
Abstract
Sixty-seven patients with first acute ischemic stroke onset between 3 to 7 days and 25 age- and sex- matched controls were analyzed for the performance of a resting-state functional MRI to investigate whether the functional connectivity (FC) of the motor network in acute ischemic stroke is independently associated with functional outcomes. The FC of cortical motor network and default mode network was analyzed. The FC was compared between controls, patients with favorable outcomes (modified Rankin Scale, mRS ≤1), and patients with unfavorable outcomes (mRS ≥2) at 3 months. Of the 67 patients, 23 (34%) exhibited unfavorable outcomes. In multivariate analysis, the FC between ipsilesional primary motor cortex (M1) and contralesional dorsal premotor area (PMd) ≤0.63, were independently associated with unfavorable outcomes (odds ratio = 6.32, P = 0.032), whereas the FC of default mode network was not different between groups. The interhemispheric FC of the motor network is an independent predictor of functional outcomes in patients with acute ischemic stroke.
Similar content being viewed by others


Introduction
Ischemic stroke is a leading cause of disability in developed countries. More than half patients with ischemic stroke can not go back to work despite months of aggressive treatment and rehabilitation1. Age, stroke severity, lesion volume, or lesion location are important factors influencing functional outcome; but none of them could be intervened effectively, and mild stroke severity does not guarantee a favorable outcome2. Several factors, such as uncontrolled hypertension, hyperglycemia, and inflammation, have been proposed to predict unfavorable functional outcomes3,4,5. However, these factors are also associated with stroke severity, and they may account for the consequences more than the causes of the unfavorable outcomes3,6. Most clinical trials targeting these factors have reported controversial results7,8,9. Therefore, it is crucial to explore novel and independent prognostic biomarkers for developing recovery treatment strategies.
Resting-state functional magnetic resonance imaging (fMRI) is a valid research tool for stroke10. With this technique, the functional connectivity (FC) represents the synchrony of intrinsic blood oxygen level-dependent (BOLD) signal fluctuations among different brain regions. A high FC means a good connection of neuronal activities between different brain regions. In patients with ischemic stroke, the FC of the motor network is impaired within hours after stroke onset11, and it changes with motor deficit improvements during longitudinal observations12,13,14. Therefore, the FC of the motor network is a potential imaging biomarker of stroke recovery. The limitations of fMRI in current stroke research are the lack of study in acute disease stage: Most previous studies regarding fMRI in stroke enrolled patients at 2 weeks or later after stroke onset11,12,13,14,15,16,17,18,19,20,21,22,23. Besides, previous studies had relatively small subject number in each study, and it is difficult to eliminate the influence of confounding factors of stroke outcome. Another issue is the potential hemodynamic lag in the hemisphere with ischemic lesions, which may affect the measurement of FC24,25. Some approaches such as cross-correlation are applied in detecting hemodynamic lags in the BOLD signal, and strategies to correct the influence of hemodynamic lags in fMRI are under investigation26,27.
We hypothesized that the FC of the motor network in patients with acute ischemic stroke is worse than health population, and the FC at acute stage of stroke is predictive of the functional outcomes.
Methods
Participants
This study was approved by the Institutional Review Board of Taipei Medical University. The data of this study are available from the corresponding author upon request. All methods were performed in accordance with relevant guidelines and regulations. From Aug 2015 to March 2017, patients with first acute unilateral ischemic stroke confirmed with neuroimaging and with a premorbid mRS score of 0 were consecutively screened when they were admitted to Taipei Medical University Shuang Ho Hospital within 7 days after stroke onset. Each patient was cared for according to standard clinical guidelines28.
MRI with T1- and T2-weighted images, T2 fluid-attenuated inversion recovery (T2 FLAIR) images, diffusion-weighted imaging (DWI), apparent diffusion coefficient maps, and time-of-flight magnetic resonance angiograms (MRA), carotid Doppler ultrasonography, and electrocardiogram of the patients were routinely evaluated. The exclusion criteria included: (1) Acute cortical infarction in the frontal or parietal lobe detected in DWI, which would overlap with the regions of interest (ROIs) of fMRI in this study (2) More than 50% stenosis of carotid, vertebral, or cerebral arteries (3) Pure sensory impairment at admission, which would usually have excellent functional outcome. Eighty-five patients were enrolled in this study, and 25 age- and sex-matched healthy volunteers were enrolled as controls. Written informed consent was obtained from all participants or their legal guardians. The etiologic subtype of stroke was classified according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) study29. An experienced neurologist (Chi) interpreted the lesion volume and location in DWI manually and rated pre-existing white matter hyperintensities in T2 FLAIR by using the Fazekas scale30. Resting-state fMRI was conducted within 7 days (range: 3 to 7 days) after stroke for the patients and once for the controls. The NIHSS was administered on the same day as the resting-state fMRI, and the mRS was evaluated at 3 months (range: 80 to 105 days). The patients with a mRS score of ≤1 at 3 months were defined as having favorable outcome, whereas those with a mRS score of ≥2 at 3 months were defined as having unfavorable outcome.
