimulation compared to those of controls with respect to expression of miR-148b-3p, miR-589-5p and miR-376b-3p (p-value miR-148b-3p = 0.0026, p-value miR-589-5p = 0.0053, p-value miR-376b-3p = 0.0057; FDR of interaction analysis all <0.25), based on small RNA sequencing data. *FDR TGF-β effect in controls <0.05, ***FDR TGF-β effect in controls <0.001.
Small RNA sequencing analysis of COPD and control lung fibroblasts
Linear regression analysis of the 349 miRNAs obtained after filtering revealed one miRNA with a higher expression in lung fibroblasts from COPD patients at an FDR cut-off <0.05 (miR-660-5p, FC = 1.4, FDR p-value = 5.9 × 10−3, Fig. 4A,B). Additionally, 37 other miRNAs showed differential expression between COPD and control fibroblasts at a nominal p-value < 0.05 (Supplementary Table 3). Validation of the differential expression of miR-660-5p by RT-qPCR in lung fibroblasts was not feasible due to low expression levels (Cp values 33–37, data not shown). In the lung tissue samples used for replication, miR-660-5p expression levels were within the range of detection (Cp values 30–32), however, no differences were observed between lung tissue from COPD patients and from controls (Fig. 4C).

MiR-660-5p in lung fibroblasts and lung tissue from COPD patients. (A) Volcano plot of the 349 miRNAs included in the analyses of the small RNA sequencing data. The lowest horizontal line represents the nominal p-value cut-off of 0.05. The upper horizontal line represents the FDR of 0.05. MiR-660-5p, indicated with a red dot, was higher expressed in lung fibroblasts from COPD compared to controls (FC = 1.4, FDR = 5.9 × 10−3). (B) MiR-660-5p expression in the lung fibroblasts from controls and COPD patients based on the small RNA sequencing data. **FDR = 5.9 × 10−3. (C) MiR-660-5p expression in lung tissue from controls and COPD patients using RT-qPCR. The data are presented as relative expression to RNU48 (2−ΔCp).
Predicted targets of miR-27a-5p, miR-148b-3p and miR-660-5p
For the identification of target genes of miR-27a-5p, miR-148b-3p and miR-660-5p relevant in lung fibroblasts we re-analysed our previously published miRNA-targetome dataset (generated with Ago2-IP) of primary lung fibroblasts from two control subjects16. For miR-27a-5p a significant enrichment of miRNA target genes in the top-1,500 of most IP-enriched genes compared to all expressed genes was observed in one of the two controls (Fig. 5A). For miR-148b-3p, we observed a significant enrichment of predicted targets in both controls (p-value < 0.0001, Fig. 5B). For miR-660-5p, a significant (p-value < 0.05) and a borderline significant (p = 0.0554) enrichment of predicted target genes was observed (Fig. 5C).

Ago2-IP-enrichment of predicted targets of miR-27a-5p, miR-148b-3p and miR-660-5p. The percentages of predicted targets of (A) miR-27a-5p, (B) miR-148b-3p and (C) miR-660-5p were calculated in all expressed genes and in the top-1,500 most IP-enriched probes in lung fibroblasts of two control subjects (Control 1 and 2). For miR-27a-5p, miR-148b-3p and miR-660-5p, 922, 677 and 421 predicted targets, respectively, were included in the analyses. Chi-square test was used to determine whether the number of predicted targets in the top-1,500 most Ago2-IP-enriched probes was significantly different from the expected based on the number of predicted targets in all expressed genes. All the other numbers in the bars are the number of predicted targets of each miRNA. *p-value < 0.05, ****p-value < 0.0001. The top-10 most IP-enriched predicted target genes are shown in the table. The numbers in the table indicate the rankings of the predicted target genes based on the IP-enrichment, i.e. 1 = most IP-enriched predicted target gene, 2 = second most IP-enriched target gene.
