
Abstract
Antenatal corticosteroids (ANS) are the major intervention to decrease respiratory distress syndrome and mortality from premature birth and are standard of care. The use of ANS is expanding to include new indications and gestational ages, although the recommended dosing was never optimized. The most widely used treatment is two intramuscular doses of a 1:1 mixture of betamethasone-phosphate (Beta-P) and betamethasone-acetate (Beta-Ac) – the clinical drug. We tested in a primate model the efficacy of the slow release Beta-Ac alone for enhancing fetal lung maturation and to reduce fetal corticosteroid exposure and potential toxic effects. Pregnant rhesus macaques at 127 days of gestation (80% of term) were treated with either the clinical drug (0.25 mg/kg) or Beta-Ac (0.125 mg/kg). Beta-Ac alone increased lung compliance and surfactant concentration in the fetal lung equivalently to the clinical drug. By transcriptome analyses the early suppression of genes associated with immune responses and developmental pathways were less affected by Beta-Ac than the clinical drug. Promoter and regulatory analysis prediction identified differentially expressed genes targeted by the glucocorticoid receptor in the lung. At 5 days the clinical drug suppressed genes associated with neuronal development and differentiation in the fetal hippocampus compared to control, while low dose Beta-Ac alone did not. A low dose ANS treatment with Beta-Ac should be assessed for efficacy in human trials.
Similar content being viewed by others

Introduction
Antenatal corticosteroids (ANS) are the major perinatal intervention to reduce the incidence of respiratory distress syndrome and neonatal mortality associated with preterm birth1. While ANS are considered to be safe, expanding treatments to gestations beyond 24 to 34 weeks may change the risk to benefit ratio2. A recent large trial demonstrated that ANS decreased the respiratory complications and the need for respiratory support for infants between 34 and 37 weeks gestational age3. ANS also decreased neonatal respiratory morbidity for elective C-section deliveries at term gestation4,5. ANS also are being used for periviable deliveries at 22–24 weeks gestation6. If widely adopted for these expanded indications and depending on the elective C-section rate, the majority of pregnancies worldwide could be treated with ANS7,8. However, the limited knowledge regarding the optimal formulation, dosing and potential delayed effects into adult life on outcomes such as metabolic syndrome suggests caution for the expanded use of ANS.
There also may be unrecognized adverse effects of ANS on different patient populations. The largest burden of prematurity is in low and middle-resource countries and in a recent large cluster-randomized trial ANS increased mortality for exposed infants with birthweight above the 5th percentile9,10. Hypoglycemia also was increased with ANS exposure in late preterm newborns (with gestational ages between 340 and 366 weeks)3. In experimental studies ANS caused hippocampal degeneration and HPA axis dysfunction in macaques11,12,13 and decreased fetal and brain growth in sheep and rats14,15,16. These findings were consistent with observational studies showing that ANS impaired fetal growth17 and decreased neuronal density in the hippocampus of newborns18.
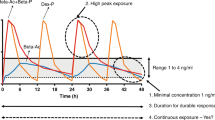
As with any medication, treatment strategies should maximize the benefits and minimize potential toxic effects. ANS are recommended by the World Health Organization to be given to the mother as intramuscular (IM) dexamethasone-phosphate (Dex-P), or a combination of equal parts of Beta-P and Beta-Ac (clinical drug)19. Phosphate and acetate formulations have distinct pharmacokinetic profiles and effects20,21. Phosphate preparations are rapidly dephosphorylated resulting in early high plasma concentrations and short half-lives in the mother and fetus. Beta-Ac is slowly deacetylated resulting in low peak plasma levels and long half-life20. In fetal sheep the clinical drug was superior to Dex-P or Beta-P alone for causing physiologic and biochemical maturation of the lung22. In contrast, a single weight-based dose of Beta-Ac improved maturation comparably to the clinical drug, with a decreased fetal exposure to Beta23.
Any pharmacological intervention for treating a pregnant woman to benefit the fetus should be considered high risk. To translate a new ANS therapy from animal models to humans, a validation in primates is desirable. We evaluated a lower dosing strategy using Beta-Ac for fetal lung maturation and transcriptional effects on the fetal lung and brain in the Rhesus macaque.
