
Abstract
Oxidative stress has been linked to cancer development in previous studies. However, the association between pre-diagnostic oxidatively generated DNA/RNA damage levels and incident cancer has rarely been investigated. Urinary oxidized guanine/guanosine (OxGua) concentrations, including 8-hydroxy-2′-deoxyguanosine, were assessed in 8,793 older adults in a population-based German cohort. 1,540 incident cancer cases, including 207 lung, 196 colorectal, 218 breast and 245 prostate cancer cases were diagnosed during over 14 years of follow-up. Associations of OxGua levels with cancer outcomes were not observed in the total population in multi-variable adjusted Cox regression models. However, in subgroup analyses, colorectal cancer incidence increased by 8%, 9% and 8% with one standard deviation increase in OxGua levels among current non-smokers, female and non-obese participants, respectively. Additionally, among non-smokers, overall and prostate cancer incidences statistically significantly increased by 5% and 13% per 1 standard deviation increase in OxGua levels, respectively. In contrast, OxGua levels were inversely associated with the risk of prostate cancer among current smokers. However, none of the subgroup analyses had p-values below a threshold for statistical significance after correction for multiple testing. Thus, results need to be validated in further studies. There might be a pattern that oxidatively generated DNA/RNA damage is a weak cancer risk factor in the absence of other strong risk factors, such as smoking, obesity and male sex.
Similar content being viewed by others


Introduction
The term “oxidative stress (OS)” refers to an imbalance in which the production of reactive oxygen species (ROS) overwhelms the capacity of antioxidant defense systems leading to a dysregulation of redox signaling and/or damage to biomolecules1. OS has long been known to be involved in cancer. Excessive levels of ROS may directly react with nucleic acids leading to mitochondrial and nucleus genomic instability, which facilitates carcinogenesis2. ROS may also activate or inhibit downstream signaling pathways promoting cancer development2,3,4,5,6. In addition, OS can contribute to carcinogenesis through epigenetic mechanisms7,8,9,10. For instance, the patterns of DNA methylation can be affected by oxidative DNA damage causing aberrant gene expression9. However, studies with humans on associations of ROS with cancer risk are not possible due to the short half-life of ROS in human specimens. Therefore, OS related biomarkers are needed for epidemiological studies as proxies for the effect of OS on cellular molecules11,12.
The Oxidized guanine/guanosine (OxGua) molecules, including 8-hydroxyguanine (8-OHGua) and its nucleoside forms 8-hydroxy-2′-deoxyguanosine (8-OHdGuo) and 8-hydroxyguanosine (8-OHGuo), have been used as biomarkers to assess the intensity of ROS-induced DNA damage in epidemiological studies. These molecules are formed from the attack of hydroxyl radicals on the guanine of the DNA strand and RNA strand12. Unrepaired DNA lesion can lead to GC → TA transversion mutations. However, the DNA lesion can be corrected by the base excision repair process, which is initiated by 8-oxoguanine glycosylase (OGG1). 8-OHGua is removed by OGG1 and the formed Apurinic/apyrimidinic site can be cleaved by an endonuclease13. The RNA is more vulnerable to oxidative stress due to its single-stranded structure. 8-OHGuo is one of 20 types of RNA damage and might lead to synthesis of anomalous proteins14. Degradation of oxidized RNA stands is mainly performed by ribonucleases14. Ultimately, the OxGua degradation products of oxidatively damaged DNA and RNA are being secreted into urine. The OxGua molecules are very stable in frozen urine samples (shown for up to 15 years of storage15). Therefore, OxGua is a biomarker of OS that can be measured in stored baseline urine samples from studies with long-term follow-up. However, due to inconsistent findings from prospective observational studies, it is unclear whether urinary OxGua levels are associated with cancer risk15,16,17,18,19,20.
In this study, OxGua levels were measured to determine the prospective association with total cancer incidence and the incidences of the most common site-specific cancers (i.e., lung, colorectal, breast and prostate cancer) in a population-based cohort study with 14 years of cancer follow-up.
