
Abstract
Raised circulating concentrations of asymmetric dimethylarginine (ADMA), an endogenous inhibitor of nitric oxide synthase (NOS), have been reported in several rheumatic diseases (RDs). However, the strength of this relationship is unclear. Therefore, the aim of this systematic review and meta-analysis was to evaluate the magnitude and the robustness of the association between ADMA concentrations and RDs. We calculated standardized mean differences (SMD, with 95% confidence intervals, CI). Study heterogeneity was evaluated by meta-regressions and sensitivity analyses according to type of RDs, conventional cardiovascular risk factors, inflammatory markers, and type of ADMA assessment methodology. Thirty-seven studies with a total of 2,982 subjects (1,860 RDs patients and 1,122 healthy controls) were included in our meta-analysis. Pooled results showed that ADMA concentrations were significantly higher in patients with RDs than in healthy controls (SMD = 1.27 µmol/L, 95% CI 0.94–1.60 µmol/L; p < 0.001). However, the between-studies heterogeneity was high. Differences in ADMA concentrations between controls and RDs patients were not significantly associated with inflammatory markers, increasing age, lipid concentrations, body mass index, blood pressure, or methodology used to assess ADMA. Furthermore, subgroup analysis showed no difference across RDs. This meta-analysis showed that, in the context of significant between-study heterogeneity, circulating concentrations of ADMA are positively related to RDs.
Similar content being viewed by others

Introduction
The term “systemic rheumatic diseases” (RDs) encompasses a broad spectrum of chronic inflammatory disorders of joints and internal organs that are characterized by tissue destruction, disability and increased cardiovascular and all-cause mortality. The dysregulation of innate and adaptive immunologic response, with overproduction of pro-inflammatory cytokines, represents the pathogenic hallmark of RDs1.
Compared with the general population, patients with RDs suffer from a significantly reduced life expectancy that is mainly due to atherosclerotic cardiovascular disease2,3. This excess of cardiovascular mortality, only partially predicted by conventional risk factors, has been linked to early endothelial dysfunction and accelerated arterial stiffening2,3,4. In fact, peripheral and central endothelial dysfunction, a measure of nitric-oxide (NO) availability and vasodilatory function, has been shown to be more prevalent in RDs than in the general population5,6,7.
A strong body of clinical and experimental evidence collected in the last decade has convincingly supported a potential pathogenetic role for the accumulation of asymmetric dimethylarginine (ADMA), an endogenous inhibitor of NO-synthase8, in the occurrence and progression of endothelial dysfunction, arterial stiffening, and atherosclerotic cardiovascular disease9. Moreover, studies in healthy subjects and different patient groups have confirmed the independent prognostic role of basal plasma ADMA concentrations on cardiovascular and all-cause mortality10,11,12. Therefore, raised circulating ADMA concentrations might be a surrogate measure of endothelial dysfunction, early atherosclerosis and increased risk of future cardiovascular events.
Increased circulating ADMA concentrations, initially reported in rheumatoid arthritis (RA) patients free of cardiovascular risk13, have also been observed in psoriatic arthritis (PsA)14,15, ankylosing spondylitis (AS)16,17,18,19,20, systemic lupus erythematosus (SLE)21, Sjogren’s syndrome (SSj)22, systemic sclerosis (SSc)23,24,25,26,27,28,29 and Behçet’s disease (BD)30,31,32,33,34.
However, despite being largely investigated, the association between ADMA concentrations and RDs has generally been studied in populations with relatively small sample size. Therefore, we performed a meta-analysis of all relevant studies to define the magnitude and the robustness of the relationship between ADMA concentrations and RDs.
Materials and Methods
Search strategy, eligibility criteria, and study selection
A systematic search of publications in the PubMed, Web of Science and Scopus databases, from inception to March 2018, was performed using the following keywords and terms, and their combination: ‘ADMA AND (rheumatic diseases OR rheumatoid arthritis OR psoriatic arthritis OR ankylosing spondylitis OR systemic lupus erythematosus OR systemic sclerosis OR Sjogren’s syndrome OR connective tissue diseases OR vasculitis OR Behçet’s disease)’. In addition, references of the filtered studies were manually checked for potentially missing eligible studies. Two researchers (GLE and AZ) independently screened the abstracts and reviewed the full articles; disagreement between the investigators, when present, was resolved by a third researcher (PP). Inclusion criteria were: (i) assessment of ADMA, (ii) only adult participants, (iii) comparison of healthy subjects with patients with RDs (case-control design), (iv) English language and (vi) full-text publications.