The top-10 most IP-enriched predicted target genes for each of these three miRNAs are shown in Fig. 5, including the ranking in the IP-enrichment for each control. Phosphatidylcholine Transfer Protein (PCTP) was the most IP-enriched predicted target gene of the TGF-β-induced miR-27a-5p. Of the most enriched predicted target genes of miR-27a-5p, Nuclear Receptor Subfamily 6 Group A Member 1 (NR6A1) and PR/SET Domain 1 (PRDM1) are both involved in negative regulation of transcription, and NHL Repeat Containing 3 (NHLRC3) and Trafficking Protein Particle Complex 1 (TRAPPC1) are engaged in neutrophil mediated immunity (Supplementary Table 4). High Mobility Group AT-Hook 2 (HMGA2) was the most IP-enriched predicted target of miR-148b-3p. Of the top-10 most enriched predicted miR-148b-3p target genes, seven genes play a role in the regulation of gene transcription. For miR-660-5p, Solute Carrier Family 46 Member 3 (SLC46A3) and Zinc Finger Protein 273 (ZNF273) were the most enriched predicted target genes. Five of the top-10 most IP-enriched predicted miR-660-5p target genes were involved in regulation of gene transcription.
Discussion
Using small RNA sequencing, we identified 96 TGF-β-regulated miRNAs in lung fibroblasts from controls and/or COPD patients, from which miR-27a-5p was the most strongly TGF-β-induced miRNA. In addition, we identified miR-148b-3p, miR-589-5p and miR-376b-3p as differentially regulated by TGF-β in COPD compared to control fibroblasts. Of these miRNAs, only miR-148b-3p was highly expressed based on our small RNA sequencing data. Furthermore, we demonstrated higher expression of miR-660-5p in COPD compared to control fibroblasts. Using our previously published miRNA-targetome dataset, we identified multiple IP-enriched and predicted targets of miR-27a-5p, miR-148b-3p and miR-660-5p, representing possible targets through which these miRNAs may affect lung fibroblast function in COPD.
TGF-β stimulation had a strong effect on the miRNA expression profile in lung fibroblasts from COPD patients and controls. Interestingly, we found much less TGF-β-regulated miRNAs in COPD fibroblasts compared to controls. A previous study reported that the TGF-β release by COPD fibroblasts was elevated, whereas their repair responses were reduced compared to control fibroblasts5. This may suggest that COPD lung fibroblasts are also less responsive to TGF-β stimulation in our study. Of the TGF-β-regulated miRNAs, miR-27a-5p was the most prominent in lung fibroblasts from both COPD patients and controls. These findings were consistent with our previous study investigating TGF-β effects on control lung fibroblasts16. Interestingly, the interaction analysis suggested that the induction of miR-27a-5p upon TGF-β stimulation was lower in COPD compared to control fibroblasts, supporting the notion that COPD fibroblasts are less responsive to TGF-β than control fibroblasts. The most IP-enriched predicted target gene of miR-27a-5p was PCTP. This gene encodes a protein that regulates intermembrane transfer of phosphatidylcholine, which is one of the most abundant phospholipids in plasma membranes17. Our enrichment and pathway analysis suggest that miR-27a-5p is involved in negative regulation of transcription by targeting NR6A1 and PRDM1. NR6A1 can repress gene expression by binding to DNA and recruiting DNA methyltransferases18. PRDM1 is a transcription factor that can repress β-interferon expression19. In addition, PRDM1 downregulates p53 transcription by binding to its promoter, while p53 positively regulates transcription of PRDM120. Knockdown of PRDM1 in human fibroblasts resulted in growth arrest20. Together this indicates that TGF-β-induced miR-27a-5p expression in lung fibroblasts may represent a mechanism to control TGF-β-induced cell proliferation via targeting PRDM1. Pathway analyses suggested that miR-27a-5p may also be involved in neutrophil mediated immunity by targeting NHLRC3 and TRAPPC1. However, expression of these genes is not restricted to neutrophils; our previously published Ago2-IP dataset demonstrated high expression levels of these genes in primary lung fibroblasts16. A recent study showed that miR-27a-5p affected NF-κB signalling in human aortic endothelial cells21, but none of those NF-κB signalling genes were enriched in the miRNA-targetome of our lung fibroblasts.
