
Abstract
The increasing ratio of diabetes is found risky across the planet. Therefore, the diagnosis is important in population with extreme risk of diabetes. In this study, a decision-making classifier (J48) is applied over a data-mining platform (Weka) to measure accuracy and linear regression on classification results to forecast cost/benefit ratio in diabetes mellitus patients along with prevalence. In total 108 invasive and non-invasive medical features are considered from 251 patients for assessment, and the real-time data are gathered from Pakistan over a time span of June 2017 to April 2018. The results indicate that J48 classifiers achieved the best accuracy of (99.28%), whereas, error rate (0.08%), Kappa stats, PRC, and MCC are (0.98%), precision, recall, and F-matrix are (0.99%). In addition, true positive rate is (0.99%) and false positive is (0.08%). The regression forecast decision indicates blood pressure and glucose level are key features for diabetes. The cost/benefit matrix indicates two predictions for positive test with accuracy (66.68%) and (30.60%), and key attributes with total Gain (118.13%). The study confirmed the proposed prediction is practical for screening of diabetes mellitus patients at the initial stage without invasive medical tests and found effectual in the early diagnosis of diabetes.
Similar content being viewed by others


Introduction
The data mining is a modern technique of digging into data to locate patterns ideally. It is an astounded spectator of incredible progress in modern health care1. The undiscovered electronic health records (EHRs) are being used to manipulate the unknown patterns located in the health datasets and healthcare industries, which are enthusiastically supporting the copious amount of data. This data can be manipulate for prognostication and scrutinizing of diabetes mellitus ratio in epidemiological states around the globe2. The data mining techniques contain the association rule mining for finding the outlines of modern classifications and cluster. From the last several years, data processing methods are being utilized in various domains by choosing data from different machine learning repositories but it came extremely late in diabetes section3. The data mining platform is supported by divine mysteries including machine learning 60%4, statistics 30%5, artificial intelligence 5%6 and probabilities 5%7. Study indicates that the data mining techniques have been used to diagnose diabetes mellitus in developing countries, i.e. Ashrafuzaman et al. mentioned that diabetes is properly considered as most rapidly spreading and inaudibly life-taking disease that causes the most valued snags in the modern world of health8. According to the initial predictions, diabetes preserves serious health complications as mentioned in the book “Heavens on Earth”9. However, the accurate predictions of diabetes remain a perplexing task for the medical whizzes due to its clandestine patterns.
According to (NIH), the number of patients suffering from diabetes is increasing exponentially that leads with some causes but the most significant factors include age, diet plans, glucose levels, sugar intakes, thirst, urination, vision symptoms, skin issues, and others with body mass indexes10,11. The mostly discussed level of diabetes mellitus found are Type-2 however, Type-1 diabetes and Gestational are at its peak in the developing countries, which are affecting the other severe health complications i.e. kidney, heart attack, strokes, and cancer. In addition, 20% of patients are treated with insulin injections to control their glucose and blood pressure levels12. However, if it is neglected, it can cause slowly spreading germs to the profound effect the optimal health. Williams wrote in his book ‘Williams textbook of Endocrinology’13 that around 385 million people were affected with diabetes in 2013 and this ratio can get higher if it remains untreated and can indeed cause to death. Around 425 million people are suffering from diabetes around the globe mentioned by the survey report of the International Diabetes Federation (IDF) in 201514. The report also indicates that almost 382 million people are affected by diabetes only in developing countries out of which 4.9% are from Asia. According to World Health Organization (WHO)15, 3.31 million deaths occurred in Asia region due to diabetes; out of which 79% population is under age of 55 that is the maximum number in any region of the world. The ratio of diabetes mellitus patients in rural and urban areas of Pakistan varies from 0.56% to 12% and it has been estimated more than double of this ratio over the past two decades16.
Numerous authors worked on different techniques for the classification of diabetes mellitus like Raj Bala et al. worked for missing values and unclear facts and analyzed the figurative rule mining worktable for spawning initial rule sets and control the projects to discover the rule sets17. Rojas et al. investigate on the theory of linear genetic classification18. Saini et al. worked on Unsupervised filtering by SVM principle19. In addition, he introduced a structure centered by heterogeneous and grid distribution. Noman et al. talked about the semi supervised clustering approach by utilizing K-means and SOM algorithms20. Andrew et al. worked with outlier prediction method to accurately diagnose cardiovascular diseases21. By report of Sohail et al.22 Xue applied a Bayesian algorithm for spotting of confusion Coronary Cardiopathy. In addition, Xing predicted the survival of CHID patients by biomedical images. Moreover, he mentioned that Shusaku et al. worked by Term-Mapping for data processing of multi-scale harmonizing23. Muhammad et al. deliberated the qualities of choosing Persecution with K-means to categorize the diabetes datasets and presented an approach for clinical screening24. Various other data mining techniques were determined by authors in classification and prediction of diabetes mellitus, which are presented in “Table 1” with their accuracy ratios.