Methods
Study population
This investigation is based on the ESTHER study (German Name: “Epidemiologische Studie zu Chancen der Verhütung, Früherkennung und optimierten Therapie chronischer Erkrankungen in der älteren Bevölkerung”), an ongoing population-based cohort. The study design has been reported elsewhere in detail21,22. Briefly, the cohort was initiated during 2000 and 2002 in Saarland, a federal state in southwest Germany. At baseline, 9,940 subjects, aged 50–75 years, were recruited by their general practitioners during a general health check-up. In current study, 783 subjects with a history of any cancer except non-melanoma skin cancer were excluded. Furthermore, we excluded 168 individuals with missing urine samples, and 196 study participants for whom urinary OxGua levels could not be measured, resulting in an analytical sample of 8,793 individuals. Analyses on breast and prostate cancer were restricted to females (n = 4,853) and males (n = 3,940) study participants, respectively.
Ethical approval and informed consent
This study was approved by the ethics committees of the University of Heidelberg and the state medical board of Saarland. Personal information and human specimens were collected after obtaining signed and informed written consent from all study participants. The study was conducted in accordance with the Declaration of Helsinki.
Laboratory analyses
At baseline, blood and spot urine samples were collected during the health check-up and shipped to the study center using a temperature-controlled supply chain. After arrival in our lab, we stored the urine samples at −80 °C until further processing. Urinary OxGua concentrations were assessed with the DNA/RNA Oxidative Damage ELISA Kit of Cayman (Ann Arbor, Michigan, USA), which detects all three OxGua species: 8-OHGua from either DNA or RNA, 8-OHdGuo from DNA, and 8-OHGuo from RNA. Accordingly, this assay captures a more complete set of biologically relevant products of oxidatively generated DNA/RNA damage than 8-OHGua specific assays. The dilution factor was 800-fold. Urinary creatinine was determined by the kinetic Jaffe method for renal function adjustment of spot urine samples and OxGua levels are being reported in the unit “μg/g creatinine”. Serum C-reactive protein (CRP) and total cholesterol levels were measured by immunoturbidimetry and an enzymatic colorimetric assay, respectively.
Outcome ascertainment
Up to the end of 2014, all cancers were recorded by linking study participants to the Saarland Cancer Registry. The 10th Revision of the International Statistical Classification of Diseases (ICD-10) was used for coding of the cancer sites. Total cancer incidence included all cancer sites except non-melanoma skin cancers (ICD-10 code C44). Lung, colorectal, breast and prostate cancer were coded as C34, C18-C21, C50 and C61, respectively.
Covariates
Sociodemographic characteristics, lifestyle and dietary factors were collected by a standardized self-administered questionnaire. Self-reported smoking information was confirmed to be reliable in a subgroup of 1,500 study participants with serum cotinine measurements23. Height and weight were measured by general practitioners during the health check-up and documented on a standardized form.
Statistical analyses
Statistical Analysis System (SAS, version 9.4, Cary, North Carolina, USA) was used to perform all statistical analyses. Statistical tests were two-sided using a significance level of 0.05.
Variations in urinary OxGua levels according to established cancer risk factors were assessed by comparing proportions (by Chi-square tests) or medians/means (by Wilcoxon-Mann-Whitney tests) in OxGua level tertiles while using the bottom tertile as the reference.
Cox proportional hazards models were performed to estimate hazard ratios (HRs) with corresponding 95% confidence intervals (95% CIs) to investigate the associations of OxGua levels with the incidence of total cancer and four common cancers. Death is a competing risk of the cancer of interest during the follow-up. Therefore, competing risk of mortality modelling was applied in Cox regression models (except the mortality due to the cancer of interest). The main model, in which OxGua levels were categorized in tertiles as well as modelled linearly, was adjusted for potential confounders, including age, sex, physical activity, body mass index, smoking status, alcohol consumption and dietary factors (fruit, vegetable and red meat consumption). These variables were modelled as displayed in Table 1. In the main analyses, smoking status was modelled in the categories shown in Table 1 and in sensitivity analyses, the continuous variables “current tobacco consumption in grams per day” and “pack-years of smoking” were used. In addition, subgroup analyses with stratification by age (50–64/65–74 years), sex, smoking status (current smoking/non-smoking) and BMI (<30/≥30 kg/m2) were performed. In a further sensitivity analysis cancers diagnosed in the first 2 years of follow-up were excluded to address potential reverse causality bias by early events. Furthermore, in order to correct for multiple testing in subgroup analyses, both the false discovery rate (FDR; using Proc Multtest (SAS 9.4)) and the more conservative Bonferroni method were applied.