Results
Beta-Ac enhances fetal lung maturation at 5 days
To compare Beta-Ac with the clinical drug for fetal lung maturation, pregnant Rhesus macaques were treated with a single IM injection of either Beta-Ac (0.125 mg/kg or 0.06 mg/kg), saline (control) or the clinical drug (0.25 mg/kg) and delivered 5 days after treatment (Table 1). ACS induce fetal lung maturation by a combination of increased surfactant production, structural changes, and improved water clearance resulting in increased lung compliance. Both the clinical drug and Beta-Ac (0.125 mg/kg) improved static lung compliance (Fig. 1A,B). Beta-Ac 0.06 mg/kg inconsistently increased lung compliance with 3 out of 5 treated animals having pressure-volume curves similar to control. The main lipid component of surfactant is saturated phosphatidylcholine (SatPC), which can be used as a marker of lung surfactant content and indicator of biochemical lung maturation24. Both Beta-Ac (0.125 mg/kg) and the clinical drug increased the SatPC in the bronchoalveolar lavage fluid compared to control, while the increase with Beta-Ac (0.06 mg/kg) was not significant (Fig. 1C).

(A) Pressure-volume curves showing comparable improved static compliance after treatment with Beta-Ac (0.125 mg/kg) and the clinical drug. (B) Lung gas volumes were increased significantly for Beta-Ac 0.125 mg/kg and the clinical drug. (C) Saturated phosphatidylcholine (SatPC) concentration in the bronchoalveolar lavage fluid (BALF) increased with Beta-Ac 0.125 mg/kg and the clinical drug compared to control. *p-value < 0.05 vs. control.
Confocal microscopy of immunofluorescent staining of the fetal lung for the epithelial cell marker TTF-1, smooth muscle actin (SMA), and type II alveolar cell markers pro-SPC, and ABCA3 showed no differences in the relative numbers of cells positive for these markers 5 days after treatment (Supplemental Fig. 1). Further, there were no differences in the proportion of cells expressing the cell cycle marker Ki-67.
Transcriptomic effects of the clinical drug and Beta-Ac on the fetal lung
RNA-sequencing analyses were performed on whole lung tissue from fetuses delivered 4 hours and 5 days after treatment with the clinical drug and 6 hours and 5 days after Beta-Ac (Fig. 2). Principal component analysis of transcriptomic changes separated animals 4 h after treatment with the clinical drug, 6 h after Beta-Ac, and control animals, with the animals treated with the clinical drug being the most distant from the others (Fig. 2A). In contrast, by 5 days the clinical drug and Beta-Ac overlapped (Fig. 2B). Further, the correlation heatmap showed the most distinct transcriptome profiles for animals treated with the clinical drug 4 h prior to delivery (Fig. 2C).

Transcriptomic analysis was performed on whole lung RNA 4 hours and 5 days after administration of the clinical drug, and 6 hours and 5 days after Beta-Ac 0.125 mg/kg and from saline-treated animals (n = 3 animals per group). 3-dimensional principal component analysis (PCA) was generated using log-transformed read counts. (A) At the early timepoint PCA separated the animals treated with the clinical drug at 4 h, Beta-Ac at 6 h, and controls. (B) At 5 days there is separation of control animals and overlap of animals treated with the clinical drug and Beta-Ac (C) Sample correlation heatmap displaying the similarity in gene expression profile. Red color indicates increasing sample correlation and yellow color indicates decreasing sample correlation. Dendrogram clustering indicates the overall similarity of the samples. Both analyses showed separation of the clinical drug at 4 h and overlap of animals in the other treatment groups.
Differential expression analysis was performed using the EdgeR package on R with differentially expressed genes determined using p-value < 0.05, q-value < 0.1 and fold-change > 1.5. At the times of high fetal plasma concentration the clinical drug caused differential expression of 1,779 genes while Beta-Ac caused the differential expression of only 393 genes, of which 372 were common to both treatments. The common differentially expressed genes had similar magnitude of fold changes, with a Pearson correlation value of 0.87 (Fig. 3A,B). In contrast, after 5 days the clinical drug and Beta-Ac differentially expressed a similar number of genes (318 and 419 genes, respectively), with 185 genes differentially expressed in common. These commonly regulated genes at 5 days also had a similar magnitude of differential expression and highly correlated log fold-change values (Fig. 3A,C). By transcription factor binding site prediction and protein regulation or interaction prediction, several of the common top regulated genes at both timepoints have either a glucocorticoid receptor enhancer motif or are predicted to be regulated or interact with the NR3C1 receptor. Several common regulated genes are also reported in the literature to be associated with “lung expression”, “respiratory disease”, and “lung cell line” (Fig. 3A).