Resting-State Functional Magnetic Resonance Imaging
The images were acquired on a GE Discovery MR750 3.0 T scanner (General Electric Healthcare, USA) with a gradient echo planar imaging sequence by employing the following imaging parameters: flip angle, 90 degrees; repetition time (TR) = 2000 ms; echo time = 30 ms; field of view, 230 mm; matrix, 64 × 64 (in-plane resolution = 3.6 × 3.6 mm2); slice thickness, 3.0 mm; spacing, 1.0 mm; and scanning time, 360 seconds (180 imaging frames). Each participant had 1 run of imaging acquisition. The imaging acquisition was interleaved and from bottom to top. The subjects were asked to open their eyes and look at a fixed point in front of them during the scan.
Functional Connectivity Analysis
Preprocessing
Preprocessing was performed using Statistical Parametric Mapping (SPM12; http://www.fil.ion.ucl.ac.uk/spm/software/spm12) and Data Processing Assistant for Resting-State fMRI V4.3 (DPARSF; http://rfmri.org)31. All scans were slice timing corrected, head movement corrected, and normalized to the eco-planar imaging template provided by SPM12. Spatial smoothing was performed using a 6-mm full-width half-maximum Gaussian kernel.
After spatial smoothing, potential hemodynamic lags in fMRI were detected by using Regressor Interpolation at Progressive Time Delays (RIPTiDe; https://github.com/bbfrederick/rapidtide)32,33. It uses cross-correlation to find the time course of endogenous low frequency oscillation (LFO, 0.009 to 0.15 Hz) in the mean BOLD signal, which is thought to be the signal of cerebral blood flow, and then it determines the strength and peak time lag of LFO at each voxel. We used RIPTiDe to produce a lag time map of whole brain in each subject. We calculated the average hemodynamic lag of the ROIs at each side of brain, and patients with a lag time difference more than 2 seconds (1 TR) between bilateral sides were excluded in this step (n = 5). In addition, RIPTiDe provides a function named “dynamic Global Signal Regression (dGSR)”34, which generate voxel-specific regressors to filter the signal of cerebral blood flow out of each voxel, therefore it can eliminate the influence of hemodynamic lag when calculating FC. In this study, although we had excluded the patients with substantial lateralized hemodynamic lags, certain hemodynamic lags at some ROIs might still exist. Therefore, in this study we processed the data and presented both the results with and without dGSR.
After preprocessing with and without dGSR, the following procedures were performed using the Resting-State fMRI Data Analysis Toolkit V1.8 (http://www.restfmri.net)35 and DPARSF V4.3. Nuisance signals were eliminated through regression of the following variables: (1) the 6 head movement parameters computed through rigid body translation and rotation during preprocessing, (2) the mean signal of cerebrospinal fluid, and (3) the mean signal within the white matter. After nuisance signals regression, low-frequency time course representing neuronal activities were extracted using a band-pass filter (0.01 to 0.08 Hz).
The framewise displacement (FD) was computed from the 6 head movement parameters. Image frames with FD > 0.5 mm were marked as unacceptable head motion, and the frames 1 back and 2 forward from the marked frames were excluded from FC analysis (image scrubbing)36. Patients with less than 150 image frames (5 minutes) after image scrubbing were excluded in this step (n = 13). Total 67 patients (44 patients with favorable outcomes, 23 patients with unfavorable outcomes) and 25 controls were enrolled for final analysis.
Selection of Regions of Interest (ROIs)
We selected the 5 cortical ROIs of the motor network reported by Wang et al.12, including primary motor cortex (M1), supplementary motor area (SMA), postcentral gyrus (PCG), ventrolateral premotor cortex (PMv), and dorsolateral premotor cortex (PMd). In addition, we selected the default mode network (DMN) to compare with the performance of motor network. The activity of DMN is prominent in resting state and DMN does not involve much about motor or language function, therefore it is suitable as the control network in this study. We selected 5 ROIs of DMN, including posterior cingulate cortex (PCC), anterior medial prefrontal cortex (amPFC), inferior parietal lobule (IPL), retrosplenial cortex (Rsp), and anterior hippocampus (AnHip). The ROI coordinates were based on the Montreal Neurological Institute system, and the ROIs represented 6-mm-radius spheres. All ROI coordinates used in this study are provided in the Supplementary Material. The ipsilesional ROIs were expressed as “iROI” (e.g., iM1), and the contralesional ROIs were expressed as “cROI” (e.g., cM1).