In the interaction analyses, we found only miR-148b-3p with high read counts that responded differently at an FDR cut-off of 0.25 to TGF-β in lung fibroblasts from COPD patients compared to controls. MiR-148b-3p expression was lower upon TGF-β treatment in the controls and did not change in COPD patients. It is tempting to speculate that processes are activated in lung fibroblasts from controls in the presence of TGF-β, which may contribute to tissue repair and remodelling. This response may be attenuated in lung fibroblasts from COPD patients. In bronchial smooth muscle cells from asthma patients, miR-148b-3p was upregulated22. HMGA2 was the most IP-enriched target gene of miR-148b-3p and was shown to be required for TGF-β-induced transcription of several genes, including GATA623. It was suggested that GATA6 may mediate the TGF-β-induced upregulation of alpha-smooth muscle actin (α-SMA) in fibroblasts from idiopathic pulmonary fibrosis with histopathology of usual interstitial pneumonia24. As miR-148b-3p was downregulated upon TGF-β-stimulation in lung fibroblasts from controls, it is plausible that miR-148b-3p may indirectly contribute to the TGF-β-induced upregulation of α-SMA. HMGA2 can also induce apoptosis and growth arrest in in human lung fibroblasts25, which may be due to the decreased miR-148b-3p expression after TGF-β treatment.
Of the other miRNAs identified in the interaction analysis, miR-99b-5p, miR-181a-2-3p, and miR-136-3p, have already been linked to COPD previously26,27,28. In addition, miR-25-3p and miR-181a-2-3p were found to be downregulated in COPD lung fibroblasts compared to controls in our current study (p-value < 0.05). For miR-21-3p, we previously showed regulation by TGF-β in control and COPD lung fibroblasts consistent with our current findings16.
We found a significantly higher expression of miR-660-5p in lung fibroblasts from COPD patients compared to controls. MiR-660-5p did not pop up in the previous miRNA profiling study of Ikari et al.14. Previously, circulating miR-660-5p levels were shown to be positively associated with FEV1/FVC of asthmatic children29. This positive association of miR-660-5p with lung function was not found in lung fibroblasts of severe COPD patients included in our study. A possible explanation for this might be that this miRNA has cell type and/or organ specific functions. Pathway analysis demonstrated that five predicted miR-660-5p targets, including the top gene ZNF273, are involved in regulating gene transcription. ZNF273 is a C2H2 zinc-finger motifs and Krüppel-associated box (KRAB)-domain-containing protein. Members of the KRAB-containing protein family are involved in transcriptional repression of RNA polymerase promoters, binding and splicing of RNA, and control of nucleolus function30. In addition, another target, SLC46A3 has been shown to be upregulated in bronchial epithelial cells of COPD compared to controls31. This is different from our findings of higher miR-660-5p levels in COPD lung fibroblasts, which would rather be associated with lower SLC46A3 expression in COPD. Again, this might be due to different involvement in cell type specific functions. Previously, miR-660-5p was shown to directly target MDM232, which was among the IP-enriched target gene in one of our controls16. MDM2 is involved in degradation of p53 protein33 and downregulation of p53 in control lung fibroblasts increased the proliferation rate and the migration and invasion capacity33. A miR-660-5p-regulated decrease in MDM2 expression in lung fibroblasts may thus modulate fibroblast proliferation and motility via p53. Interestingly, because in line with the increased miR-660-5p in COPD, it was reported that p53 protein levels were elevated in emphysematous lung tissue34,35.
Whereas small RNA sequencing revealed differential regulation upon TGF-β stimulation for miR-148b-3p in COPD fibroblasts and differential expression of miR-660-5p, both miRNAs could not be validated using RT-qPCR in the same samples, since the expression levels were too low to be quantified reliably. Especially for miR-148b-3p which had high read counts in the small RNA sequencing data and very strong enrichment of predicted target genes, this was a surprise. It may be explained by lack of specificity of the assays. Although overall read counts of miR-660-5p were relatively low, differences in small RNA sequencing data were clear and significant enrichment of predicted target genes in lung fibroblast does suggest that this miRNA is active in these cells. Further investigation, including biological validation, is needed to confirm our results.