The objective of this study is to develop an accurate prediction assessment model by utilizing intrusive and non-intrusive medical features to identify a high risk of diabetes in the patients. For this purpose, the machine learning classifier J48 decision tree is used on the data-mining platform Weka version 3.9.2 to acquire accuracy in classification assumptions. Subsequently, Linear Regression LR is utilized on classification results to predict and forecast the patients with a high risk of diabetes. The proposed method can be applied to diabetes mellitus patients specifically in the remote areas or villages with low socioeconomic status and extreme epidemiological risk.
Results
In total, 281 diabetes mellitus patients were evaluated out of 563 for the assessment, including 160 (56.93%) female members and 121 (43.06%) male members. Among 281 records, 11(3.91%) were T2DM (insulin dependent), 256(91.10%) were T1DM (non-insulin dependent), and 14(4.98%) were Gestational. Initially, the real-life dataset was divided into the ratio of 20:80 percent to conduct training and testing. After training the machine, 10-fold cross-validation technique was implemented on an experimental platform of Weka (3.9.2) for classification. The dataset was further divided into 10 samples. Each sample was utilized as validation data from the retention process, while the remaining nine samples served as training data and the process was performed 10 times. This process provided a significant reduction in the error ratio and bias correlation by random sampling.
Measurements
Initially, the K-means clustering algorithm was used for the assessment of positive and negative clusters. K-means provides the specific set of accurate observations, where each observation represents d-dimensional vectors to partition the “n” observations into (k ≤ n) sets by (1). “Figure 1” presents the classified instance ratio of tested positive and negative clusters with the separation between them. By the assessment of 281 instances, 143 (51%) patients classified as tested positive for diabetes and 138 (49%) classified as tested negative that means the negative instances have fewer symptoms of diabetes and positive has strong.

Show the K-means clustering assessment of positive and negative clusters separated by the separation line.
In addition, J48 machine learning classification algorithm was utilized on 281 diabetes patients by 10 fold cross-validation technique with parameters as 100 for batch size, 0.25% for the confidence interval, minimum object numbers and decimal number places of 2, 3 numbers of folds with error pruning rate of false, and 1 number of seeds value. After the loop test, the final accuracy reached 99.28% by (2) and the error rate was 0.08%. Weka constructed a J48 evaluation of 0.08 second, a kappa stat result of 0.98%, an average true positive rate of 0.99%, an average false positive rate of 0.08%, an average accuracy, a recall rate, an F matrix, and a ROC area ratio of 0.99%, and The average PRC area ratio, MCC value is 0.98%, as shown in “Fig. 2”.

Show the classification assessment of machine learning J48 classifier with the confusion matrix of tested positive and tested negative instances.
Conclusively, “Table 2” divides the final assessment into two parts. Initially, it describes the clustering results achieved by K-means; furthermore, it shows the J48 pruning tree assessment for patients screening. The decision tree indicates that glucose and blood pressure are key features of diabetes screening after the Age attribute. The filtering rules implemented by J48 pruning tree are:
-
(1)
If the patient’s glucose level is accurate (>101), diabetes will be predicted to be positive, and in our data set, 191 patients were tested positive because their glucose levels exceeded 101.
-
(2)
If the glucose level is accurate (≤101) than 4 cases apply:
-
i.
Check blood pressure, if accurate (≤100), the test patient is negative, in our data set, 85 patients were negative in this particular case.
-
ii.
If blood pressure is usually (>100), the glucose level helps predict, as follows.
-
iii.
If glucose is (≤72), the test is accurately predicted to be negative for diabetes, which is 2 in our data set.
-
iv.
If glucose is (>72) than the specific prediction for the diabetes test is carefully taken as positive, which comes as 3 patients in our data set.