A pre-established protocol, including methods for the analysis, was followed: in particular, we investigated the difference in ADMA concentrations stratifying for the following subgroups (i) RD subtype (e.g. RA vs SSc vs PsA, etc.) (ii) connective tissue diseases (CTD) vs non-CTD, (iii) autoimmune conditions (SLE, RA, SSc and SSj) vs conditions with mixed (autoimmune and inflammatory) features (PsA, AS) and autoinflammatory conditions (BD and Familial Mediterranean Fever, FMF), (iv) biological sample (serum vs plasma) and (v) type of laboratory test (e.g. liquid chromatography-LC vs ELISA).
Where available, we extracted demographic, anthropometric, clinical and laboratory data from the selected articles and presented them in table format.
Quality of studies was assessed with the Newcastle–Ottawa Scale (NOS)35. Meta-regression analysis was carried out to investigate potentially influencing factors on ADMA% difference.
Statistical analysis
Standardized mean differences (SMD) were used to create forest plots of continuous data and to assess differences in ADMA concentrations between healthy controls and patients with RDs. A p < 0.05 was considered statistically significant, and 95% confidence intervals (CIs) were reported. In two studies22,23 the mean and standard deviation were inferred from median and IQR as previously reported36, while in two further studies30,37 the mean and standard deviation were inferred from median and range as previously reported by Hozo et al.38.
Heterogeneity of SMD across studies was tested with the Q statistic (significance level at p < 0.10). The I2 statistic was also calculated (I2 < 25%, no heterogeneity; I2 between 25% and 50%, moderate heterogeneity; I2 between 50% and 75%, large heterogeneity; and I2 > 75%, extreme heterogeneity)39,40. Statistical heterogeneity was defined as an I2 statistic value ≥ 50% (38). In analyses in which heterogeneity was high, a random-effects model was used.
The influence of each single study on effect size was evaluated by sequentially excluding one study at the time, through sensitivity analysis. Publication bias was assessed by means of Begg’s adjusted rank correlation test and Egger’s regression asymmetry test at the p < 0.05 level of significance41,42. Duval and Tweedie “trim and fill” procedure was performed to identify and correct for funnel plot asymmetry resulting from publication bias43. The aim of this method is to remove (trim) smaller studies responsible for funnel plot asymmetry, use the trimmed funnel plot to evaluate the true centre of the funnel, then replacing the omitted studies with the new calculated “missing” studies around the centre (filling). This allows to estimate the number of missing studies and recalculates the effect size including the filled studies. Statistical analysis was carried out using MedCalc for Windows, version 15.4 64 bit (MedCalc Software, Ostend, Belgium) and Stata 14 (STATA Corp., College Station, TX, USA)
This meta-analysis was performed according to PRISMA statements.
Results
Literature Search and Study Selection
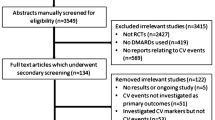
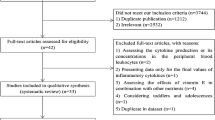
A flowchart summarizing the screening process is described in Fig. 1. We initially detected 309 potentially relevant studies (PubMed n = 85, Scopus n = 84 and WOS n = 140). Two hundred and twenty eight studies were excluded after the initial screening because they were either duplicates (n = 146), irrelevant (n = 81) or not available in full text (n = 1).

Flowchart of study selection.
After a full-text review of 81 articles, 44 were rejected because they did not meet the inclusion criteria. Thus, 37 studies were included in the meta-analysis13,14,15,16,17,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,37,44,45,46,47,48,49,50,51,52,53,54,55,56,57. The characteristics of these studies, published between 2006 and 2018, are summarized in Table 1.
ADMA and RDs
A total of 1,860 RDs patients (41% males) and 1,122 healthy controls (34% males) were evaluated. Overall, the mean age of participants across all studies was 44.6 years both in RDs patients and in controls (Tables 1 and 2).
The forest plot for ADMA concentrations in RDs patients and controls is shown in Fig. 2. Due to the extreme heterogeneity between studies (I2 = 93.2%, p < 0.001), random-effects models were used to perform the analysis. Pooled results showed that ADMA concentrations were significantly higher in patients with RDs (SMD = 1.27 µmol/L, 95% CI 0.94–1.60 µmol/L; p < 0.001).

The pooled standard mean difference (SMD) for asymmetric dimethylarginine (ADMA) concentrations with 95% confidence intervals for eligible studies.
Sensitivity analysis showed that the effect size was not modified when any single study was in turn removed (effect size ranged between 1.17 µmol/L and 1.33 µmol/L, Fig. 3).

Sensitivity analysis of studies examining asymmetric dimethylarginine (ADMA) concentrations in rheumatic diseases (RDs).