No variable had more than 10% of missing values and these missing values were imputed by multiple imputation24. The imputation model consisted of total cholesterol, CRP and the variables of the main model. Five complete data sets were generated by multiple imputation and results of Cox regression were combined by using the MIANALYZE procedure of the SAS software.
Results
Table 1 shows that the mean age of the analyzed study population was 62 years and more females (55.2%) were included than males. Table 2 presents that the OxGua levels were positively, statistically significantly associated with female sex, low education, physical inactivity, and higher CRP levels, whereas a negative direction of the association was observed with alcohol consumption. However, OxGua levels were not associated with age and total cholesterol to a relevant extent, and associations with smoking, BMI and dietary factors were weak or not observed.
During 14 years of follow-up, 1,540 participants were diagnosed with incident cancer, including 207 lung cancers, 196 colorectal cancers, 221 breast cancers and 246 prostate cancers. Table 3 shows the associations of OxGua levels with overall and site-specific cancer incidences in the total population and for the age groups 50–64 years and 65–74 years. No statistically significant associations were observed. In addition, no statistically significant findings were observed in the other subgroup analyses after correcting for multiple testing with either the FDR or Bonferroni correction. In total, we carried out 41 tests for potential associations of OxGua levels and the 5 cancer outcomes in the total population and in subgroup analyses defined by age, sex, smoking and obesity. Therefore, a Bonferroni-corrected p-value < 0.0012 would have been needed for a statistically significant finding. The lowest observed p-value in all analyses was 0.006 (for 1 SD increase in OxGua levels and total cancer incidence in current non-smokers), which is above the Bonferroni corrected p-value for statistical significance. The same result was obtained with FDR correction, which led to a statistically non-significant p-value of 0.162 for the strongest association observed in all analyses.
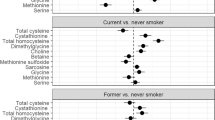
Therefore, the following observed associations with p-values < 0.05 (before correction for multiple testing was performed) are not statistically significant and shall only be regarded to be hypotheses generating. In analyses stratified by sex, an association between OxGua levels and colorectal cancer was observe among women (HR (95% CI) per 1 SD increase: 1.09 (1.02, 1.17)) (Table 4). Stratified by smoking status, a 1 SD increase in OxGua levels was associated with a 5% increase in total cancer incidence (HR (95% CI): 1.05 (1.02, 1.10)), an 8% increase in colorectal cancer (HR (95% CI): 1.08 (1.01, 1.16)) and a 13% increase in prostate cancer incidence (HR (95% CI): 1.13 (1.01, 1.28)) among current non-smokers (Table 5). In current smokers, however, OxGua levels were negatively associated with prostate cancer risk (for comparison of top and bottom tertile) (Table 5). Splitting up the current non-smokers into never and former smokers did not reveal differential results (data not shown). Subgroup analyses in non-obese and obese study participants are shown in Table 6. The only finding was for colorectal cancer among non-obese individuals (HR (95% CI) per 1 SD increase: 1.08 (1.00, 1.16)).
In a sensitivity analysis, modelling smoking with the variables “current average amount of consumed grams of tobacco per day” or “pack-years of smoking” did not change the results (data not shown). In a further sensitivity analysis, no relevant changes of the findings were observed after excluding cancer cases during the first 2 years of follow-up (data not shown).
Discussion
In this large cohort of older adults, OxGua levels were not associated with any cancer outcome in the total population. Although not statistically significant after correction for multiple testing, some potential associations (raw p-values < 0.05) between OxGua levels and cancer incidences were observed in subgroup analyses. Positive associations were observed between OxGua levels and colorectal cancer among current non-smokers, women and non-obese participants. In addition, OxGua levels were positively associated with overall and prostate cancer incidence among current non-smokers. In contrast, OxGua levels were inversely associated with prostate cancer incidence among current smokers.