Furthermore, the results obtained by the classification are used to predict future predictions by linear regression. “Figure 3” shows the future predictions for glucose and blood pressure properties as follows: If the blood pressure (BDPR > 80) and glucose level of diabetic patients reach (GLUC ≥ 125), the insulin injection will be high, which will lead to the death of diabetic patients. The black arrows in the figure mark the predictive evaluation of the two attributes.

Show the future forecast prediction assessment done on the classification resulted attributes (Blood pressure and Glucose level).
Cost/benefit matrix
“Figure 4” presents the cost/benefit assessment matrix for 281 diabetes patients datasets achieved by experiment measurements into four parts. The first part indicates the threshold plot curve ratio between the classified instances from 0 to 1 and the second part indicates the predicted confusion matrix between the tested positive and tested negative clusters with an accuracy of 99.28%. From 281 instances 68.68% classified as tested positive for the first prediction and 30.60% for the second prediction in the matrix. In addition, one instance with a ratio of (0.36%) classified as tested negative in both first and second prediction.

Show the cost/benefit assessment achieved by the decision tree J48 machine learning classifier into four parts as explained in the text.
Moreover, the third part presents the classified instance cost/benefit plot graphically between the predicted clusters 0 and 1 from (0 to 193%) predicted instances and fourth part shows the cost matrix of two key attributes (glucose level and blood pressure) with the total gain of 118.13% and a random ratio of 120.13% in prediction instances of 281 diabetes patients.
Discussion
In this study, the machine-learning technique is instigated on a data-mining platform with a dataset of 281 patients suffering from diabetes. The data are collected only from Pakistan for the assessment of diabetes mellitus prevalence by determining J48 classifier and linear regression to forecast the classification results on invasive and non-invasive medical attributes/variables. It includes the age (of the patient), gender (male and female), glucose level, body mass index, hypertension, diet (healthy and unhealthy), and utmost 100 other features to accurately measure the cost/benefit ratio of the predictive negative instance on classification results for medical specialists. Why the Pakistan region is significant25? Because it voluntarily enters in the developing countries, where the modern life necessitates, require with the enormous number of ratios and diabetes is the vastly spreading disease causing many other symptoms of cancer, blindness, and heart strokes.
The assessment has been launched on the data-mining platform (Weka) and the data set was divided into two parts for training and testing at a ratio of 20:80%. The 20 percent of the data was used to train the machine and measure the outcome whereas; the rest of 80 percent was used for testing analysis. In addition, a complete dataset of 281 patients was analyzed on the experimental mode of Weka for the assessment of decision tree classifiers namely J48 with an accuracy of (99.28%), J48 consolidation is (98.93%), J48 graft is (98.93%), and Hoeffding tree is (91.10%) respectively, also shown in “Table 3”. The J48 decision tree classification results show that the average accuracy is 99.28% and the error rate is 0.08%. In addition, the average Kappa was 0.98%, the true positive rate was 0.99%, the false positive rate was 0.08%, the precision, the recall rate, ROC and F-matrix were 0.99%, and the PRC and MCC were 0.98%.
The outcomes of the invasive and non-invasive medical features used in this study indicate that this assessment can accurately help to predict the patients of diabetes and pre-diabetes without necessitating any preliminary laboratory tests and equally useful for the medical specialists to analyze the cost/benefit on the tested negative patients for diabetes. In addition, the J48 decision rule generated during the assessment showed the main characteristics of diabetic patients were blood pressure and blood glucose levels. Therefore, Therefore, this study proposes a prediction that age is a potential and root variable, followed by blood pressure and blood sugar levels. These implementations are useful for low socioeconomic status regions around the globe, i.e. Africa, Asia, and other developing countries.
The cost-benefit principles span the key area of diabetes from the patients to analyze the record statistics of insulin level or with other treatment terminologies of diabetic patients. Put differently, cost-benefit analysis frequently finds quantification and traditionally includes all the valid factors of interest, rather than determining, reckoning and subtracting all negative ratios, called costs. The major difference between these two terms is whether the planned action is advisable or not for the patients. In Pakistan, diabetes is a rapidly growing vascular disease and is intimately associated with increased visual impairments with other subsets. The cost-benefit analysis can undoubtedly help the medical specialists and private doctors to analyze the tested negative ration of a patient with their medical stages. It works diligently with an accurate prediction of tested positive and tested negative ratios.