Top common differentially expressed genes in each group relative to control were determined using thresholds of p-value < 0.05, q-value < 0.1 and fold-change > 1.5. (A) Top 20 up and down regulated genes relative to control and predicted regulation by the glucocorticoid receptor (GR) either by the presence of a GR motif or predicted interaction by ingenuity pathway analysis. Genes reported in the literature to be associated with “lung”, “respiratory disease”, or “lung cell line” are bolded. Scatterplots of log fold-changes (logFC) of differentially expressed genes from. (B) Beta-Ac 6 h and the clinical drug 4 h relative to control and (C) Beta-Ac 5d and the clinical drug 5d relative to control. Most commonly differentially expressed genes had a similar direction and magnitude of changes. There was strong correlation between logFC values (r = 0.87 for 6 h and 4 h; r = 0.96 for 5d).
Genes differentially regulated by either of the ANS treatments were associated with several similar biological processes. At the early time point induced genes were associated with “cellular localization”, “developmental process”, “ion and protein transport” while suppressed genes were associated with “cellular morphogenesis”, “chemotaxis”, and “immune responses”.
Despite the similarities, there were large differences between biological processes and pathways that were differentially regulated in the lung by the clinical drug and Beta-Ac relative to control at the time of peak drug concentration in the fetal plasma (Fig. 4). The clinical drug had larger inhibitory effects on immune system processes and development, including suppression of Th1, Th2 and Th17 lymphocyte differentiation, lymphocyte proliferation and activation, and cytokine signaling. The clinical drug also modulated biological processes related to organ development and morphogenesis, which were only weakly associated with Beta-Ac treatment. Specifically, genes inhibited by the clinical drug were strongly enriched for angiogenesis and vascular development, endothelial cell proliferation, epithelial tube morphogenesis, and canonical Wnt signaling. Genes differentially expressed by the clinical drug at the early time point may not be contributing to lung maturational responses as the 2 treatments resulted in similar improvement in lung gas volume and similar RNA profiles at 5 days.

Gene set enrichment analysis comparing the clinical drug and Beta-Ac to control in the lung at time of peak Beta plasma concentration in the fetus. Selected gene ontology terms are displayed with the bar chart representing log p-values. Positive p-values denote induced genes and negative p-values denote suppressed genes. Genes suppressed by the clinical drug were more strongly associated with morphogenesis and developmental processes than genes suppressed by the Beta-Ac.
Transcriptomic effects in the fetal hippocampus at 5 days
To evaluate potentially toxic effects of ANS on the fetal brain development we compared the transcriptome of the fetal hippocampus 5 days after ANS treatment. The principal component analysis and the correlation heatmap demonstrate that control animals cluster separately and distant from animals treated with the clinical drug (Fig. 5A,B). In contrast, animals treated with Beta-Ac 0.125 mg/kg are interspersed between the other groups but with wide variation among samples.

Transcriptomic analysis was performed for fetal hippocampus from saline-treated animals and 5 days after administration of ANS (n = 5 animals per group). (A) 3-dimensional principal component analysis (PCA) was generated using log-transformed read counts. (B) Sample correlation heatmap displaying the similarity in gene expression profile. Red color indicates increasing sample correlation and yellow color indicates decreasing sample correlation. Dendrogram clustering indicates the overall similarity of the samples. Both analyses showed separation of the control from animals treated with the clinical drug, while animals treated with Beta-Ac are interspersed between the controls and clinical treatment animals. (C) Top differentially induced and suppressed genes by the clinical drug in the hippocampus at 5 days. Genes are ordered by magnitude of gold change; p values are adjusted by the Benjamin-Hochberg method.
By differential expression analysis 1612 genes were differentially regulated (788 induced, 824 suppressed) in the hippocampus by the clinical drug at 5 days compared to control (Fig. 5C). There were no statistical differences between gene expression levels in the Beta-Ac treated animals compared to control. Genes induced by the clinical drug were associated with the regulation of synapse maturation and semaphorin interactions, among others. Suppressed genes were associated with regulation of neurogenesis, neuron, projection development, cellular morphogenesis and nervous system development (Figs 6 and 7).

Gene set enrichment analysis comparing differentially expressed genes for the clinical drug compared to control in the fetal hippocampus. There was no differential expression between Beta-Ac and control. Selected gene ontology terms are displayed with the bar chart representing log p-values. Positive p-values denote induced genes and negative p-values denote suppressed genes.

Network of genes suppressed by the clinical drug in the fetal hippocampus at 5 days associated with the biological processes of neurogenesis and neuron differentiation.