Extraction of the Time Courses of ROIs and Construction of the Resting State Network
The time courses of each ROI were extracted. The Pearson correlation coefficient of the average time courses for each ROI pair was calculated as the FC, and Fisher’s z transformation was applied to convert the FC to normal distribution. The FC between all ROIs of the motor network were calculated for each subject. The FC between ROIs was expressed as “the FC of ROI/ROI” (e.g., FC of iM1/cM1). The FC matrices and anatomic distribution figures were produced by using BrainNet Viewer toolbox V1.5337.
Statistical Analyses
Data normality was tested by using the Shapiro-Wilk test. The demographic data between controls, patients with favorable outcomes, and patients with unfavorable outcomes were compared by using analysis of variance (ANOVA), the Kruskal-Wallis test, or Chi-square test and post hoc analysis. The FC between groups were compared by ANOVA, the false discovery rate (FDR) corrected P < 0.05 was considered statistically significant38. The Tukey-Kramer test was applied as the post hoc analysis when P value of ANOVA was considered statistically significant. The FC which was significantly different between the patients with favorable and unfavorable functional outcomes were chosen for further analysis: The receiver operating characteristic (ROC) analysis was used for testing the sensitivity and specificity of the FC, as well as its best cut-off value in identifying patients with unfavorable functional outcomes. A univariate logistic regression analysis was conducted to estimate the odds ratio (OR) of unfavorable functional outcomes for the demographic variables and FC. Age, sex, and variables with P ≤ 0.10 in the univariate logistic regression analysis were included in a multivariate logistic regression model to adjust the OR of unfavorable functional outcomes. In order to ensure the independence between variables included in the multivariate logistic regression, the variables were put in a multiple linear regression model (dependent variable: mRS at 3 months) to check the variance inflation factor (VIF), and the variable with a VIF ≥ 10 will be excluded from multivariate logistic regression to avoid the problem of multicollinearity. Normally distributed data are expressed as mean ± standard deviation, non-normal data are expressed as the median value and interquartile range (IQR). P < 0.05 was considered statistically significant. Statistical data were analyzed using MedCalc Statistical Software V17 (MedCalc Software bvba, Ostend, Belgium). The flowchart of study protocol is presented in the Fig. 1.

Flowchart of study protocol.
Results
The clinical characteristics of the controls (n = 25), patients with favorable outcomes (n = 44), and patients with unfavorable outcomes (n = 23) are summarized in Table 1. No significant differences were observed in age and sex among the three groups. The proportion of patients with hypertension and hyperlipidemia was significantly higher than in controls. The proportion of having corticospinal tract lesion in DWI and the stroke etiologies were not different between patients with favorable and unfavorable outcomes. The most common stroke etiology was small vessel disease, followed by large artery atherosclerosis. Most patients had mild stroke severity (NIHSS: median = 3 in patients with favorable outcome, 4 in patients with unfavorable outcomes), small lesion volume in DWI (median = 0.60 cm3 in patients with favorable outcomes, 1.40 cm3 in patients with unfavorable outcomes), and mild pre-existing white matter hyperintensities (median score of periventricular and deep white matter Fazekas scale = 1 and 1 respectively).The spatial distribution of ischemic lesions in patients is presented in the Fig. 2. The FC matrices of motor network are presented in the Fig. 3, and the corresponding ANOVA P value matrices of the 3-group comparison are presented in the Fig. 4. The FC of iM1/cM1, iM1/cPCG, iM1/cPMd, iPCG/cM1, iPCG/cPCG, iPCG/cPMd, iPMv/cPMv, and cM1/cPCG were significantly different between the three groups. In the post hoc test of ANOVA (Fig. 5), all aforementioned FC were significantly lower in patients with unfavorable outcomes than in controls, and FC of iM1/cM1, iM1/cPCG, iPCG/cM1, and iPCG/cPMd were not different between patients with favorable outcomes and controls. Only the FC of iM1/cPMd was significantly lower in patients with unfavorable outcomes than in patients with favorable outcomes. The FC with significant differences between the controls and patients are presented in Fig. 6A.

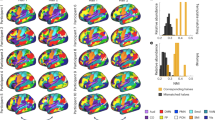
Heat map of ischemic lesion in patients.