In the proposed method, cost/return has a good predicted percentage. From 281 instances, the positive rate of the predicted confusion matrix was 193 (68.68%) and the negative was 86 (30.60%). These two instances are classified as non-category for cost analysis with a forecast ratio of 0.36%. The cost/benefit analysis graph shows a clear threshold curve prediction for medical experts. The characteristics obtained by J48 decision-making algorithm are:
-
i.
It handles discrete and continuous attributes correctly. The threshold is determined by C4.5 and is used to process continuous attributes. This value divides the data list into those whose attribute values are below the threshold and remain greater than or equal to the threshold.
-
ii.
It also handles missing values in training data.
-
iii.
After constructing the decision tree, J48 performs the appropriate pruning of the tree by pruning the branches that do not contribute to the leaf nodes.
The goal of this study is to utilize all decision-making classifiers (J48, J48 consolidation, J48 graft, and Hoeffding tree) with logistic regression assessment to identify and forecast diabetes mellitus prevalence. Similarly, the use of realistic health records collected from the seven principal hospitals of ‘Pakistan’, where the prevalence proportion of diabetes in men and women is high and explicitly mentioned in the literature. Hence, forming decision-making rules can screen the patients with diabetes mellitus and also mellitus can be controlled through organizing appropriate educational programs in developing countries that will help to govern the widespread growth of diabetes mellitus. The classification assessment of J48 proposed in this paper was set to compare with the most recent achievement from other authors as shown in table three, which clearly indicates J48 decision making classifiers have been successful in clinically meaningful research of this study.
The proposed study experiences two limitations. The first includes the training and test data partitioning of the Meta dataset, and the second is the time required to test the metadata for classification. If the metadata are analyzed on the same platform, the processing time can be further increased; it depends on the type of dataset, the number of seed inputs, and the number of experiments performed to achieve the desired result.
In conclusion, the proposed approach encourages and supports medical professionals to correctly assess the classifications of diabetes mellitus patients. In addition, future study can be conducted by utilizing this approach on Metadata. Particularly, the medical specialists can use the proposed approach to forecast diabetes mellitus patient’s attributes on the initial stages of apparent prevalence or on the initial stage of screening and diagnosing diabetes mellitus type 1, type 2 and gestational under the more constant decision-making phase.
Methods
The Ethics committee of Yanshan University, Natural science foundation of China Hebei province, approved the study and all experiments procedures conformed to the Declaration of Helsinki. All participants provided written informed consent after all procedures were explained orally and in writing.
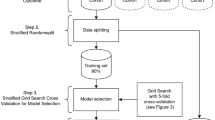
“Figure 5” displays the assessment framework used in this work for screening and cost benefit implications (performed in six steps) in diabetes patients. Initially, the real-life diabetes mellitus data was acquired and preprocessed afterward; the data was used for evaluation and assessment. Secondly, the updated plugins of machine learning J48 decision tree classifier were used on Weka version 3.9.2 “data mining platform” for classification measurements and assessment. Additionally, the linear regression method was employed on the results of machine learning classifiers to forecast the future predictions.

Show the assessment methodology framework into six steps as explained in the main text.
The realistic dataset of 563 diabetes patients was collected by questionnaire design and verbal interviews from seven principal hospitals of Pakistan through time span of June 2017 to April 2018 with 108 medical features. “Figure 6” shows the tributaries namely with percentage of patients suffering from diabetes includes Victoria hospital (14.92%), Sharif medical college (13.32%), Sheikh Zaid hospital (15.09%), Civil hospital (15.45%), Quaid Azam medical college (16.69%), Central medical hospital (11.72%), and Khalid Saeed hospital (12.78%). The first part of figure shows the number of diabetes mellitus patients visited the mentioned hospitals by months and the second part show the total number of patients in each hospital graphically.

Show the diabetes data collection flow into two parts as described in the text.
Out of 563 records, 282 records were removed from the dataset due to missing values in various attributes i.e. glucose level, patient’s occupation, last visit to the doctor, insulin injection intake, body mass index (BMI), work stress and many others out of 108 attributes. 281 records were analyzed for the model assessment of cost benefit analysis of diabetes patients. These records include the diabetes mellitus patients both male and female from age of (≥15) and (≤87), who was suffering other disease symptoms equally. The parameter selection for each attribute was analyzed carefully for the assessment as Age and gender represent demographic characteristics. Patients Glucose level (mmoI/L) has a relation with the age and diet. Family history of diabetes was defined as any family member previously diagnosed by a physician as diabetic or pre-diabetic (Yes = 1, No = 0). BMI was calculated as body weight divided by the square of height in meters and (BMI ≥ 25) was defined as overweight. Out of 108 attributes, other attributes were optimized at the initial stage by the values of 0 and 1 according to their mellitus relations. Numeric attributes were instantly changed to the nominal values presenting 0 as No and 1 as Yes by (3) to reduce the cognitive complexity of the dataset to properly conduct the assessment but carefully used the real values for the attributes like blood pressure, glucose and insulin to forecast the cost benefit predictions.