Discussion
Since 1972, use of ANS for women at risk of preterm labor at 24–34 weeks gestation decreased the incidence of respiratory distress syndrome and mortality in preterm newborns, but the formulation and dosing was never optimized by pharmacokinetic analyses or for safety2,25. In fact, the expanding use of ANS beyond the 24 to 34 week gestational has identified previously unrecognized risks such as hypoglycemia in late preterm infants and increased mortality in middle and low-resource countries3,9. We report that fetal lung maturation in the primate can be achieved with a single weight-based dose of Beta-Ac that avoided fetal exposure to higher Beta levels from the Beta-P component of the clinical drug. Beta-Ac minimized early transcriptional changes in the fetal lung associated with immunity and morphogenesis, and at 5 days in the fetal hippocampus associated with nervous system development despite similar pulmonary maturation. As even routine short-term use of corticosteroids is associated with risks, and complications are dose related26, the lowest fetal exposure sufficient to get the maturational benefit should be the goal.
Different steroid formulations and dosing intervals are used around the world based on a total dose of 24 mg with minimal experimental or clinical data to support equivalency25. We previously showed with fetal sheep that a single dose of Beta-Ac that was 25% of the standard 2-dose treatment with the clinical drug yielded similar improvements in gas exchange and lung compliance 2 days after treatment23. This treatment strategy in sheep exposes the fetus to a peak drug concentration that is 10% of the peak drug concentration with the clinical drug, while providing continuous fetal exposure to betamethasone for 24 hours23.
In the primate, treatments with Beta-Ac alone and the clinical drug resulted in similar mechanical induction of lung maturation as demonstrated by the pressure-volume curves and similar increase in the surfactant content, measured by the SatPC concentration in the BALF. Increased surfactant production by the premature lung decreases the severity and incidence of RDS in preterm newborns. Moreover, there were no differences between the lung transcriptomes 5 days after treatment. Interestingly, the proportions of cells expressing the epithelial marker TTF-1 or the type 2 alveolar cell markers, ABCA3 and SPC, were similar among treatment groups and control at 5 days, suggesting that ANS induced transient changes in expression of mRNA but not persistent cellular differentiation to increase the number of surfactant producing cells. This finding is consistent with the observation that the effects of ANS are transient and clinical trials have not consistently demonstrated benefit in decreasing RDS beyond 7 days after treatment1,27.
The early transcriptomic changes in the lung 4 to 6 hours after ACS exposure offers new insight into the complex signaling mechanism of lung maturation induced by corticosteroids. While most studies have focused on the effects of ACS on the endpoints of increased surfactant production and improved lung structure here we show that ACS has large effects on developmental, vascularization, cell signaling, and cell cycle pathways. These multiple effects likely all contribute to the improved lung function seen in preterm newborns after ACS treatment. More interestingly, 5 days after ACs treatment, transcriptional changes were limited and were associated with ion transport and cytoskeletal organization. These changes could be associated with continued structural and tissue water balance maturation. However, most of the effects of ACS on gene expression had disappeared by 5 days.
We provide new information that the high peak drug level from the clinical drug was associated with more suppression of lung immune responses, angiogenesis and developmental pathways based on transcriptome analyses. While the clinical drug regulated a larger number of genes and pathways than Beta-Ac, the genes that were commonly differentially expressed had similar magnitudes of change, indicating that the additional steroid exposure may not be contributing to more maturational signaling. Changes in expression of other genes may only have harmful harmful side effects. While in high resource environments ANS has not been associated with increased risk of maternal or neonatal infection or sepsis28, in the subgroup of patients with preterm rupture of membranes the risk of chorioamnionitis was increased with repeated treatments with ANS29. In middle and low-resource countries the increased infant mortality associated with ANS treatment may be caused by increased the risk of infection10. Due to cost and availability, the international cluster-randomized trial used Dex-P given as 4 intramuscular doses of 6 mg every 12 hours9. This dosing strategy, provides fetal exposure to ANS for greater than 48 hours but with 4 high peak fetal plasma levels that are not necessary in animal models22,30. Avoiding high fetal concentrations of corticosteroids should minimize the treatment effects on the maternal and fetal immune responses and the risk of perinatal infection.