The OxGua molecules are derived from repair products of the oxidatively generated DNA/RNA lesions12. The formation of OxGua is not organ-specific and its excretion into urine is reflecting the average production in all parts of the body. Therefore, a statistically significant association with total cancer incidence was expected which would suggest that OS-induced genome instability may be involved in the etiology of various types of cancer among25. However, a potential association of OxGua levels and total cancer incidence was only observed among non-smokers. A possible explanation might be that a weak association cannot be detected among current smokers because smoking is a much stronger cancer risk factor than oxidatively generated DNA/RNA damage and overshadows the latter by increasing the absolute cancer risk of smokers leading to very weak relative risks for other risk factors.
This statistical explanation, may also explain the findings for colorectal cancer. Oxidatively generated DNA/RNA damage was only detected as a risk factor for colorectal cancer in the absence of other strong risk factors for this cancer entity, such as smoking, obesity and male sex26.
It is more difficult to explain the different directions of the observed effect estimates for associations of OxGua levels with prostate cancer incidence among current smokers and current non-smokers. OxGua levels were positively associated with prostate cancer incidence in non-smokers and inversely associated with prostate cancer incidence in current smokers. Among current non-smokers, the positive direction of the association can be explained by the fact that OS activates androgen receptor signaling27, which can promote prostate cancer development29. Among current smokers, the protective role of OS in prostate cancer development is unexpected because other observational studies showed that cigarette smoking is a risk factor for prostate cancer and smoking is known to be associated with OS28. The potential mechanism might be the cytotoxicity of OS caused by cigarette smoke in prostate tissue. OS plays an important role in determining cell fate and the effect of OS on cells largely relies on its levels30. Therefore, higher levels of OS of smokers may lead to apoptosis of prostate cancer cells. However, this explanation is a speculation and it should be remembered that the observed protective association could also be a random finding because the association was not statistically significant after correction of multiple testing. Interestingly, another analysis in the ESTHER cohort with 8-isoprostane levels also detected an inverse association of the OS biomarker with prostate cancer among current smokers31. Therefore, this initially unexpected finding deserves further investigations in other studies.
There is no previous prospective epidemiological study that estimated the association of OxGua levels with the risk of colorectal or prostate cancer to which we could compare our results. With respect to breast cancer, while it was observed a borderline statistically significant association of urinary 8-OHdGuo with breast cancer in a general population based on a Danish nested case-control study17, a Chinese population based nested case-control study did not confirm it19.
Our findings are consistent with two Danish nested case-control studies, which did not observe an association of 8-OHGua and 8-OHdGuo levels with lung cancer incidence in the total population15,16. The authors only observed an increased lung cancer incidence rate ratio with increasing 8-OHdG levels in subgroups (men, never smoker and former smoker)15,16. Albeit not statistically significant, our study also observed an increased risk for lung cancer at high OxGua levels only among non-smokers but not smokers.
Strengths include the prospective design, the long term cancer registry based follow-up and the large sample size. Although residual confounding cannot be completely excluded, detailed adjustment for potential confounders limited the extent of confounding as far as possible. In addition, reverse causality bias was unlikely because excluding cancers from the first two years of follow-up did not change the results.
There are also limitations need to be considered when interpreting the results. First, OxGua levels were measured with single measurements because of limited funding. This may have affected the precision of measurements for single study participants but at the population level, the large sample size (n = 8,793) minimized the influence of random measurement errors on the associations with the outcomes. Second, ELISA assays have the general limitation of a lower specificity for the target molecule(s), when compared to mass spectrometry methods. As outlined in detail in the methods section, the chosen ELISAs also measure structurally related molecules, including biologically relevant metabolites. Of course, it would be even better to have distinct measurements of all these metabolites in order to assess their distinct associations with the outcomes (in particular for 8-OHGua from either DNA or RNA, 8-OHGuo from DNA and 8-OHdGuo from RNA), which could differ, as shown previously for DNA and RNA oxidation for mortality and cardiovascular disease risk in diabetes patients32. Future studies are required to target potential differences for DNA and RNA oxidation for cancer outcomes with more specific methods. Third, studies for others ethnicities and younger study participants are needed because our results can only be generalized for older Caucasians.