In conclusion, we showed that TGF-β affects expression of a considerable number of miRNAs in primary lung fibroblasts. Three of these TGF-β-regulated miRNAs responded differently to TGF-β in COPD compared to control fibroblasts. In contrast, only one miRNA was differentially expressed in COPD fibroblasts. Altered miRNA regulation, i.e. differential response to TGF-β stimulation in COPD compared to control fibroblasts and differentially expressed miR-660-5p in COPD, may be one of the mechanisms underlying aberrant tissue repair and remodelling in COPD.
Materials and Methods
Subjects
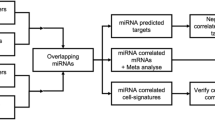
The workflow of this study is shown in Fig. 6. Primary fibroblasts were obtained from 15 stage IV COPD patients undergoing lung transplant surgery and 15 non-COPD controls with normal lung function undergoing lung tumour resection surgery. For the latter group lung fibroblasts were isolated from left-over parenchymal lung tissue located far away from the tumour without histological abnormalities36,37. Lung tissue from 18 stage IV COPD patients and 17 non-COPD controls was used to replicate the results.

Workflow FDR = false discovery rate, DE = differentially expressed, Ago2-IP = argonaute 2-immunoprecipitation.
This study was performed in accordance with the national ethical and professional guidelines on the use human body material (“Code of conduct; Dutch federation of biomedical scientific societies”; https://www.federa.org/codes-conduct) and the Research Code of the University Medical Centre Groningen (https://www.umcg.nl/SiteCollectionDocuments/English/Researchcode/umcg-research-code-2018-en.pdf). The left-over lung material, which was used to isolate lung fibroblasts or to replicate the results, was at the time of the experiments not subject to the act on medical research involving human subjects in the Netherlands. Therefore, an ethics waiver was provided by the Medical Ethical Committee of the University Medical Centre Groningen (METc UMCG). All samples and clinical information were de-identified before experiments were performed.
Cell culture, TGF-β stimulation and RNA isolation
Primary fibroblasts were isolated from lung parenchyma using the explant technique as described previously38. The fibroblasts were cultured in complete medium consisting of Ham’s F12 medium, 10% (v/v) fetal calf serum (FCS), 100 U/ml penicillin/streptomycin and 200 mM L-glutamine (all from Lonza, Breda, The Netherlands). The experiments were performed on fibroblasts at passage 5. Lung fibroblasts were stimulated with 7.5 ng/ml TGF-β1 (R&D Systems, Abingdon, UK) in complete Ham’s F12 medium containing 0.5% (v/v) FCS for 24 h. Total RNA was isolated from primary parenchymal lung fibroblasts and lung tissues using TRIzol (Invitrogen, Carlsbad, CA, USA), according to the protocol of the manufacturer. The RNA concentration was measured with a NanoDrop 1000 Spectrophotometer (Thermo Scientific, Wilmington, DE, USA).
cDNA synthesis and qPCR for ECM genes and α-SMA
To confirm effective TGF-β stimulation, expression levels of several known TGF-β-regulated genes FN1, COL1A1 and α-SMA in lung fibroblasts39,40 were determined by RT-qPCR, as described previously16. 18S rRNA (18S) and RNA polymerase II (RP2) were used as reference genes. Positive and negative controls were included in each run. The formula 2−ΔCp was used to calculate the relative mRNA expression levels.
Small RNA sequencing
Libraries were generated with the NEXTflex Small RNA-seq kit V3 (Bioo Scientific, Uden, The Netherlands) using total RNA (approximately 1 μg) of the lung fibroblasts with/without TGF-β stimulation and sequenced on the NextSeq 500 (Illumina, San Diego, CA, USA) according to the protocol of the manufacturer. TrimGAlore 0.3.7 was used to trim the adapter sequences of the raw reads. Subsequently, the reads were allocated to the human miRNAs (miRBase Release 21, http://www.mirbase.org/) allowing one mismatch using the miRDeep2 V2.0.0.8 software41. The reads of miRNAs with the same mature sequence were summed up. Only miRNAs with ≥10 reads per million in more than half of the samples in at least one group (lung fibroblasts of COPD patients or controls, with or without TGF-β stimulation) were included. After applying these filtering steps, 349 miRNAs were left for further analyses.