More concerning are the reports of direct effects of glucocorticoids on the fetal brain. Preterm newborns exposed to glucocorticoids had decreased number of neurons in the hippocampus12, consistent with a previous report of increased apoptosis of neuron in the hippocampus of macaques after treatment with glucocorticoids31. We found that fetal exposure to the clinical drug resulted in suppression of genes associated with neurogenesis and nervous system development 5 days after treatment. There were no differences in the hippocampus transcriptome between animals treated with Beta-Ac compared to control but we did observe a wide variability in the Beta-Ac group with some animals clustering with controls and others with the clinical drug. This variability could be due to individual variations regarding drug metabolism affecting the fetal exposure to the treatment or genetic variants affecting the molecular response to corticosteroids. In our limited sample size the sex of the animal did not seem to affect the response. The most recent meta-analysis of antenatal corticosteroids showed a trend towards reduced neurodevelopmental impairment after a single course of ANS in infants less than 34 weeks gestation in high resource countries28. There are no data on neurodevelopmental outcomes for late preterm infants where the clinical benefits of ANS are small and may not outweigh the risks. This benefit to risk ratio may be even less for elective C-sections. Even more problematic are reports of increased renal disease, obesity and metabolic syndrome at advanced ages in sheep and baboons exposed as fetuses to ANS32,33,34. These effects cannot be evaluated in human populations being treated with ANS today and may be at long-term risk of fetal effects on adult outcomes.
Here we demonstrate that a clinically relevant dose of ANS used for fetal lung maturation caused profound and early changes in transcriptional networks that control lung development and immunity and persistent changes on brain development pathways. Many of the changes can be avoided by low-dose Beta-Ac while preserving the physiological maturational effects in a nonhuman primate model. This strategy should be considered for clinical trials to optimize ANS treatment in preterm infants and decrease potential toxic effects.
Methods
Animals
The Institutional Animal Care and Use Committee at the University of California Davis approved all animal procedures, which were performed at the California National Primate Research Center according to the approved protocol. Time-mated pregnant Rhesus macaques were given the clinical drug as intramuscular Celestone Soluspan® 0.25 mg/kg (6 mg/ml containing 3 mg/mL betamethasone as Beta-P and 3 mg/mL of Beta-Ac; Merck Sharp & Dohme, Kenilworth, NJ), 0.125 mg/kg Beta-Ac (a gift from Merck Sharp & Dohme, Kenilworth, NJ), 0.06 mg/kg Beta-Ac or saline prior to preterm delivery at 132 ± 2 days gestational age (term is 165 days). To investigate the early transcriptional effects, fetuses were delivered at the time of peak fetal blood Beta levels based on measurements in fetal sheep23: 4 h after the clinical drug and 6 h after Beta-Ac (n = 3 animals/group). Lung samples were frozen for RNA-sequencing. To assess the maturational effects of the interventions, other groups of fetuses were treated 5 days before delivery at 132 ± 2 days of gestation (n = 5–8 animals/group). After delivery, pressure-volume curves were measured with a syringe and pressure manometer by inflating the lungs to 40 cm H2O pressure and followed by deflation with measurements of lung volumes. The right upper lobe of the fetal lung was inflation fixed with formalin at 30 cm H2O pressure for histology; tissue samples from the right lower lobe of fetal lung and the hippocampus were snap frozen for RNA-sequencing
Saturated phosphatidylcholine and cortisol measurements
Alveolar lavage fluid was recovered from the left lung and lipids were extracted with chloroform-methanol (2:1). Saturated phosphatidylcholine (SatPC) was isolated after exposure to osmium tetroxide and quantified by phosphorus assay as previously described35. Cord blood plasma cortisol levels were measured using an ELISA kit (EA65; Oxford Biomedical Research, Rochester Hills, MI).
Immunofluorescence and confocal microscopy
Sections from paraffin-embedded tissues underwent heat-assisted antigen retrieval with citrate buffer (pH 6.0), followed by blocking with donkey or goat serum and incubation with primary antibodies overnight (Table 2). The following day, sections were incubated with species-specific Alexa Fluor antibody (Life Technologies, Carlsbad, CA), followed by DAPI (Life technologies, Carlsbad, CA, dilution 1:2000). Sections were mounted with ProLong Gold (Life technologies, Carlsbad, CA). Stained slides were imaged by confocal microscopy for co-localization of fluorescent antibodies at 40x magnification, 1024 × 1024 pixels resolution on a Nikon Eclipse A1RSi inverted microscope (Nikon Instruments Inc., Melville, NY). Confocal images were analyzed using Nikon NIS Elements software (Nikon Instruments Inc., Melville, NY), for object count and colocalization.
Statistical analyses
Statistical analyses of morphological and immunofluorescence data were performed with GraphPad Prism software (Carlsbad, CA). Values for continuous variables were compared by t-test or ANOVA followed by Holm-Sidak post-hoc analysis for multiple comparisons. Data are presented as bars with individual data points and standard deviation.