Since the Begg’s (p < 0.001) and Egger’s tests (p < 0.001) evidenced a significant publication bias, we applied the trim-and-fill method to correct the results. Twelve potential missing studies were added on the left side of the funnel plot to ensure symmetry (Fig. 4). The adjusted SMD was decreased, but remained significant (0.51 µmol/L, 95% CI 0.15–0.88 µmol/L, p = 0.006).

Funnel plot of eligible studies on dimethylarginine (ADMA) concentrations in rheumatic diseases (RDs).
To explore possible sources of heterogeneity, we investigated differences in SMD across RDs (Table 2). Extreme heterogeneity was observed in all disease types (Table 2). RA, SSc and AS but not BD, FMF, and PsA patients showed significantly higher SMD when compared to healthy controls. However, no significant differences in SMD values were observed between different disease types by meta-regression analysis (p > 0.05).
Moreover, the SMD values in studies of participants with connective tissue diseases (CTD) (1.95 µmol/L, 95% CI 1.02–2.88 µmol/L, p < 0.0001; I2 = 96.0%, p < 0.0001) were higher than that in participants with no-CTD disease (1.10 µmol/L, 95% CI 0.76–1.44 µmol/L, p < 0.0001; I2 = 91.9%, p < 0.0001) although the difference was not significant by meta-regression analysis (t = −1.40, p = 0.17, Fig. 5). Classification of RDs according to CTD phenotype did not influence heterogeneity across studies.

Forest plot depicting the standard mean (SMD) of dimethylarginine (ADMA) concentrations in connective tissue (CTD) vs no-CTD rheumatic diseases. CTD: Systemic lupus erythematosus (SLE), Systemic sclerosis (SS), Rheumatoid arthritis (RA), Sjogren’s syndrome (SSj).
As reported in in Fig. 6, there was no significant difference in SMD values in RDs patients affected by pure autoimmune diseases (1.53 µmol/L, CI 1.08, 1.98 µmol/L, p < 0.0001; I2 = 93.1%, p < 0.0001) when compared with RDs patients with mixed (autoimmune and autoinflammatory) diseases (1.02 µmol/L, CI 0.43, 1.60 µmol/L, p = 0.006; I2 = 94.1%, p = 0.0001) or with autoinflammatory diseases (0.77 µmol/L, CI −0.73, 2.27 µmol/L, p = 0.317; I2 = 95.6%, p < 0.0001). Similarly, heterogeneity was not influenced by disease sub-groups.

Forest plot depicting the standard mean (SMD) of dimethylarginine (ADMA) concentrations in autoimmune (Systemic lupus erythematosus-SLE, Systemic sclerosis-SS, Rheumatoid arthritis-RA, and Sjogren’s syndrome-SSj) vs mixed autoimmune-autoinflammatory (Behcet’s disease-BD, psoriatic arthritis-PsA, and ankylosing spondylitis-AS) vs autoinflammatory (Familial Mediterranean fever (FMF).
We then investigated C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), systolic blood pressure (SBP), diastolic blood pressure (DBP), lipid concentrations, body mass index (BMI), age, sex, and disease duration (DD) as possible contributors to between-study variance. However, none of these variables was found significantly related to pooled SMD by meta-regression analysis [CRP (t = 0.72, p = 0.477), ESR (t = 0.73, p = 0.475), SBP (t = 0.63, p = 0.537), DBP (t = 1.11, p = 0.29), DD (t = 0.93, p = 0.362), total cholesterol (t = −1.71, p = 0.105), LDL (t = −1.05, p = 0.305), HDL (t = −1.56, p = 0.138), TG (t = 0.86, p = 0.399), BMI (t = −0.02, p = 0.981), age (t = 1.47, p = 0.152) and sex (t = −0.19, p = 0.850)].
Finally, we considered whether methodological factors, as biological sample type (serum vs plasma) or detection method (LC vs ELISA) may contribute to heterogeneity. The SMD from studies measuring ADMA in plasma (1.78 µmol/L, 95% CI 0.93–1.60 µmol/L, p < 0.0001; I2 = 94.3%, p < 0.0001) was higher than that in studies measuring ADMA in serum (0.98 µmol/L, 95% CI 0.59–1.37 µmol/L, p < 0.0001; I2 = 92.6%, p < 0.0001, Fig. 7), but the difference was not statistically significant (t = −1.53, p = 0.135).

Forest plots depicting the standard mean (SMD) of dimethylarginine (ADMA) concentrations in rheumatic diseases (RDs) according to the biological matrix tested (serum vs plasma).
Furthermore, the SMD from studies measuring ADMA by LC was higher (1.66 µmol/L, 95% CI 0.99–2.33 µmol/L, p < 0.0001; I2 = 95.1%, p < 0.0001) than that of studies measuring ADMA by ELISA (1.09 µmol/L, 95% CI 0.71–1.47 µmol/L, p < 0.0001; I2 = 92.3%, p < 0.0001, Fig. 8) without a statistically significant difference (t = 1.06, p = 0.296). Heterogeneity in sub-groups was extremely high.