Data mining platform Waikato environment of knowledge analysis (Weka/v 3.9.2) was utilized for the preprocessing, classification assessment of cost benefit analysis, and forecast prediction of diabetes mellitus patients by updated plugins of machine learning algorithms K-means for clustering and J48 for classification26. In addition, linear regression was used on Weka for the future forecast assessment27. Initially, data was divided into 20/80 ratios in Weka by automatic filtering method, 20% was used as training dataset to train the machine, and 80% was utilized for initial classification evaluation to assign class attributes to final data sets for testing as positive and negative status of diabetes mellitus. Finally, the 100% dataset of 281 instances were utilized on the experimenter mode of Weka for the final assessment of classification and clustering. In addition, the generated results of classification were implemented for the forecast prediction analysis by linear regression. The advantage of using Weka is to avoid the over fitting and unnecessary complexity in the dataset.
K-means clustering algorithm is distance-based cluster and the distance measured by similarities in the cluster instances20. The K-means parameters selection was 100 for maximum canopies to hold in memory, minimum canopy density was set as 2.0, canopy pruning rate as 10000, canopy T1 as (−1.25), canopy T2 as (−1.0), functioning distance was set as Euclidean20, maximum iterations as 500, number of clusters as 2, execution slots as 1, and seeds value as 10.
The idea works behind K-means is invariably to define the K centroids for each cluster but these cluster centroids should be carefully placed in a scheming way because of the diverse locations produces inconsistent results. Therefore, the centroids should be prudently placed with the certain distance as much as possible from each other. After that it instantly seizes each point legitimately belonging to the dataset given and positively associate it to the most adjacent centroids. If there is no specific point remains than the first phase of the algorithm process is complete and the primary groupie is done. By this stage, it recalculates the K new centroids as barycenter of the clusters as resulted from the first phase. A new bound assuredly has to be done correctly after the K creative centroids between the points of same dataset and the most adjacent new centroid. For that the continuous loop generates to shift the specific location of K centroids on each necessary step and repeats until no centroid move anymore. This process executes as in (4–6).
Where n is the number of data points in the i clusters and k is the number of cluster centers and \(\parallel {x}_{i}^{(j)}-{c}_{j}\parallel \) represents the Euclidean distance between \({x}_{i}^{(j)}\) and cj. Basically, the Kmean algorithm for the clustering is composed of the following steps on which it works further modeled as in (7, 8).
-
i.
Place the K points into the considerable space as represented by the objects that are being clustered. These essential points sufficiently indicate the initial group of centroids.
-
ii.
Properly assign each object to the group that undoubtedly possesses the most adjacent centroid.
-
iii.
After the assigning all objects, recalculate the prominent position of K centroid.
-
iv.
Repeat fiercely the second and third step until the centroids no able to move more significantly. This efficiently produces the possible separation of groups objects which the matric to be minimized can be accurately calculated.
Decision tree classification helps to find out the vectors behave for the instance numbers3,12,22,23. After separation assessment of positive and negative clusters, this study adopted four decision-making classification algorithms with updated plugins in order to achieve the cost benefit classification for diabetes mellitus patients dataset namely J48, J48 consolidation, J48 graft, and Hoeffding tree. Finally, the J48 machine learning algorithms was utilized with 10-fold cross validation technique for the decision-making classification after the comparison assessment of four algorithms. In addition, the final classification results of J48 were used to forecast the predictions by linear regression on Weka. Essentially, J48 algorithm obtains the extension of ID3 and typically retains the additional formats for solving down the missing values, values ranges, and rules derivation. In addition, it is precisely an open source java implementation program of C4.5 algorithm in Weka (3.9.2), which includes three fundamental steps in our assessment model as:
-
i.
In the specific case where the instance correctly belongs to a similar class, the tree represents the leaf that replaces the label with the corresponding class.