RNA isolation and sequencing
Total RNA was extracted from frozen lung tissues using the RNeasy Universal Mini Kit (Qiagen, Valencia, CA) according to the manufacturer’s instructions. RNA quality and integrity were verified using the Agilent 2100 Bioanalyzer (Agilent, Agilent Technologies, Santa Clara, CA). RNA-sequencing was performed by the Cincinnati Children’s Hospital Medical Center DNA Sequencing and Genotyping Core with a read depth of 20–30 million reads per sample for 75 bp paired-end reads. The raw sequence reads in FASTQ format were aligned to the Rhesus (Macaca mulatta) genome build MMUL1.0 using Bowtie 236. Reads were counted using featureCounts37. After checking data quality, raw read counts were filtered to exclude genes with low expression (<7 reads) and normalized using the trimmed mean of M values method38. Differential expression analyses comparing treatment groups to control and between each other were performed using EdgeR39 followed by false discovery rate adjustment using Storey’s method40. Genes were considered differentially expressed based on their fold-change relative to control (= or >1.5), p-value (<0.05) and q-value (<0.1).
Functional enrichment and pathway analysis
Differentially expressed genes were used for functional enrichment analysis of Gene Ontology and pathway terms using the ToppCluster web server41. Only unique terms associated with either induced or suppressed genes and at least 2 genes are reported. Negative log p-values represent terms associated with suppressed gene expression and positive log p-values are associated with induced gene expression. Promoter GRE cis-element was scanned using the Msig-DB motif gene sets within 4 kb around their transcription starting sites (http://software.broadinstitute.org/gsea/msigdb). The evidence that NR3C1 regulates or interacts with genes in the top hits list was obtained via literature mining using Genomatix co-citation database (Genomatix Inc.) and IPA knowledge base (Ingenuity Pathway Analysis, QIAGEN). Annotation of genes expressed in the lung or associated with respiratory disease were collected from IPA knowledge base.
Data Availability
The gene expression data discussed in this publication have been deposited in NCBI’s Gene Expression Omnibus and are accessible through GEO Series Accession Number GSE118438 (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE118438).
References
In WHO Recommendations on Interventions to Improve Preterm Birth Outcomes WHO Guidelines Approved by the Guidelines Review Committee (2015).
Jobe, A. H. & Goldenberg, R. L. Antenatal corticosteroids: an assessment of anticipated benefits and potential risks. Am J Obstet Gynecol 219, 62–74, https://doi.org/10.1016/j.ajog.2018.04.007 (2018).
Gyamfi-Bannerman, C. et al. Antenatal Betamethasone for Women at Risk for Late Preterm Delivery. N Engl J Med 374, 1311–1320, https://doi.org/10.1056/NEJMoa1516783 (2016).
Stutchfield, P., Whitaker, R., Russell, I. & Antenatal Steroids for Term Elective Caesarean Section Research Team. Antenatal betamethasone and incidence of neonatal respiratory distress after elective caesarean section: pragmatic randomised trial. BMJ 331, 662, https://doi.org/10.1136/bmj.38547.416493.06 (2005).
Nada, A. M. et al. Antenatal corticosteroid administration before elective caesarean section at term to prevent neonatal respiratory morbidity: a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol 199, 88–91, https://doi.org/10.1016/j.ejogrb.2016.01.026 (2016).
Committee Opinion No. 713 Summary: Antenatal Corticosteroid Therapy for Fetal Maturation. Obstet Gynecol 130, 493–494, https://doi.org/10.1097/AOG.0000000000002231 (2017).
Betran, A. P. et al. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990–2014. PLoS One 11, e0148343, https://doi.org/10.1371/journal.pone.0148343 (2016).
Blencowe, H. et al. Born too soon: the global epidemiology of 15 million preterm births. Reprod Health 10(Suppl 1), S2, https://doi.org/10.1186/1742-4755-10-S1-S2 (2013).
Althabe, F. et al. A population-based, multifaceted strategy to implement antenatal corticosteroid treatment versus standard care for the reduction of neonatal mortality due to preterm birth in low-income and middle-income countries: the ACT cluster-randomised trial. Lancet 385, 629–639, https://doi.org/10.1016/S0140-6736(14)61651-2 (2015).
Althabe, F. et al. The Antenatal Corticosteroids Trial (ACT)’s explanations for neonatal mortality - a secondary analysis. Reprod Health 13, 62, https://doi.org/10.1186/s12978-016-0175-3 (2016).
Epstein, M. F. et al. Maternal betamethasone and fetal growth and development in the monkey. Am J Obstet Gynecol 127, 261–263 (1977).