Motor network functional connectivity matrices (mean) ROIs: 1 = iM1, 2 = iSMA, 3 = iPCG, 4 = iPMd, 5 = iPMv 6 = cM1, 7 = cSMA, 8 = cPCG, 9 = cPMd, 10 = cPMv.

(A) The ANOVA P value matrices of the 3-group comparison in motor network functional connectivity ROIs: 1 = iM1, 2 = iSMA, 3 = iPCG, 4 = iPMd, 5 = iPMv 6 = cM1, 7 = cSMA, 8 = cPCG, 9 = cPMd, 10 = cPMv *FDR corrected P < 0.05 (B) Motor network ROIs.

Functional connectivity comparison between groups *Significant difference in the post hoc test of ANOVA.

(A) Motor functional connectivity (FC) different between groups Gray lines: FC different between controls and patients Red line: FC different between patients with favorable and unfavorable outcomes (B) Receiver operating characteristics curve of iM1/cPMd in identifying patients with unfavorable outcome (mRS ≥ 2) The sensitivity = 82.6% and specificity = 47.7%, the optimal cut-off value = 0.63.
ROC analysis showed that the area under curve (AUC) of the FC of iM1/cPMd was 0.659 [95% confidence interval (CI) = 0.533–0.770, P = 0.023] (Fig. 6B). The sensitivity and specificity of identifying the patients with unfavorable outcomes was 82.6% and 47.7% in the FC of iM1/cPMd, and the optimal cut-off value was 0.63. Therefore, the FC of iM1/cPMd ≤ 0.63 is a valid predictor of unfavorable functional outcomes in acute ischemic stroke.
The FC matrices of DMN are presented in the Fig. 7, and the corresponding ANOVA P value matrices of the 3-group comparison are presented in the Fig. 8. The FC of between any 2 ROIs in DMN are not significantly different between the three groups after FDR correction. Therefore, the FC of DMN is not predictive of functional outcome in acute ischemic stroke. In addition, it provide an evidence that the motor network FC difference between the three groups was not due to the presence of global physiological noises such as motions in a specific group.

Default mode network functional connectivity matrices (mean) ROIs: 1 = iPCC, 2 = iamPFC, 3 = iIPL, 4 = iRsp, 5 = iAnHip 6 = cPCC, 7 = camPFC, 8 = cIPL, 9 = cRsp, 10 = cAnHip.

(A) The ANOVA P value matrices of the 3-group comparison in default mode network functional connectivity ROIs: 1 = iPCC, 2 = iamPFC, 3 = iIPL, 4 = iRsp, 5 = iAnHip 6 = cPCC, 7 = camPFC, 8 = cIPL, 9 = cRsp, 10 = cAnHip No significant difference existed after FDR correction (B) Defualt mode network ROIs.
The FC matrices of motor network by using dGSR are presented in the Fig. 9, and the corresponding ANOVA P value matrices of the 3-group comparison are presented in the Fig. 10. The FC of between any 2 ROIs in motor network are not significantly different between the three groups after FDR correction.

Motor network functional connectivity matrices (mean) by using dynamic Global Signal Regression ROIs: 1 = iM1, 2 = iSMA, 3 = iPCG, 4 = iPMd, 5 = iPMv = cM1, 7 = cSMA, 8 = cPCG, 9 = cPMd, 10 = cPMv.

The ANOVA P value matrices of the 3-group comparison in motor network by using dynamic Global Signal Regression ROIs: 1 = iM1, 2 = iSMA, 3 = iPCG, 4 = iPMd, 5 = iPMv 6 = cM1, 7 = cSMA, 8 = cPCG, 9 = cPMd, 10 = cPMv No significant difference existed after FDR correction.
Table 2 presents the results of univariate and multivariate logistic regression analyses of variables potentially predicting unfavorable functional outcomes. In univariate logistic regression analysis, hypertension, lesion at the corticospinal tract, NIHSS score, and the FC of iM1/cPMd ≤0.63 were significant predictors, whereas age, sex, diabetes, hyperlipidemia, atrial fibrillation, DWI lesion on the left side, DWI lesion volume, and Fazekas scale were not significant predictors. There was weak association between iM1/cPMd and age (correlation coefficient = −0.225, P = 0.031). In the multicollinearity test, age, sex, hypertension, lesion at the corticospinal tract, and NIHSS score had small VIF (<1.2), therefore, they were included in the multivariate logistic regression analysis to adjust the OR of the FC of iM1/cPMd ≤0.63. In the multivariate analysis, age and sex became significant predictors, whereas lesion at corticospinal tract became non-significant. The FC of iM1/cPMd ≤0.63 and NIHSS score remained significant predictors of unfavorable functional outcomes. In this multivariate logistic regression, the Nagelkerke R2 was 0.604. Therefore, the FC of iM1/cPMd is an independent outcome predictor among the FC in patients with acute ischemic stroke.