Forest plots depicting the standard mean (SMD) of dimethylarginine (ADMA) concentrations in rheumatic diseases (RDs) according to analytical techniques (liquid chromatography-LC vs ELISA).
Discussion
Besides their effect on the vascular tone, high circulating concentrations of ADMA have been reported to promote oxidative stress58 vascular inflammation59 and smooth muscle cell proliferation60,61. Therefore, ADMA is a candidate pathogenetic factor for oxidative stress-related endothelial dysfunction, accelerated atherosclerosis and vascular remodelling process62 occurring in RDs.
However, the results of studies reporting the association between ADMA and RDs have been contradictory: although most studies demonstrated a significant association between ADMA and RDs13,14,16,17,19,20,21,22,23,24,26,28,29,31,32,33,34,44,45,46,47,48,49,50,52,53,54,55,56,63, other studies failed to report a significant relationship15,18,25,27,30,37,57. The different results might be at least partially explained by the small sample size of each study.
Therefore, we performed a systematic review and meta-analysis to evaluate the strength of the association between circulating ADMA concentrations and RDs. Our analysis, including data from 37 studies with a total of 2,982 subjects, suggested that RDs are associated with significantly higher concentrations of circulating ADMA.
However, we found substantial heterogeneity in studies estimating ADMA in RDs; Therefore, to explore in detail any potential sources of heterogeneity we presented data on a wide range of subgroups based on rheumatic disease phenotype and methodological aspects (Figs 5–8).
First, according to a pre-defined protocol, a subgroup analysis according to type of RDs was performed to identify the source of heterogeneity: other than expected, inclusion in the meta-analysis of different RDs did not account for the large heterogeneity reported in the pooled analysis; Even if SMD was higher in studies including RA, SSc and AS than in studies including BD, FMF and PsA (Table 2) this difference was not statistically significant across studies by meta-regression analysis.
We were also interested to understand whether specific pathogenetic and clinical features of RDs were associated with significant between studies heterogeneity. Therefore, according to pre-specified sub-group analyses, we stratified RDs in CTD vs no-CTD. However, this classification of RDs was not able to explain the large heterogeneity observed in the pooled analysis.
Moreover, according to Mc Goonagle et al.64, we stratified RDs in autoimmune diseases (e.g RA, SLE, and SSc), diseases with mixed autoimmune and autoinflammatory features (e.g, diseases associated with HLA-B27 and other MHC class I epitopes, such as AS, PsA and BD65,66) and autoinflammatory diseases (e.g FMF). However, the difference in autoimmune vs autoinflammatory features did not account for the observed heterogeneity.
A significant association between raised circulating ADMA concentrations and traditional atherosclerotic risk factors (hypercholesterolemia, hypertriglyceridemia, and hypertension) have been reported67,68,69 suggesting that ADMA is causally involved in the pathophysiology of atherosclerosis.
Interestingly, in our study, cardiovascular risk factors did not modify the ADMA SMD. These results question the currently accepted hypothesis that raised circulating ADMA concentrations, a potential measure of the presence of co-existing cardiovascular risk factors, may be associated with increased morbidity and mortality for cardiovascular events in RDs. Therefore, prospective studies with larger sample sizes are warranted to further define the significance of the relationship between ADMA and conventional atherosclerotic risk factor and the independent role of ADMA in the development of atherosclerotic disease in RDs.
Biomarkers of systemic inflammatory burden (such as CRP and ESR) have been shown to be correlated to circulating ADMA concentrations in the general population and in RDs17,59,70. However, in our meta-analyses, we found no significant association between ESR, CRP, disease duration and ADMA concentrations: the cross-sectional design and the small sample size of studies included in this meta-analysis may partly explain this finding.
We also performed two additional pre-specified meta-analyses to evaluate between-group differences according to the analytical techniques used and the biological matrix tested as a potential source of heterogeneity.
To date, preferred methods for the determination of plasma and serum ADMA concentrations are LC and ELISA. However, it is still a matter of debate whether these two methods are comparable to each other71,72,73. A recent meta-analysis reported plasma ADMA concentrations in healthy subjects ranging from 0.34 to 1.10 μmol/l73. On the contrary, normal serum ADMA concentrations in healthy subjects are less well defined: a recent study reported a range of normality of serum ADMA concentrations of 0.43–0.96 μmol/74.