Uno, H. et al. Neurotoxicity of glucocorticoids in the primate brain. Horm Behav 28, 336–348, https://doi.org/10.1006/hbeh.1994.1030 (1994).
de Vries, A. et al. Prenatal dexamethasone exposure induces changes in nonhuman primate offspring cardiometabolic and hypothalamic-pituitary-adrenal axis function. J Clin Invest 117, 1058–1067, https://doi.org/10.1172/JCI30982 (2007).
Huang, W. L. et al. Effect of corticosteroids on brain growth in fetal sheep. Obstet Gynecol 94, 213–218 (1999).
Gramsbergen, A. & Mulder, E. J. The influence of betamethasone and dexamethasone on motor development in young rats. Pediatric research 44, 105–110, https://doi.org/10.1203/00006450-199807000-00017 (1998).
Jobe, A. H., Wada, N., Berry, L. M., Ikegami, M. & Ervin, M. G. Single and repetitive maternal glucocorticoid exposures reduce fetal growth in sheep. Am J Obstet Gynecol 178, 880–885 (1998).
Braun, T. et al. Fetal and neonatal outcomes after term and preterm delivery following betamethasone administration. Int J Gynaecol Obstet 130, 64–69, https://doi.org/10.1016/j.ijgo.2015.01.013 (2015).
Tijsseling, D. et al. Effects of antenatal glucocorticoid therapy on hippocampal histology of preterm infants. PLoS One 7, e33369, https://doi.org/10.1371/journal.pone.0033369 (2012).
Effect of corticosteroids for fetal maturation on perinatal outcomes. NIH Consens Statement 12, 1–24 (1994).
Samtani, M. N., Lohle, M., Grant, A., Nathanielsz, P. W. & Jusko, W. J. Betamethasone pharmacokinetics after two prodrug formulations in sheep: implications for antenatal corticosteroid use. Drug Metab Dispos 33, 1124–1130, https://doi.org/10.1124/dmd.105.004309 (2005).
Jobe, A. H. et al. Betamethasone dose and formulation for induced lung maturation in fetal sheep. Am J Obstet Gynecol 201, 611 e611–617, https://doi.org/10.1016/j.ajog.2009.07.014 (2009).
Schmidt, A. F. et al. Antenatal dexamethasone vs. betamethasone dosing for lung maturation in fetal sheep. Pediatric research 81, 496–503, https://doi.org/10.1038/pr.2016.249 (2017).
Schmidt, A. F. et al. Low-dose betamethasone-acetate for fetal lung maturation in preterm sheep. Am J Obstet Gynecol 218, 132 e131–132 e139, https://doi.org/10.1016/j.ajog.2017.11.560 (2018).
Jobe, A. H. et al. Endotoxin-induced lung maturation in preterm lambs is not mediated by cortisol. Am J Respir Crit Care Med 162, 1656–1661, https://doi.org/10.1164/ajrccm.162.5.2003044 (2000).
Brownfoot, F. C., Gagliardi, D. I., Bain, E., Middleton, P. & Crowther, C. A. Different corticosteroids and regimens for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev, CD006764, https://doi.org/10.1002/14651858.CD006764.pub3 (2013).
Waljee, A. K. et al. Short term use of oral corticosteroids and related harms among adults in the United States: population based cohort study. BMJ 357, j1415, https://doi.org/10.1136/bmj.j1415 (2017).
Norberg, H., Kowalski, J., Marsal, K. & Norman, M. Timing of antenatal corticosteroid administration and survival in extremely preterm infants: a national population-based cohort study. BJOG 124, 1567–1574, https://doi.org/10.1111/1471-0528.14545 (2017).
Roberts, D., Brown, J., Medley, N. & Dalziel, S. R. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev 3, CD004454, https://doi.org/10.1002/14651858.CD004454.pub3 (2017).
Crowther, C. A., McKinlay, C. J., Middleton, P. & Harding, J. E. Repeat doses of prenatal corticosteroids for women at risk of preterm birth for improving neonatal health outcomes. Cochrane Database Syst Rev, CD003935, https://doi.org/10.1002/14651858.CD003935.pub4 (2015).
Kemp, M. W. et al. Maternofetal pharmacokinetics and fetal lung responses in chronically catheterized sheep receiving constant, low-dose infusions of betamethasone phosphate. Am J Obstet Gynecol 215, 775 e771–775 e712, https://doi.org/10.1016/j.ajog.2016.08.017 (2016).
Uno, H. et al. Brain damage induced by prenatal exposure to dexamethasone in fetal rhesus macaques. I. Hippocampus. Brain Res Dev Brain Res 53, 157–167 (1990).