Discussion
Resting-state fMRI was proposed as a potential tool for predicting stroke outcomes10. The advantage of using resting-state fMRI instead of task-based fMRI in patients with stroke is that it can minimize the interindividual differences in the task performance and easily be integrated into routine clinical MRI. Previous studies have reported that FC improves with neurological functional recovery during longitudinal follow-up12,13,14,15,17,39,40, and FC is associated with neurological scores at certain observation time points16,19,21,41,42. Most previous studies regarding fMRI in stroke enrolled patients at 2 weeks or later after stroke onset with about 20 patients in each study11,12,13,14,15,16,17,18,19,20,21,22,23, so it was not possible to test the predictive power of FC by using multivariate analyses. This study analyzed 67 patients with acute ischemic stroke and mild severity, so it was able to find an optimal cut-off value of FC that predicts functional outcomes, and using multivariate analyses could clarify its association with other risk factors of unfavorable functional outcomes.
The disturbance in FC after mild to moderate ischemic stroke has been reported either within the ipsilesional hemisphere or between hemispheres11,12,13,39. Using resting-state fMRI, we determined that the interhemispheric FC of motor network in patients was lower than that in controls. However, only the FC of iM1/cPMd was significantly different between the patients with favorable and unfavorable functional outcomes (Figs 5 and 6). In studies using iM1 as the primary ROI, it was found that the interhemispheric FC increased and ipsilesional intrahemispheric FC decreased after rehabilitation39. In addition, decreased FC between bilateral motor cortices correlated with the neurological functions more favorably than that within ipsilesional motor cortices did11,16,17. Therefore, the interhemispheric FC might be more important than the ipsilesional intrahemispheric FC in the functional recovery of ischemic stroke. The PMd belongs to the Brodmann area 6, and it accounts for integrating the sensory information and movement targeting43. In a study of patients with stroke, contralesional PMd is more active compared with in healthy controls, which is thought to support the motor recovery44, and inhibitory repetitive transcranial magnetic stimulation (rTMS) of contralesional PMd worsen the recovered performance of paretic hand45. Therefore, it is reasonable that the FC of iM1/cPMd play a crucial role in the recovery of stroke.
In our study, the FC of iM1/cPMd at the acute stage of ischemic stroke independently predicted the functional outcome. Therefore, FC in fMRI appears to be a valid and timely imaging biomarker for acute ischemic stroke. Moreover, the FC is a potentially treatable target in stroke patients. By using neurostimulation techniques such as high frequency rTMS or anodal transcranial direct current stimulation (tDCS), the excitability of the motor cortices can be enhanced. However, the therapeutic effect of rTMS or tDCS in stroke remains controversial46,47. This may be explained by the lack of appropriate patient selection in past studies. The FC of motor cortices assessed by using resting state fMRI can help identifying the patients with high risk of unfavorable functional outcome, who may truly benefit from neurostimulation therapies.
Although the FC of iM1/cM1, iM1/cSMA, iM1/iPMd, and iM1/cPMd were reported to be correlated with patients’ neurological function in the chronic stage of stroke17,39,44,48,49. only the FC of iM1/cPMd was found to be significantly different between the patients with favorable and unfavorable functional outcomes in this study. An explanation is the difference of neurological rating scale between studies: most studies used the Fugl–Meyer Assessment (FMA) or only the motor domain of FMA, whereas we used NIHSS and mRS. The FMA is a more sophisticated rating scale than the mRS or NIHSS, therefore the FMA might be more sensitive in detecting the interindividual difference of neurological function. Nevertheless, the NIHSS and mRS are the most commonly used neurological rating scales in clinical studies of stroke, and the definition of mRS ≤ 1 as a favorable functional outcome has been commonly used. The FMA may be less amenable in clinical practice because it is more complex and requires a substantially longer administration time compared with the NIHSS or mRS50.