cDNA syntheses and qPCR for miRNAs
To validate and replicate the small RNA sequencing results, RT-qPCR was performed as described previously16,42. Briefly, cDNA was synthesized using 10 ng total RNA of the parenchymal fibroblasts and/or lung tissues and reverse transcription primers from TaqMan® microRNA Assay kits, small nucleolar RNA, C/D box 48 (RNU48) (Assay ID: 001006), hsa-miR-27a* (Assay ID: 002445), hsa-miR-148b (Assay ID: 000471) and efu-miR-660 (Assay ID: 475114_mat) (Applied Biosystems, Carlsbad, CA, USA). Assays were selected based on the most abundant miRNA sequence identified in the small RNA sequencing data. Next, qPCR was performed in LightCycler 480 Probes Master reaction mix (Roche Diagnostics GmbH, Mannheim, Germany) and the above mentioned TaqMan microRNA assays. RNU48 was used as reference gene, and positive and negative controls were included in each run. The relative miRNA expression levels were calculated using the formula 2−ΔCp.
Ago2-IP and gene ontology/pathway analyses
Data of our previously published argonaute-2-immunoprecipitation (Ago2-IP) experiments in primary lung fibroblasts from two control subjects were used to identify genes targeted by miRNAs selected in this study, as described previously16. Control 1 had in total 19,874 expressed genes of which the top-1,500 IP-enriched probes consisted of 1,298 unique genes16. Control 2 had in total 17,779 expressed genes of which the top-1,500 IP-enriched probes encounter for 1,306 unique genes16. For poorly conserved miRNAs, predicted targets with a cumulative weighted context++ score ≤0.2 were included in the analyses (TargetScan version 7.243). For broadly conserved miRNAs, predicted targets with conserved binding sites were considered. To assess the potential functional relevance of individual miRNAs, we identified the top-10 most IP-enriched and TargetScan predicted genes. For each miRNA, the top-10 most enriched predicted target genes were subjected to Enrichr44,45 to identify the biological processes (gene-set library: GO_Biological_Process_2018) and Reactome pathways (gene-set library: Reactome_2016). We focused on pathways for which at least two of the top-10 enriched genes are involved in, without taking the significance of the process/pathway enrichment into account.
Statistical analyses
The Mann Whitney U test was used to compare differences in subject characteristics between COPD patients and control subjects, and between the fibroblast and lung tissue donors (IBM SPSS Statistics version 22). Small RNA sequencing data were analysed in R (v3.5.2)46 with the Bioconductor-Limma package (v3.38.3)47.
Three separate analyses were conducted; (1) a linear regression model (TGF-β - baseline) was performed to investigate the effect of TGF-β overall on miRNA expression in controls and COPD fibroblasts, separately, (2) interaction analysis ((COPD TGF-β - COPD baseline) - (control TGF-β - control baseline)) was conducted to investigate whether miRNAs are differentially regulated by TGF-β in COPD compared to control fibroblasts, and (3) a linear regression model (COPD baseline - control baseline) was run to look at the differences of miRNA expression between COPD and control fibroblasts at baseline. For the interaction analyses, we focused on miRNAs that were differentially expressed upon TGF-β stimulation in fibroblasts from COPD patients and/or controls. These models were adjusted for age, gender, smoking status and library preparation batch. Results were corrected for multiple testing using the Benjamini-Hochberg false discovery rate (FDR).
The TGF-β effect on miRNA expression levels determined by RT-qPCR was analysed using the one-sided paired Wilcoxon signed rank test. Enrichment of predicted target genes in the Ago2-IP was assessed by a chi-square test on the percentage of predicted targets in the top-1,500 enriched probes compared to the percentage of predicted targets in all expressed genes. A p-value below 0.05 was considered statistically significant.
Data availability
The small RNA sequencing dataset generated for this manuscript is available for collaboration upon request.
References
WHO. The top 10 causes of death., http://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of-death (2018).
WHO. Chronic obstructive pulmonary disease (COPD), http://www.who.int/en/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (2017).