To conclude, this prospective cohort study observed no association of urinary OxGua levels with lung, colorectal, breast and prostate cancer in the total population. Higher urinary OxGua levels were potentially associated with an increased risk of colorectal cancer only among current non-smokers, women and non-obese participants. Urinary OxGua levels also showed a positive association with overall, prostate cancer incidence among current non-smokers and an inverse association with prostate cancer incidence among current smokers. However, none of these findings from subgroup analyses were statistically significant after correction for multiple testing and further studies are needed to corroborate our findings. However, we are confident that our results can be validated by others because there seemed to be pattern in our study results that oxidatively generated DNA/RNA damage could be a weak cancer risk factor (especially for colorectal cancer) in the absence of other strong risk factors like smoking, obesity and male sex.
Data Availability
Requests for access to the data used for this investigation can be made by inquiry at the corresponding author.
References
Jones, D. P. Redefining oxidative stress. Antioxid Redox Signal 8, 1865–1879 (2006).
Sosa, V. et al. Oxidative stress and cancer: An overview. Ageing Res Rev 12, 376–390 (2013).
Gào, X. & Schöttker, B. Reduction–oxidation pathways involved in cancer development: a systematic review of literature reviews. Oncotarget. 8, e17128 (2017).
Gupta, S. C. et al. Upsides and downsides of reactive oxygen species for cancer: the roles of reactive oxygen species in tumorigenesis, prevention, and therapy. Antioxid Redox Signal. 16, 1295–1322 (2012).
Liou, G. Y. & Storz, P. Reactive oxygen species in cancer. Free Radic Res 44, 479–496 (2010).
Saha, S. K. et al. Correlation between Oxidative Stress, Nutrition, and Cancer Initiation. Int J Mol Sci 18, e1544 (2017).
Afanas’ev, I. New nucleophilic mechanisms of ros-dependent epigenetic modifications: comparison of aging and cancer. Aging Dis 5, 52–62 (2014).
Bhat, A. V., Hora, S., Pal, A., Jha, S. & Taneja, R. Stressing the (epi)genome: dealing with ROS in cancer. Antioxid Redox Signal 29, 1273–1292 (2017).
Franco, R., Schoneveld, O., Georgakilas, A. G. & Panayiotidis, M. I. Oxidative stress, DNA methylation and carcinogenesis. Cancer Lett 266, 6–11 (2008).
Gao, T. et al. DNA methylation of oxidative stress genes and cancer risk in the Normative Aging Study. Am J Cancer Res 6, 553–561 (2016).
Cracowski, J. L., Durand, T. & Bessard, G. Isoprostanes as a biomarker of lipid peroxidation in humans: physiology, pharmacology and clinical implications. Trends Pharmacol Sci 23, 360–366 (2002).
Valavanidis, A., Vlachogianni, T. & Fiotakis, C. 8-hydroxy-2′-deoxyguanosine (8-OHdG): A critical biomarker of oxidative stress and carcinogenesis. J. Environ Sci Health C Environ Carcinog Ecotoxicol Rev 27, 120–139 (2009).
Hill, J. W., Hazra, T. K., Izumi, T. & Mitra, S. Stimulation of human 8-oxoguanine-DNA glycosylase by AP-endonuclease: potential coordination of the initial steps in base excision repair. Nucleic Acids Res 29, 430–438 (2001).
Kong, Q. & Lin, C. L. Oxidative damage to RNA: mechanisms, consequences, and diseases. Cell Mol Life Sci 67, 1817–1829 (2010).
Loft, S. et al. Prospective study of 8-oxo-7,8-dihydro-2′-deoxyguanosine excretion and the risk of lung cancer. Carcinogenesis 27, 1245–1250 (2006).
Loft, S. et al. Association between 8-oxo-7,8-dihydroguanine excretion and risk of lung cancer in a prospective study. Free Radic Biol Med 52, 167–172 (2012).
Loft, S., Olsen, A., Moller, P., Poulsen, H. E. & Tjonneland, A. Association between 8-oxo-7,8-dihydro-2′-deoxyguanosine excretion and risk of postmenopausal breast cancer: nested case-control study. Cancer Epidemiol Biomarkers Prev 22, 1289–1296 (2013).
Chuma, M. et al. 8-Hydroxy-2′-deoxy-guanosine is a risk factor for development of hepatocellular carcinoma in patients with chronic hepatitis C virus infection. J Gastroenterol Hepatol. 23, 1431–1436 (2008).