An interesting finding of this study is that after using dGSR, the differences of moto network FC between the three groups disappeared, although we had excluded the patients with substantial lateralized hemodynamic lags in advance. It is possible that the FC differences were driven by hemodynamic lags at some but not all ROIs of motor network, and dGSR eliminated the influence of hemodynamic lag to FC, therefore the FC abnormalities in patients were restored. In previous studies of FC in stroke, hemodynamic lags were managed by different approaches: 1. Excluding the subjects with lateralized hemodynamic lags51. 2. Shifting the time courses of ROIs with a hemodynamic lag to re-align with the global signal27, and 3. Using voxel-specific regressors to filter cerebral blood flow signal out of each voxel (dGSR)33. In this study, the motor network FC differences between groups existed after excluding the subjects with lateralized hemodynamic lags, but disappeared after using dGSR. Therefore, different managements of a hemodynamic lag result in different conclusions, and it is worth more investigations in the management of hemodynamic lag in fMRI.
In this study the DWI lesion volume was not a significant outcome predictor in the regression analysis. This result is not consistent with the common sense that large infarction volume is associated with poor outcome. The most probable reason of this result is that the lesion volume in our patients were consistently small, and some patients had large lesions at non-motor area such as posterior cerebral artery territory. This point of view is supported by the non-significant correlation between lesion volume and NIHSS score in our patients (correlation coefficient = 0.187, P = 0.129). Therefore, it is reasonable that the lesion volume is not predictive of outcome in our data.
This study has limitations. First, we excluded patients with frontal or parietal cortical infarction that could involve the ROIs in this study, as well as patients with significant vascular stenosis. The current fMRI analytic methods would raise concerns of inaccurately calculating FC in patients with lesions in ROIs or with significant vascular stenosis. Second, the mechanism underlying poor FC in patients with unfavorable outcomes compared with those with favorable outcomes remains unclear and could not be identified in the present study. Third, there is no validation test of the cut-off FC values in this study, which will need a new group of patients to validate our findings.
In conclusion, the cortical FC of the motor network is impaired in patients with acute ischemic stroke; in particular, the FC of iM1/cPMd at the acute stage is independently associated with functional outcomes. These findings require validation in another group of patients.
Data Availability
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
References
Hsieh, F. I. et al. Get With the Guidelines-Stroke performance indicators: surveillance of stroke care in the Taiwan Stroke Registry: Get With the Guidelines-Stroke in Taiwan. Circulation 122, 1116–1123 (2010).
Khatri, P., Conaway, M. R. & Johnston, K. C. & Acute Stroke Accurate Prediction Study, I. Ninety-day outcome rates of a prospective cohort of consecutive patients with mild ischemic stroke. Stroke 43, 560–562 (2012).
Capes, S. E., Hunt, D., Malmberg, K., Pathak, P. & Gerstein, H. C. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke 32, 2426–2432 (2001).
Yong, M. & Kaste, M. Association of characteristics of blood pressure profiles and stroke outcomes in the ECASS-II trial. Stroke 39, 366–372 (2008).
Tuttolomondo, A. et al. Inflammation as a therapeutic target in acute ischemic stroke treatment. Curr Top Med Chem 9, 1240–1260 (2009).
Tikhonoff, V., Zhang, H., Richart, T. & Staessen, J. A. Blood pressure as a prognostic factor after acute stroke. Lancet Neurol 8, 938–948 (2009).
Gray, C. S. et al. Glucose-potassium-insulin infusions in the management of post-stroke hyperglycaemia: the UK Glucose Insulin in Stroke Trial (GIST-UK). Lancet Neurol 6, 397–406 (2007).
Sare, G. M., Geeganage, C. & Bath, P. M. High blood pressure in acute ischaemic stroke–broadening therapeutic horizons. Cerebrovasc Dis 27(Suppl 1), 156–161 (2009).
Use of anti-ICAM-1 Therapy in ischemic stroke: results of the Enlimomab Acute Stroke Trial. Neurology 57, 1428–1434 (2001).
Ovadia-Caro, S., Margulies, D. S. & Villringer, A. The value of resting-state functional magnetic resonance imaging in stroke. Stroke 45, 2818–2824 (2014).
Golestani, A. M., Tymchuk, S., Demchuk, A., Goodyear, B. G. & Group, V.-S. Longitudinal evaluation of resting-state FMRI after acute stroke with hemiparesis. Neurorehabil Neural Repair 27, 153–163 (2013).
Wang, L. et al. Dynamic functional reorganization of the motor execution network after stroke. Brain 133, 1224–1238 (2010).
Zheng, X. et al. The plasticity of intrinsic functional connectivity patterns associated with rehabilitation intervention in chronic stroke patients. Neuroradiology, https://doi.org/10.1007/s00234-016-1647-4 (2016).
Fan, Y. T. et al. Neuroplastic changes in resting-state functional connectivity after stroke rehabilitation. Front Hum Neurosci 9, 546 (2015).