Mocchegiani, E., Giacconi, R. & Costarelli, L. Metalloproteases/anti-metalloproteases imbalance in chronic obstructive pulmonary disease: genetic factors and treatment implications. Current opinion in pulmonary medicine 17(Suppl 1), S11–19, https://doi.org/10.1097/01.mcp.0000410743.98087.12 (2011).
Hogg, J. C. & Timens, W. The pathology of chronic obstructive pulmonary disease. Annual review of pathology 4, 435–459, https://doi.org/10.1146/annurev.pathol.4.110807.092145 (2009).
Togo, S. et al. Lung fibroblast repair functions in patients with chronic obstructive pulmonary disease are altered by multiple mechanisms. American journal of respiratory and critical care medicine 178, 248–260, https://doi.org/10.1164/rccm.200706-929OC (2008).
Takizawa, H. et al. Increased expression of transforming growth factor-beta1 in small airway epithelium from tobacco smokers and patients with chronic obstructive pulmonary disease (COPD). American journal of respiratory and critical care medicine 163, 1476–1483, https://doi.org/10.1164/ajrccm.163.6.9908135 (2001).
Mak, J. C. et al. Elevated plasma TGF-beta1 levels in patients with chronic obstructive pulmonary disease. Respiratory medicine 103, 1083–1089, https://doi.org/10.1016/j.rmed.2009.01.005 (2009).
Konigshoff, M., Kneidinger, N. & Eickelberg, O. TGF-beta signaling in COPD: deciphering genetic and cellular susceptibilities for future therapeutic regimen. Swiss medical weekly 139, 554–563, smw-12528 (2009).
Zandvoort, A. et al. Smad gene expression in pulmonary fibroblasts: indications for defective ECM repair in COPD. Respiratory research 9, 83, https://doi.org/10.1186/1465-9921-9-83 (2008).
Friedman, R. C., Farh, K. K., Burge, C. B. & Bartel, D. P. Most mammalian mRNAs are conserved targets of microRNAs. Genome research 19, 92–105, https://doi.org/10.1101/gr.082701.108 (2009).
Ardekani, A. M. & Naeini, M. M. The Role of MicroRNAs in Human. Diseases. Avicenna journal of medical biotechnology 2, 161–179 (2010).
Osei, E. T. et al. Unravelling the complexity of COPD by microRNAs: it’s a small world after all. The European respiratory journal 46, 807–818, https://doi.org/10.1183/13993003.02139-2014 (2015).
De Smet, E. G., Mestdagh, P., Vandesompele, J., Brusselle, G. G. & Bracke, K. R. Non-coding RNAs in the pathogenesis of COPD. Thorax 70, 782–791, https://doi.org/10.1136/thoraxjnl-2014-206560 (2015).
Ikari, J. et al. Effect of culture conditions on microRNA expression in primary adult control and COPD lung fibroblasts in vitro. In vitro cellular & developmental biology. Animal 51, 390–399, https://doi.org/10.1007/s11626-014-9820-8 (2015).
Ikari, J. et al. Reduced microRNA-503 expression augments lung fibroblast VEGF production in chronic obstructive pulmonary disease. PloS one 12, e0184039, https://doi.org/10.1371/journal.pone.0184039 (2017).
Ong, J. et al. Identification of transforming growth factor-beta-regulated microRNAs and the microRNA-targetomes in primary lung fibroblasts. PloS one 12, e0183815, https://doi.org/10.1371/journal.pone.0183815 (2017).
Mao, G. et al. Transcription Factor RUNX1 Regulates Platelet PCTP (Phosphatidylcholine Transfer Protein): Implications for Cardiovascular Events: Differential Effects of RUNX1 Variants. Circulation 136, 927–939, https://doi.org/10.1161/CIRCULATIONAHA.116.023711 (2017).
Wang, H., Wang, X., Xu, X., Kyba, M. & Cooney, A. J. Germ Cell Nuclear Factor (GCNF) Represses Oct4 Expression and Globally Modulates Gene Expression in Human Embryonic Stem (hES) Cells. The Journal of biological chemistry 291, 8644–8652, https://doi.org/10.1074/jbc.M115.694208 (2016).