In our subgroup meta-analysis, we found no difference in ADMA SMD on the basis of the analytic method employed or biological matrix tested, suggesting that the large heterogeneity between studies is not explained by techniques variability. However, as reported in Table 1, the range of mean plasma and serum ADMA concentrations in CTRLs was extremely large (from 0.10 to 3.22 μmol/L) with reported mean values not falling within the expected range in a large number of studies30,33,34,37,52,57,75. We think that this finding might be related to variability in the selection of healthy controls, pre-analytical and analytical issues, potentially accounting for the large heterogeneity of pooled estimates in this meta-analysis.
Finally, we explored the substantial heterogeneity of pooled analysis by evaluating whether specific studies might influence the final results. After excluding each study in turn, the significance of SMD remained stable in every meta-analysis.
Moreover, according to Begg’s method and Egger’s test, our meta-analyses carry a significant publication bias. Thus, the trim and fill method was used to adjust for funnel plot asymmetry: in particular, 12 studies were added to balance the funnel plot. The adjusted SMD, even if decreased, remained significant. This indicated that publication bias did not affect the result of the meta-analysis.
This meta-analysis has some limitations; First, substantial heterogeneity of the included studies might decrease the significance of the results. Second, we only searched for studies written in English, an aspect that may have introduced publication bias. Third, most of the articles did not report the type of anti-inflammatory or anti-rheumatic drugs used and their effects on outcome. This last aspect is of both clinical and experimental relevance, considering that some prospective studies have reported a positive effect in reducing ADMA concentrations of immunosuppressive therapies76,77.
Strengths of this systematic review and meta-analysis on the topic of ADMA in RDs, performed on a relatively large and representative population, include the evaluation of ADMA in different disease phenotypes within the ‘rheumatic diseases’ umbrella and extensive analysis of the source of heterogeneity including pathogenetic and clinical features of RDs, analytical techniques and biological matrixes.
Moreover, this meta-analysis provided an estimated ‘effect size’ target of 1.27 umol/L for future interventional studies aiming at reducing ADMA in the population of patients with RDs.
Conclusions
In summary, results from this meta-analysis show a significant positive association between elevated circulating ADMA concentrations and RDs.
The relatively high heterogeneity of the studies included in the meta-analysis, albeit extensively investigated with a number of additional analyses focused on clinical and demographic characteristics, analytical techniques, biological matrixes, and specific studies, requires further research to confirm, or refute, our findings.
Data Availability
All data generated or analysed during this study are included in this published article.
References
Smolen, J. S., Aletaha, D. & McInnes, I. B. Rheumatoid arthritis. Lancet 388, 2023–2038 (2016).
Lee, K. S., Kronbichler, A., Eisenhut, M., Lee, K. H. & Shin, J. I. Cardiovascular involvement in systemic rheumatic diseases: An integrated view for the treating physicians. Autoimmun Rev 17, 201–214 (2018).
O’Sullivan, M., Bruce, I. N. & Symmons, D. P. M. Cardiovascular risk and its modification in patients with connective tissue diseases. Best Practice & Research Clinical Rheumatology 30, 81–94 (2016).
Prasad, M. et al. Cardiorheumatology: cardiac involvement in systemic rheumatic disease. Nat Rev Cardiol 12, 168–176 (2015).
Erre, G. L. et al. Prevalence and Determinants of Peripheral Microvascular Endothelial Dysfunction in Rheumatoid Arthritis Patients: A Multicenter Cross-Sectional Study. Mediators Inflamm. 2018, 6548715 (2018).
Murdaca, G. et al. Endothelial dysfunction in rheumatic autoimmune diseases. Atherosclerosis 224, 309–317 (2012).
Erre, G. L. et al. Coronary flow reserve in systemic rheumatic diseases: a systematic review and meta-analysis. Rheumatol. Int., https://doi.org/10.1007/s00296-018-4039-8 (2018).
Vallance, P., Leone, A., Calver, A., Collier, J. & Moncada, S. Accumulation of an endogenous inhibitor of nitric oxide synthesis in chronic renal failure. Lancet 339, 572–575 (1992).
Mangoni, A. A. The emerging role of symmetric dimethylarginine in vascular disease. Adv Clin Chem 48, 73–94 (2009).
Maas, R. et al. Asymmetric dimethylarginine, smoking, and risk of coronary heart disease in apparently healthy men: prospective analysis from the population-based Monitoring of Trends and Determinants in Cardiovascular Disease/Kooperative Gesundheitsforschung in der Region Augsburg study and experimental data. Clin. Chem. 53, 693–701 (2007).
Zoccali, C. et al. Plasma concentration of asymmetrical dimethylarginine and mortality in patients with end-stage renal disease: a prospective study. Lancet 358, 2113–2117 (2001).
Zhou, S. et al. Asymmetric dimethylarginine and all-cause mortality: a systematic review and meta-analysis. Sci Rep 7, 44692 (2017).