James, G. A. et al. Changes in resting state effective connectivity in the motor network following rehabilitation of upper extremity poststroke paresis. Top Stroke Rehabil 16, 270–281 (2009).
Carter, A. R. et al. Resting interhemispheric functional magnetic resonance imaging connectivity predicts performance after stroke. Ann Neurol 67, 365–375 (2010).
Park, C. H. et al. Longitudinal changes of resting-state functional connectivity during motor recovery after stroke. Stroke 42, 1357–1362 (2011).
Carter, A. R. et al. Upstream dysfunction of somatomotor functional connectivity after corticospinal damage in stroke. Neurorehabil Neural Repair 26, 7–19 (2012).
Yin, D. et al. Patterns in cortical connectivity for determining outcomes in hand function after subcortical stroke. PLoS One 7, e52727 (2012).
Dacosta-Aguayo, R. et al. Prognostic value of changes in resting-state functional connectivity patterns in cognitive recovery after stroke: A 3T fMRI pilot study. Hum. Brain Mapp. 35, 3819–3831 (2014).
Dacosta-Aguayo, R. et al. Impairment of functional integration of the default mode network correlates with cognitive outcome at three months after stroke. Hum Brain Mapp 36, 577–590 (2015).
Zhang, Y. et al. Abnormal functional networks in resting-state of the sub-cortical chronic stroke patients with hemiplegia. Brain Res. 1663, 51–58 (2017).
Liu, G. et al. Increased spontaneous neuronal activity in structurally damaged cortex is correlated with early motor recovery in patients with subcortical infarction. Eur J Neurol 22, 1540–1547 (2015).
Amemiya, S., Kunimatsu, A., Saito, N. & Ohtomo, K. Impaired hemodynamic response in the ischemic brain assessed with BOLD fMRI. Neuroimage 61, 579–90 (2012).
Lv, Y. et al. Identifying the perfusion deficit in acute stroke with resting-state functional magnetic resonance imaging. Ann. Neurol. 73, 136–139 (2013).
DeB Frederick, B., Nickerson, L. D. & Tong, Y. Physiological denoising of BOLD fMRI data using Regressor Interpolation at Progressive Time Delays (RIPTiDe) processing of concurrent fMRI and near-infrared spectroscopy (NIRS). Neuroimage 60, 1913–23 (2012).
Siegel, J. S., Snyder, A. Z., Ramsey, L., Shulman, G. L. & Corbetta, M. The effects of hemodynamic lag on functional connectivity and behavior after stroke. J. Cereb. Blood Flow Metab. 36, 2162–2176 (2016).
Jauch, E. C. et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 44, 870–947 (2013).
Adams, H. P. Jr et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 24, 35–41 (1993).
Fazekas, F., Chawluk, J. B., Alavi, A., Hurtig, H. I. & Zimmerman, R. A. Mr Signal Abnormalities At 1.5-T in Alzheimer Dementia and NormalAging. Am. J. Roentgenol. 149, 351–356 (1987).
Chao-Gan, Y. & Yu-Feng, Z. DPARSF: A MATLAB Toolbox for ‘Pipeline’ Data Analysis of Resting-State fMRI. Front Syst Neurosci 4, 13 (2010).
Tong, Y., Bergethon, P. R. & DeB Frederick, B. An improved method for mapping cerebrovascular reserve using concurrent fMRI and near-infrared spectroscopy with Regressor Interpolation at Progressive Time Delays (RIPTiDe). Neuroimage 56, 2047–2057 (2011).
Donahue, M. J. et al. Time delay processing of hypercapnic fMRI allows quantitative parameterization of cerebrovascular reactivity and blood flow delays. J. Cereb. Blood Flow Metab. 36, 1767–1779 (2016).
Erdoğan, S. B., Tong, Y., Hocke, L. M., Lindsey, K. P. & DeB Frederick, B. Correcting for Blood Arrival Time in Global Mean Regression Enhances Functional Connectivity Analysis of Resting State fMRI-BOLD Signals. Front. Hum. Neurosci. 10, 1–22 (2016).
Song, X. W. et al. REST: a toolkit for resting-state functional magnetic resonance imaging data processing. PLoS One 6, e25031 (2011).
Power, J. D., Barnes, K. A., Snyder, A. Z., Schlaggar, B. L. & Petersen, S. E. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. Neuroimage 59, 2142–2154 (2012).
Xia, M., Wang, J. & He, Y. BrainNet Viewer: a network visualization tool for human brain connectomics. PLoS One 8, e68910 (2013).
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society 57, 289–300 (1995).