-
ii.
The information is calculated for each attribute. At that considerable time, the gain information was being calculated by a test on attributes.
-
iii.
The best branching attribute for decision tree assuredly found on the consistent basis of the present selection criterion.
The parameter selection for J48 was 100 as batch size with confidence interval of 0.25%, minimum number of objects and the decimal number places were set as 2, numbers of folds were set as 3, and error pruning as false with number of seeds equal to 1. The counting gain process would gently take the Entropy’s, where Y is calculated as (9, 10) and the total gain is calculated as in (11) to split the argument Y by value of J. Furthermore, the kappa stats for the classification accuracy measurements were analyzed as (12, 13).
The successful outcomes of J48 were implemented on linear regression to forecast the cost benefit assessment of decision tree attributes. Parameters for linear regression were set as 100 for batch size with attribute selection method M5, number of decimal places were set as 4 with ridge rate as (1.0E-8). In addition, linear regression works by using the values 0 and 1 along the logistic regression algorithm as (14), because the logistic regression deals with binary codes of values to accurate mapping of data items and has the ability to perform admirably the specific task using sigmoid function layers as followed in (15–17).
Ethical approval and informed consent
Approval: We confirm that all experimental protocols were approved by Yanshan institute and has approved in method section of this paper. Accordance: All methods were carried out in accordance with the relevant guidelines and regulations. Informed consent: We confirm that informed consent was obtained from all participants and/or their legal guardian/s. Patient’s information: We confirm that informed consent to publish identifying information/images was obtained must be included in the methods section and we also identify that images/video/details about patient’s, has been removed from the paper due to policy restrictions.
Data Availability
All data utilized in this study is available as a supplementary information file.
References
Chen, P. & Pan, C. Diabetes classification model based on boosting algorithms. BMC Bioinformatics 19, 109 (2018).
Bao, C. et al. Diabetes in midlife and risk of cancer in late life: A nationwide Swedish twin study. Int. J. Cancer 143, 793–800 (2018).
Sohail, M. N., Jiadong, R., Uba, M. M. & Irshad, M. A Comprehensive Looks at Data Mining Techniques Contributing to Medical Data Growth: A Survey of Researcher Reviews. In 21–26, https://doi.org/10.1007/978-981-10-8944-2_3 (Springer, Singapore, 2019).
Jothi, N., Rashid, N. A. & Husain, W. Data Mining in Healthcare – A Review. Procedia Comput. Sci. 72, 306–313 (2015).
Muhammad, M. U., Asiribo, O. E. & Noman, S. M. Application of Logistic Regression Modeling Using Fractional Polynomials of Grouped Continuous Covariates. Niger. Stat. Soc. Ed. Proc. 1st Int. Conf. 1, 144–147 (2017).
Parapuram, G. K., Mokhtari, M. & Hmida, J. B. Prediction and Analysis of Geomechanical Properties of the Upper Bakken Shale Utilizing Artificial Intelligence and Data Mining. Prediction and Analysis of Geomechanical Properties of the Upper Bakken Shale Utilizing Artificial Intelligence and Data Minin, https://doi.org/10.15530/urtec-2017-2692746 (2017).
Kranjc, J., Orač, R., Podpečan, V., Lavrač, N. & Robnik-Šikonja, M. ClowdFlows: Online workflows for distributed big data mining. Futur. Gener. Comput. Syst. 68, 38–58 (2017).
Ashrafuzaman, M., Alam, M. T. & Abdullah-Al-Harun, M. An Engineering Module to Identify Potential Diabetes Patients and Preventive Measures for Diabetes in Developing Countries like Bangladesh. In 405–409, https://doi.org/10.1007/978-981-10-9035-6_75 (2019).
Shermer, M. Heavens on earth: the scientific search for the afterlife, immortality, and utopia.
Mostafa, S. A. et al. Modelling incremental benefits on complications rates when targeting lower HbA 1c levels in people with Type 2 diabetes and cardiovascular disease. Diabet. Med. 35, 72–77 (2018).
For Disease Control, C. National Diabetes Statistics Report, 2017 Estimates of Diabetes and Its Burden in the United States Background, https://doi.org/10.1177/1527154408322560 (2017).
Sohail, N., Jiadong, R., Uba, M., Irshad, M. & Khan, A. Classification and cost benefit Analysis of Diabetes mellitus Dominance. Int. J. Comput. Sci. Netw. Secur. 18, 29–35 (2018).