Surdacki, A. et al. Elevated plasma asymmetric dimethyl-L-arginine levels are linked to endothelial progenitor cell depletion and carotid atherosclerosis in rheumatoid arthritis. Arthritis Rheum. 56, 809–819 (2007).
Atzeni, F. et al. Coronary flow reserve and asymmetric dimethylarginine levels: new measurements for identifying subclinical atherosclerosis in patients with psoriatic arthritis. J. Rheumatol. 38, 1661–1664 (2011).
Yilmazer, B., Sahin, T., Unlu, B. Ö., Kir, H. M. & Cefle, A. Investigation of subclinical atherosclerosis in psoriatic arthritis patients with minimal disease activity. Rheumatol. Int. 35, 1385–1392 (2015).
Sari, I. et al. Increased levels of asymmetric dimethylarginine (ADMA) in patients with ankylosing spondylitis. Intern. Med. 48, 1363–1368 (2009).
Erre, G. L. et al. Plasma asymmetric dimethylarginine (ADMA) levels and atherosclerotic disease in ankylosing spondylitis: a cross-sectional study. Clinical rheumatology 30, 21–27 (2011).
Korkosz, M. et al. Disparate effects of anti-TNF-α therapies on measures of disease activity and mediators of endothelial damage in ankylosing spondylitis. Pharmacol Rep 65, 891–897 (2013).
Berg, I. J. et al. Disease activity in ankylosing spondylitis and associations to markers of vascular pathology and traditional cardiovascular disease risk factors: a cross-sectional study. J. Rheumatol. 42, 645–653 (2015).
Inci, U., Yildiz, A., Batmaz, I. & Tekbas, E. Assessment of serum asymmetric dimethylarginine levels and left ventricular diastolic function in patients with ankylosing spondylitis. Int J Rheum Dis 20, 238–244 (2017).
Saadany, H. E. et al. Biochemical and genetic risk factors for atherosclerosis in systemic lupus erythematosus. The Egyptian Rheumatologist 33, 35–43 (2011).
Atzeni, F. et al. New parameters for identifying subclinical atherosclerosis in patients with primary Sjögren’s syndrome: a pilot study. Clin. Exp. Rheumatol. 32, 361–368 (2014).
Turiel, M. et al. Silent cardiovascular involvement in patients with diffuse systemic sclerosis: a controlled cross-sectional study. Arthritis Care Res (Hoboken) 65, 274–280 (2013).
Dooley, A. et al. Abnormal nitric oxide metabolism in systemic sclerosis: increased levels of nitrated proteins and asymmetric dimethylarginine. Rheumatology (Oxford) 45, 676–684 (2006).
Wipff, J. et al. Disturbed angiogenesis in systemic sclerosis: high levels of soluble endoglin. Rheumatology (Oxford) 47, 972–975 (2008).
Blaise, S. et al. Correlation of biomarkers of endothelium dysfunction and matrix remodeling in patients with systemic sclerosis. J. Rheumatol. 36, 984–988 (2009).
Ciurzyński, M. et al. Serum endothelin-1 and NT-proBNP, but not ADMA, endoglin and TIMP-1 levels, reflect impaired right ventricular function in patients with systemic sclerosis. Clin. Rheumatol. 33, 83–89 (2014).
Silva, I. et al. Predictive value of vascular disease biomarkers for digital ulcers in systemic sclerosis patients. Clin. Exp. Rheumatol. 33, S127–130 (2015).
Dimitroulas, T. et al. Early detection of cardiac involvement in systemic sclerosis assessed by tissue-Doppler echocardiography: relationship with neurohormonal activation and endothelial dysfunction. J. Rheumatol. 37, 993–999 (2010).
Ozturk, B., Vatansev, H. & Taner, A. Asymmetric dimethylarginine levels in Behçet’s disease - Google Scholar. Turk J Biochem 39, 362–7 (2014).
Sahin, M. et al. Asymmetric dimethylarginine and nitric oxide levels as signs of endothelial dysfunction in Behcet’s disease. Ann. Clin. Lab. Sci. 36, 449–454 (2006).
Aydin, M. et al. Serum nitric oxide, asymmetric dimethylarginine, and plasma homocysteine levels in active Behçet’s disease. Turk J Med Sci 42, 1194–1199 (2012).
Ozuguz, P. et al. Markers of endothelial dysfunction and evaluation of vascular reactivity tests in Behçet disease. Angiology 65, 937–943 (2014).
Yuksel, M. et al. Novel markers of endothelial dysfunction and inflammation in Behçet’s disease patients with ocular involvement: epicardial fat thickness, carotid intima media thickness, serum ADMA level, and neutrophil-to-lymphocyte ratio. Clin. Rheumatol. 35, 701–708 (2016).
Ottawa Hospital Research Institute. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (Accessed: 16th February 2018).