Keller, A. D. & Maniatis, T. Identification and characterization of a novel repressor of beta-interferon gene expression. Genes & development 5, 868–879 (1991).
Yan, J. et al. BLIMP1 regulates cell growth through repression of p53 transcription. Proceedings of the National Academy of Sciences of the United States of America 104, 1841–1846, https://doi.org/10.1073/pnas.0605562104 (2007).
Romay, M. C. et al. Regulation of NF-kappaB signaling by oxidized glycerophospholipid and IL-1beta induced miRs-21-3p and -27a-5p in human aortic endothelial cells. Journal of lipid research 56, 38–50, https://doi.org/10.1194/jlr.M052670 (2015).
Alexandrova, E. et al. Small RNA profiling reveals deregulated phosphatase and tensin homolog (PTEN)/phosphoinositide 3-kinase (PI3K)/Akt pathway in bronchial smooth muscle cells from asthmatic patients. The Journal of allergy and clinical immunology 137, 58–67, https://doi.org/10.1016/j.jaci.2015.05.031 (2016).
Singh, I. et al. High mobility group protein-mediated transcription requires DNA damage marker gamma-H2AX. Cell research 25, 837–850, https://doi.org/10.1038/cr.2015.67 (2015).
Lepparanta, O. et al. Transcription factor GATA-6 is expressed in quiescent myofibroblasts in idiopathic pulmonary fibrosis. American journal of respiratory cell and molecular biology 42, 626–632, https://doi.org/10.1165/rcmb.2009-0021OC (2010).
Shi, X. et al. A novel anti-proliferative role of HMGA2 in induction of apoptosis through caspase 2 in primary human fibroblast cells. Bioscience reports 35, https://doi.org/10.1042/BSR20140112 (2015).
Conickx, G. et al. MicroRNA Profiling Reveals a Role for MicroRNA-218-5p in the Pathogenesis of Chronic Obstructive Pulmonary Disease. American journal of respiratory and critical care medicine 195, 43–56, https://doi.org/10.1164/rccm.201506-1182OC (2017).
Kim, J. et al. Role of miRNA-181a-2-3p in cadmium-induced inflammatory responses of human bronchial epithelial cells. Journal of thoracic disease 11, 3055–3069, https://doi.org/10.21037/jtd.2019.07.55 (2019).
Qian, Y. et al. Comprehensive Analysis of miRNA-mRNA-lncRNA Networks in Non-Smoking and Smoking Patients with Chronic Obstructive Pulmonary Disease. Cellular physiology and biochemistry: international journal of experimental cellular physiology, biochemistry, and pharmacology 50, 1140–1153, https://doi.org/10.1159/000494541 (2018).
Kho, A. T. et al. Circulating MicroRNAs: Association with Lung Function in Asthma. PloS one 11, e0157998, https://doi.org/10.1371/journal.pone.0157998 (2016).
Urrutia, R. KRAB-containing zinc-finger repressor proteins. Genome biology 4, 231, https://doi.org/10.1186/gb-2003-4-10-231 (2003).
Chang, W. A., Tsai, M. J., Jian, S. F., Sheu, C. C. & Kuo, P. L. Systematic analysis of transcriptomic profiles of COPD airway epithelium using next-generation sequencing and bioinformatics. International journal of chronic obstructive pulmonary disease 13, 2387–2398, https://doi.org/10.2147/COPD.S173206 (2018).
Fortunato, O. et al. Mir-660 is downregulated in lung cancer patients and its replacement inhibits lung tumorigenesis by targeting MDM2-p53 interaction. Cell death & disease 5, e1564, https://doi.org/10.1038/cddis.2014.507 (2014).
Nagaraja, M. R. et al. p53 Expression in Lung Fibroblasts Is Linked to Mitigation of Fibrotic Lung Remodeling. The American journal of pathology 188, 2207–2222, https://doi.org/10.1016/j.ajpath.2018.07.005 (2018).