Lee, K. H. et al. Breast cancer and urinary biomarkers of polycyclic aromatic hydrocarbon and oxidative stress in the Shanghai Women’s Health Study. Cancer Epidemiol Biomarkers Prev 19, 877–883 (2010).
Tanaka, H. et al. Hepatic oxidative DNA damage is associated with increased risk for hepatocellular carcinoma in chronic hepatitis C. Br J Cancer 98, 580–586 (2008).
Löw, M., Stegmaier, C., Ziegler, H., Rothenbacher, D. & Brenner, H. Epidemiological investigations of the chances of preventing, recognizing early and optimally treating chronic diseases in an elderly population (ESTHER study). Dtsch Med Wochenschr 129, 2643–2647 (2004).
Schöttker, B. et al. Strong associations of 25-hydroxyvitamin D concentrations with all-cause, cardiovascular, cancer, and respiratory disease mortality in a large cohort study. Am J Clin Nutr 97, 782–793 (2013).
Zhang, Y. et al. Self-reported smoking, serum cotinine, and blood DNA methylation. Environ Res 146, 395–403 (2016).
Schafer, J. L. Analysis of incomplete multivariate data. (NY: Chapman and Hall, 1997).
Hanahan, D. & Weinberg, R. A. Hallmarks of cancer: the next generation. Cell 144, 646–674 (2011).
Brenner, H., Kloor, M. & Pox, C. P. Colorectal cancer. Lancet 383, 1490–1502 (2014).
Shiota, M., Yokomizo, A. & Naito, S. Oxidative stress and androgen receptor signaling in the development and progression of castration-resistant prostate cancer. Free Radic Biol Med 51, 1320–1328 (2011).
Huncharek, M., Haddock, K. S., Reid, R. & Kupelnick, B. Smoking as a Risk Factor for Prostate Cancer: A Meta-Analysis of 24 Prospective Cohort Studies. Am J Public Health 100, 693–701 (2010).
Culig, Z. & Santer, F. R. Androgen receptor signaling in prostate cancer. Cancer Metastasis Rev 33, 413–427 (2014).
Matés, J. M., Segura, J. A., Alonso, F. J. & Márquez, J. Oxidative stress in apoptosis and cancer: an update. Arch Toxicol 86, 1649–1665 (2014).
Gào, X. et al. Urinary 8-isoprostane levels and occurrence of lung, colorectal, prostate, breast and overall cancer: Results from a large, population-based cohort study with 14 years of follow-up. Free Radic Biol Med 123, 20–26 (2018).
Broedbaek, K. et al. Long-term effects of Irbesartan treatment and smoking on nucleic acid oxidation in patients with type 2 diabetes and microalbuminuria: an Irbesartan in patients with type 2 diabetes and Microalbuminuria (IRMA 2) substudy. Diabetes Care 34, 1192–1198 (2011).
Acknowledgements
Funds for this investigation were obtained by a grant from the German Research Foundation (DFG, Grant No. SCHO 1545/3-1) and by a scholarship given by the China Scholarship Council to Xīn Gào (Grant No. 201506010268). The ESTHER study was funded by the Baden-Württemberg state Ministry of Science, Research and Arts, the Federal Ministry of Education and Research of Germany, the Saarland state Ministry for Social Affairs, Health, Women and Family Affairs, and the Federal Ministry of Family Affairs, Senior Citizens, Women and Youth of Germany.
Author information
Authors and Affiliations
Contributions
X.G. and B.S. designed the research; H.B. developed the ESTHER study and supervised the data collection; B.H. conducted data collection from the Saarland Cancer Registry. X.G., K.C. and Y. Xu conducted to lab analyses. X.G. analyzed the data and drafted the manuscript, B.S. revised it; B.H., K.C., Y.Z., A.A., Y. Xuan, Y. Xu. and H.B. contributed important intellectual content to the discussion. All authors were involved in the interpretation and discussion of results.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gào, X., Holleczek, B., Cuk, K. et al. Investigation on potential associations of oxidatively generated DNA/RNA damage with lung, colorectal, breast, prostate and total cancer incidence. Sci Rep 9, 7109 (2019). https://doi.org/10.1038/s41598-019-42596-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-42596-x
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