Wan, X., Wang, W., Liu, J. & Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 14, 135 (2014).
Pamuk, B. O., Sari, I., Selcuk, S., Gokce, G. & Kozaci, D. L. Evaluation of circulating endothelial biomarkers in familial Mediterranean fever. Rheumatol. Int. 33, 1967–1972 (2013).
Hozo, S. P., Djulbegovic, B. & Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5, 13 (2005).
Bowden, J., Tierney, J. F., Copas, A. J. & Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med Res Methodol 11, 41 (2011).
Higgins, J. P. T. & Thompson, S. G. Quantifying heterogeneity in a meta-analysis. Stat Med 21, 1539–1558 (2002).
Begg, C. B. & Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 50, 1088–1101 (1994).
Sterne, J. A. & Egger, M. Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J Clin Epidemiol 54, 1046–1055 (2001).
Duval, S. & Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 56, 455–463 (2000).
Radhakutty, A. et al. Opposing effects of rheumatoid arthritis and low dose prednisolone on arginine metabolomics. Atherosclerosis 266, 190–195 (2017).
Terekeci, H. M. et al. Increased asymmetric dimethylarginine levels in young men with familial Mediterranean fever (FMF): is it early evidence of interaction between inflammation and endothelial dysfunction in FMF? J. Rheumatol. 35, 2024–2029 (2008).
Turiel, M. et al. Non-invasive assessment of coronary flow reserve and ADMA levels: a case-control study of early rheumatoid arthritis patients. Rheumatology (Oxford) 48, 834–839 (2009).
Topal, G. et al. Asymmetric dimethylarginine (ADMA) levels are increased in patients with fibromyalgia: correlation with tumor necrosis factor-α (TNF-α) and 8-iso-prostaglandin F(2α) (8-iso-PGF(2α)). Clin. Biochem. 44, 364–367 (2011).
Karaoğlan, B. et al. Romatoid Artritli Hastalarda ADMA Düzeyleri ile Karotid Arter Intima-Media Kalınlığı Arasındaki İlişkinin Saptanması. Türkiye Fiziksel Tıp ve Rehabilitasyon Dergisi 57, 114–118 (2011).
Di Franco, M. et al. Serum levels of asymmetric dimethylarginine and apelin as potential markers of vascular endothelial dysfunction in early rheumatoid arthritis. Mediators Inflamm. 2012, 347268 (2012).
Kwaśny-Krochin, B., Głuszko, P. & Undas, A. Plasma asymmetric dimethylarginine in active rheumatoid arthritis: links with oxidative stress and inflammation. Pol. Arch. Med. Wewn. 122, 270–276 (2012).
Sandoo, A. et al. Clinical remission following treatment with tumour necrosis factor-alpha antagonists is not accompanied by changes in asymmetric dimethylarginine in patients with rheumatoid arthritis. Clin. Biochem. 45, 1399–1403 (2012).
Vatansev, H. et al. Asymmetric dimethylarginine and arginine levels in patients with rheumatoid arthritis. Turkish Journal of Biochemistry 38, 169–175 (2013).
Klimek, E. et al. Differential associations of inflammatory and endothelial biomarkers with disease activity in rheumatoid arthritis of short duration. Mediators Inflamm. 2014, 681635 (2014).
Akgol, G. et al. Can serum asymmetric dimethyl-arginine and homocysteine levels be a new activity parameter of disease in patients with rheumatoid arthritis? Int J Clin Exp Med 9, 14586–14595 (2016).
Erre, G. L. et al. Asymmetric dimethylarginine and arterial stiffness in patients with rheumatoid arthritis: A case-control study. J Int Med Res 44, 76–80 (2016).
Şentürk, T., Yılmaz, N., Sargın, G., Köseoğlu, K. & Yenisey, Ç. Relationship between asymmetric dimethylarginine and endothelial dysfunction in patients with rheumatoid arthritis. Eur J Rheumatol 3, 106–108 (2016).
Ozalper, V. et al. Evaluation of endothelial dysfunction in patients with familial Mediterranean fever: the relationship between the levels of asymmetric dimethylarginine and endocan with carotid intima-media thickness and endothelium-dependent vasodilation. Clin. Rheumatol. 36, 2071–2077 (2017).
Karbach, S., Wenzel, P., Waisman, A., Munzel, T. & Daiber, A. eNOS uncoupling in cardiovascular diseases–the role of oxidative stress and inflammation. Curr. Pharm. Des. 20, 3579–3594 (2014).
Antoniades, C. et al. Role of asymmetrical dimethylarginine in inflammation-induced endothelial dysfunction in human atherosclerosis. Hypertension 58, 93–98 (2011).