Zhang, Y. et al. Relationship between functional connectivity and motor function assessment in stroke patients with hemiplegia: a resting-state functional MRI study. Neuroradiology, https://doi.org/10.1007/s00234-016-1646-5 (2016).
Bannister, L. C., Crewther, S. G., Gavrilescu, M. & Carey, L. M. Improvement in Touch Sensation after Stroke is Associated with Resting Functional Connectivity Changes. Front Neurol 6, 165 (2015).
Ding, X. et al. Patterns in default-mode network connectivity for determining outcomes in cognitive function in acute stroke patients. Neuroscience 277, 637–646 (2014).
Park, J. Y. et al. Significance of longitudinal changes in the default-mode network for cognitive recovery after stroke. Eur J Neurosci 40, 2715–2722 (2014).
Hoshi, E. & Tanji, J. Functional specialization in dorsal and ventral premotor areas. Prog. Brain Res. 143, 507–11 (2004).
Bestmann, S. et al. The role of contralesional dorsal premotor cortex after stroke as studied with concurrent TMS-fMRI. J. Neurosci. 30, 11926–37 (2010).
Lotze, M. et al. The role of multiple contralesional motor areas for complex hand movements after internal capsular lesion. J. Neurosci. 26, 6096–102 (2006).
Hao, Z., Wang, D., Zeng, Y. & Liu, M. Repetitive transcranial magnetic stimulation for improving function after stroke. Cochrane Libr. 5, (2013).
Elsner, B., Kugler, J., Pohl, M. & Mehrholz, J. Transcranial direct current stimulation (tDCS) for improving activities of daily living, and physical and cognitive functioning, in people after stroke. Cochrane database Syst. Rev. 3, CD009645 (2016).
Wittenberg, G. F. et al. Predictors and brain connectivity changes associated with arm motor function improvement from intensive robotic practice in chronic stroke. F1000Research 5, 2119 (2016).
Wu, J. et al. Connectivity measures are robust biomarkers of cortical function and plasticity after stroke. Brain 138, 2359–2369 (2015).
Malouin, F., Pichard, L., Bonneau, C., Durand, A. & Corriveau, D. Evaluating motor recovery early after stroke: comparison of the Fugl-Meyer Assessment and the Motor Assessment Scale. Arch. Phys. Med. Rehabil. 75, 1206–12 (1994).
Siegel, J. S. et al. Disruptions of network connectivity predict impairment in multiple behavioral domains after stroke. Proc. Natl. Acad. Sci. 113, E4367–E4376 (2016).
Acknowledgements
We thank Prof. Chia-Shu Lin (National Yang-Ming University) and Ms. Yi-Tien Lee (Shuang Ho Hospital) for the assistance of figures production, Prof. Chang-Wei Wu (Taipei Medical University) and Dr. Nai-Wen Chi (National Taiwan University) for the assistance in fMRI analytic works. This study was supported by the Taiwan Ministry of Science and Technology (MOST 103-2314-B-038-004, MOST 105-2314-B-038-003, MOST 105-2314-B-038-007), Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW105-TDU-B-212-113004); China Medical University Hospital, Academia Sinica Taiwan Biobank, Stroke Biosignature Project (BM10601010036); and Taiwan Clinical Trial Consortium for Stroke (MOST 106-2321-B-039-005).
Author information
Authors and Affiliations
Contributions
N.F. Chi, H.L. Ku, H.Y. Chiou and C.J. Hu- Study concept and design N.F. Chi, H.L. Ku, D. Y.T. Chen, Y.C. Tseng, C.J. Chen, Y.C. Lin, L. Chan and C.J. Hu- Acquisition of data N.F. Chi, H.L. Ku, D. Y.T. Chen, Y.C. Hsieh and C.J. Hu- analysis and interpretation N.F. Chi, H.L. Ku, D. Y.T. Chen, Y.C. Hsieh, H.Y. Chiou, C.Y. Hsu and C.J. Hu- critical revision of the manuscript for important intellectual content H.Y. Chiou, C.Y. Hsu, and C.J. Hu- study supervision.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chi, NF., Ku, HL., Chen, D.YT. et al. Cerebral Motor Functional Connectivity at the Acute Stage: An Outcome Predictor of Ischemic Stroke. Sci Rep 8, 16803 (2018). https://doi.org/10.1038/s41598-018-35192-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-35192-y
Keywords
This article is cited by
-
Disruption of Resting-State Functional Connectivity in Acute Ischemic Stroke: Comparisons Between Right and Left Hemispheric Insults
Brain Topography (2024)
-
Structural and functional reorganization following unilateral internal capsule infarction contribute to neurological function recovery
Neuroradiology (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