Melmed, S., Polonsky, K. S., Larsen, P. R. & Kronenberg, H. Williams textbook of endocrinology. (Elsevier, 2016).
Whiting, D. R., Guariguata, L., Weil, C. & Shaw, J. IDF Diabetes Atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 94, 311–321 (2011).
Cho, N. H. et al. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 138, 271–281 (2018).
Shamshirgaran, S. M., Jorm, L., Lujic, S. & Bambrick, H. Health related outcomes among people with type 2 diabetes by country of birth: Result from the 45 and Up Study. Prim. Care Diabetes 13, 71–81 (2019).
Bala, R., Sikka, S. & Singh, J. A Comparative Analysis of Clustering Algorithms. Int. J. Comput. Appl. 100, 975–8887 (2014).
Rojas, E., Munoz-Gama, J., Sepúlveda, M. & Capurro, D. Process mining in healthcare: A literature review. J. Biomed. Inform. 61, 224–236 (2016).
Saini, S. Hybrid Model Using Unsupervised Filtering Based On Ant Colony Optimization And Multiclass Svm By Considering Medical Data Set. Int. Res. J. Eng. Technol. 4, 2565–2571 (2017).
Sohail, M. N., Ren, J. & Muhammad, M. U. A Euclidean Group Assessment on Semi-Supervised Clustering for Healthcare Clinical Implications Based on Real-Life Data. Int. J. Environ. Res. Public Heal. 2019, Vol. 16, Page 1581 16, 1581 (2019).
Brown, A. W., Kaiser, K. A. & Allison, D. B. Issues with data and analyses: Errors, underlying themes, and potential solutions. Proc. Natl. Acad. Sci. USA 115, 2563–2570 (2018).
Sohail, M. N., Jiadong, R., Irshad, M., Uba, M. M. & Abir, S. I. Data mining techniques for Medical Growth: A Contribution of Researcher reviews. Int. J. Comput. Sci. Netw. Secur. 18, 5–10 (2018).
MN, S. et al. Why only data mining? A pilot study on inadequacy and domination of data mining technology. Int. J. Recent Sci. Res. 9, 29066–29073 (2018).
Sohail, M. N. et al. An Accurate Clinical Implication Assessment for Diabetes Mellitus Prevalence Based on a Study from Nigeria. Process. 2019, Vol. 7, Page 289 7, 289 (2019).
Stewart, F. Country experience in providing for basic needs. Finance Dev. 16, 23–6 (1979).
Witten. Weka - Data Mining with Open Source Machine Learning Software in Java. weka Available at, https://www.cs.waikato.ac.nz/ml/weka/ (2016).
Sohail, M. N. et al. Forecast Regression analysis for Diabetes Growth: An inclusive data mining approach. Int. J. Adv. Res. Comput. Eng. Technol. 7, 715–721 (2018).
Barrios, O. et al. Predictive modeling for presumptive diagnosis of type 2 diabetes mellitus based on symptomatic analysis. In 2017 IEEE XXIV International Conference on Electronics, Electrical Engineering and Computing (INTERCON) 1–4, https://doi.org/10.1109/INTERCON.2017.8079667 (IEEE, 2017).
Acknowledgements
The Natural Science Foundation of Hebei Province, China under Grants of 61572420, 61472341, and 61772449 funded this research.
Author information
Authors and Affiliations
Contributions
Writing-Original draft preparation, methodology, software and formal analysis have been done by Muhammad Noman Sohail; conceptualization, validation, data and visualization, has done by Muhammad Noman Sohail and Musa Uba Muhammad; supervision, resources, project administration, and funding acquisition has done by Ren Jiadong; investigation has done by Musa Uba Muhammad and Muhammad Irshad; in closing, writing-review and editing have carefully done by Noman Sohail, Wasim Iqbal, Jehangir Arshad and Antony John Verghese.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sohail, M.N., Jiadong, R., Uba, M.M. et al. A hybrid Forecast Cost Benefit Classification of diabetes mellitus prevalence based on epidemiological study on Real-life patient’s data. Sci Rep 9, 10103 (2019). https://doi.org/10.1038/s41598-019-46631-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-46631-9
This article is cited by
-
Exploring antibiotic resistance genes, mobile gene elements, and virulence gene factors in an urban freshwater samples using metagenomic analysis
Environmental Science and Pollution Research (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