Tang, L. et al. Prenatal betamethasone exposure alters renal function in immature sheep: sex differences in effects. Am J Physiol Regul Integr Comp Physiol 299, R793–803, https://doi.org/10.1152/ajpregu.00590.2009 (2010).
Kuo, A. H. et al. Prenatal steroid administration leads to adult pericardial and hepatic steatosis in male baboons. Int J Obes (Lond) 41, 1299–1302, https://doi.org/10.1038/ijo.2017.82 (2017).
Huber, H. F. et al. Antenatal Synthetic Glucocorticoid Exposure at Human Therapeutic Equivalent Doses Predisposes Middle-Age Male Offspring Baboons to an Obese Phenotype That Emerges With Aging. Reprod Sci, 1933719118778794, https://doi.org/10.1177/1933719118778794 (2018).
Ikegami, M. et al. Surfactant metabolism in SP-D gene-targeted mice. Am J Physiol Lung Cell Mol Physiol 279, L468–476 (2000).
Langmead, B. & Salzberg, S. L. Fast gapped-read alignment with Bowtie 2. Nat Methods 9, 357–359, https://doi.org/10.1038/nmeth.1923 (2012).
Liao, Y., Smyth, G. K. & Shi, W. featureCounts: an efficient general purpose program for assigning sequence reads to genomic features. Bioinformatics 30, 923–930, https://doi.org/10.1093/bioinformatics/btt656 (2014).
Robinson, M. D. & Oshlack, A. A scaling normalization method for differential expression analysis of RNA-seq data. Genome Biol 11, R25, https://doi.org/10.1186/gb-2010-11-3-r25 (2010).
Nikolayeva, O. & Robinson, M. D. edgeR for differential RNA-seq and ChIP-seq analysis: an application to stem cell biology. Methods Mol Biol 1150, 45–79, https://doi.org/10.1007/978-1-4939-0512-6_3 (2014).
Storey, J. D. A direct approach to false discovery rates. J Roy Stat Soc B 64, 479–498, https://doi.org/10.1111/1467-9868.00346 (2002).
Kaimal, V., Bardes, E. E., Tabar, S. C., Jegga, A. G. & Aronow, B. J. ToppCluster: a multiple gene list feature analyzer for comparative enrichment clustering and network-based dissection of biological systems. Nucleic Acids Res 38, W96–102, https://doi.org/10.1093/nar/gkq418 (2010).
Acknowledgements
This study was funded by the Bill & Melinda Gates Foundation [OPP 1132910] (AHJ); Perinatal Institute Pilot Grant, Cincinnati Children’s Hospital Medical Center; National Institute of Health [HL122642] (JAW, YX). Presented at the Pediatric Academic Societies Meeting, 05th May 2017, San Francisco, CA. Betamethasone-acetate was a gift from Merck. The funding organizations did not participate in the conceptualization, design, data collection, analysis, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
A.F.S. participated in the conception of the experimental design and animal experiments, analyzed the bioinformatics and the confocal data, P.S.K. performed and analyzed the cortisol assay and performed the immunofluorescence experiments, J.P.B. and A.F. performed the surfactant measurement experiments, D.L. participated in the bioinformatics analysis, M.K. participated in the experimental design and data interpretation, L.A.M. participated in the experiment design, animal experiment planning and data interpretation, S.G.K. participated in the animal experiments and data interpretation, Y.X. and J.A.W. participated in the bioinformatics analyses. A.H.J conceived the idea, participated in the animal experiments and interpretation of the data. A.F.S. wrote the manuscript with support from J.A.W. and A.H.J. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schmidt, A.F., Kannan, P.S., Bridges, J.P. et al. Dosing and formulation of antenatal corticosteroids for fetal lung maturation and gene expression in rhesus macaques. Sci Rep 9, 9039 (2019). https://doi.org/10.1038/s41598-019-45171-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-45171-6
This article is cited by
-
Association of antenatal corticosteroids with mortality and morbidities in very preterm infants born to women with hypertensive disorders of pregnancy: a multicenter prospective cohort study
BMC Pregnancy and Childbirth (2024)
-
A Reduction in Antenatal Steroid Dose Was Associated with Reduced Cardiac Dysfunction in a Sheep Model of Pregnancy
Reproductive Sciences (2023)
-
Which corticosteroid is a better option for antenatal fetal lung maturation?
Pediatric Research (2022)
-
Extremely preterm children exhibit altered cortical thickness in language areas
Scientific Reports (2020)
-
Contemporary Challenges and Developments: Antenatal Corticosteroid Therapy
Current Obstetrics and Gynecology Reports (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