Morissette, M. C., Vachon-Beaudoin, G., Parent, J., Chakir, J. & Milot, J. Increased p53 level, Bax/Bcl-x(L) ratio, and TRAIL receptor expression in human emphysema. American journal of respiratory and critical care medicine 178, 240–247, https://doi.org/10.1164/rccm.200710-1486OC (2008).
Mizuno, S. et al. p53 Signaling Pathway Polymorphisms Associated With Emphysematous Changes in Patients With COPD. Chest 152, 58–69, https://doi.org/10.1016/j.chest.2017.03.012 (2017).
Noordhoek, J. A. et al. Different proliferative capacity of lung fibroblasts obtained from control subjects and patients with emphysema. Experimental lung research 29, 291–302 (2003).
Noordhoek, J. A. et al. Different modulation of decorin production by lung fibroblasts from patients with mild and severe emphysema. Copd 2, 17–25 (2005).
Brandsma, C. A. et al. Differential effects of fluticasone on extracellular matrix production by airway and parenchymal fibroblasts in severe COPD. American journal of physiology. Lung cellular and molecular physiology 305, L582–589, https://doi.org/10.1152/ajplung.00152.2013 (2013).
Brandsma, C. A. et al. A large lung gene expression study identifying fibulin-5 as a novel player in tissue repair in COPD. Thorax 70, 21–32, https://doi.org/10.1136/thoraxjnl-2014-205091 (2015).
Renzoni, E. A. et al. Gene expression profiling reveals novel TGFbeta targets in adult lung fibroblasts. Respiratory research 5, 24, https://doi.org/10.1186/1465-9921-5-24 (2004).
Friedlander, M. R., Mackowiak, S. D., Li, N., Chen, W. & Rajewsky, N. miRDeep2 accurately identifies known and hundreds of novel microRNA genes in seven animal clades. Nucleic acids research 40, 37–52, https://doi.org/10.1093/nar/gkr688 (2012).
Kluiver, J., Slezak-Prochazka, I. & van den Berg, A. Studying microRNAs in lymphoma. Methods in molecular biology 971, 265–276, https://doi.org/10.1007/978-1-62703-269-8_15 (2013).
Agarwal, V., Bell, G. W., Nam, J. W. & Bartel, D. P. Predicting effective microRNA target sites in mammalian mRNAs. eLife 4, https://doi.org/10.7554/eLife.05005 (2015).
Chen, E. Y. et al. Enrichr: interactive and collaborative HTML5 gene list enrichment analysis tool. BMC bioinformatics 14, 128, https://doi.org/10.1186/1471-2105-14-128 (2013).
Kuleshov, M. V. et al. Enrichr: a comprehensive gene set enrichment analysis web server 2016 update. Nucleic acids research 44, W90–97, https://doi.org/10.1093/nar/gkw377 (2016).
R: A language and environment for statistical computing. R Foundation for Statistical Computing. Vienna, Austria. Available at: https://www.R-project.org/ (2016).
Ritchie, M. E. et al. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic acids research 43, e47, https://doi.org/10.1093/nar/gkv007 (2015).
Acknowledgements
We thank the UMCG Genomics Coordination centre, the UG Centre for Information Technology and their sponsors BBMRI-NL & TarGet for storage and compute infrastructure. In addition, we would like to thank Wierd Kooistra for performing RT-qPCR. This work was supported by the Lung Foundation Netherlands (Longfonds), grant number: 3.2.12.044.
Author information
Authors and Affiliations
Contributions
W.T., M.v.d.B., A.v.d.B., J.K., and C.A.B. designed the research and drafted the analysis plan. J.O. performed the experiments, analysed the data and prepared the figures and tables. K.K. and M.M.T. pre-processed the small RNA sequencing dataset. A.F. analysed the small RNA sequencing data. J.O. and C.A.B. drafted the manuscript. All authors reviewed, edited and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ong, J., Faiz, A., Timens, W. et al. Marked TGF-β-regulated miRNA expression changes in both COPD and control lung fibroblasts. Sci Rep 9, 18214 (2019). https://doi.org/10.1038/s41598-019-54728-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-54728-4
This article is cited by
-
Different expression of circulating microRNA profile and plasma SP-D in Tibetan COPD patients
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