Pekarova, M. et al. Asymmetric dimethyl arginine induces pulmonary vascular dysfunction via activation of signal transducer and activator of transcription 3 and stabilization of hypoxia-inducible factor 1-alpha. Vascul. Pharmacol. 73, 138–148 (2015).
Zhou, Y. et al. Rho/ROCK signal cascade mediates asymmetric dimethylarginine-induced vascular smooth muscle cells migration and phenotype change. Biomed Res Int 2014, 683707 (2014).
Boin, F. et al. Oxidative stress-dependent activation of collagen synthesis is induced in human pulmonary smooth muscle cells by sera from patients with scleroderma-associated pulmonary hypertension. Orphanet journal of rare diseases 9, 123 (2014).
Sandoo, A. et al. Lack of association between asymmetric dimethylarginine and in vivo microvascular and macrovascular endothelial function in patients with rheumatoid arthritis. Clin. Exp. Rheumatol. 30, 388–396 (2012).
McGonagle, D. & McDermott, M. F. A Proposed Classification of the Immunological Diseases. PLoS Medicine 3, e297 (2006).
Erre, G. L. et al. Global microRNA profiling of peripheral blood mononuclear cells in patients with Behcet’s disease. Clinical and experimental rheumatology 33, 72–79 (2015).
Piga, M. et al. Genetics of Behçet’s disease in Sardinia: two distinct extended HLA haplotypes harbour the B* 51 allele in the normal population and in patients. Clinical and Experimental Rheumatology-Incl Supplements 30, S51 (2012).
Böger, R. H. et al. Asymmetric dimethylarginine (ADMA): a novel risk factor for endothelial dysfunction: its role in hypercholesterolemia. Circulation 98, 1842–1847 (1998).
Lundman, P. et al. Mild-to-moderate hypertriglyceridemia in young men is associated with endothelial dysfunction and increased plasma concentrations of asymmetric dimethylarginine. J. Am. Coll. Cardiol. 38, 111–116 (2001).
Surdacki, A. et al. Reduced urinary excretion of nitric oxide metabolites and increased plasma levels of asymmetric dimethylarginine in men with essential hypertension. J. Cardiovasc. Pharmacol. 33, 652–658 (1999).
van der Zwan, L. P. et al. Systemic inflammation is linked to low arginine and high ADMA plasma levels resulting in an unfavourable NOS substrate-to-inhibitor ratio: the Hoorn Study. Clin Sci (Lond). 121, 71–8 (2011).
Siroká, R., Trefil, L., Rajdl, D., Racek, J. & Cibulka, R. Asymmetric dimethylarginine–comparison of HPLC and ELISA methods. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 850, 586–587 (2007).
Schulze, F. et al. Determination of asymmetric dimethylarginine (ADMA) using a novel ELISA assay. Clin. Chem. Lab. Med. 42, 1377–1383 (2004).
Németh, B. et al. The issue of plasma asymmetric dimethylarginine reference range - A systematic review and meta-analysis. PLoS ONE 12, e0177493 (2017).
Atzler, D. et al. Serum reference intervals of homoarginine, ADMA, and SDMA in the study of health in Pomerania. Clin. Chem. Lab. Med. 52, 1835–1842 (2014).
Dimitroulas, T. et al. Left atrial volume and N-terminal pro-B type natriuretic peptide are associated with elevated pulmonary artery pressure in patients with systemic sclerosis. Clin. Rheumatol. 29, 957–964 (2010).
Spinelli, F. R. et al. Effect of therapeutic inhibition of TNF on circulating endothelial progenitor cells in patients with rheumatoid arthritis. Mediators Inflamm. 2013, 537539 (2013).
Angel, K. et al. The L-arginine/asymmetric dimethylarginine ratio is improved by anti-tumor necrosis factor-α therapy in inflammatory arthropathies. Associations with aortic stiffness. Atherosclerosis 225, 160–165 (2012).
Author information
Authors and Affiliations
Contributions
G.L.E. and A.Z. designed the study. G.L.E. and A.Z. searched databases and performed the selection of studies; G.L.E., A.Z., and A.A.M. wrote the manuscript; P.P. and A.Z. analyzed the data; F.C., C.C. and G.P. contributed to writing and critically uprising the manuscript and approved the last version.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Erre, G.L., Mangoni, A.A., Castagna, F. et al. Meta-Analysis of Asymmetric Dimethylarginine Concentrations in Rheumatic Diseases. Sci Rep 9, 5426 (2019). https://doi.org/10.1038/s41598-019-41994-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-41994-5
This article is cited by
-
A systematic review and meta-analysis of circulating adhesion molecules in rheumatoid arthritis
Inflammation Research (2024)
-
Genetic regulation of dimethylarginines and endothelial dysfunction in rheumatoid arthritis
Amino Acids (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
