
Abstract
The purpose of this study is to evaluate similarities and differences in gut bacterial measurements and stability in the microbial communities of three different types of samples that could be used to assess different niches of the gut microbiome: rectal swab, stool, and normal rectal mucosa samples. In swab-stool comparisons, there were substantial taxa differences with some taxa varying largely by sample type (e.g. Thermaceae), inter-individual subject variation (e.g. Desulfovibrionaceae), or by both sample type and participant (e.g. Enterobacteriaceae). Comparing all three sample types with whole-genome metagenome shotgun sequencing, swab samples were much closer to stool samples than mucosa samples although all KEGG functional Level 1 and Level 2 pathways were significantly different across all sample types (e.g. transcription and environmental adaptation). However, the individual signature of participants was also observed and was largely stable between two time points. Thus, we found that while the distribution of some taxa was associated with these different sampling techniques, other taxa largely reflected individual differences in the microbial community that were insensitive to sampling technique. There is substantial variability in the assessment of the gut microbial community according to the type of sample.
Similar content being viewed by others


Introduction
With recent advances in next-generation sequencing, our understanding of the role of the microbiome in health has dramatically increased1,2,3,4,5,6. The human colorectum microbiome is responsible for a substantial number of physiological functions that have both localized and systemic effects on human health including immunity, nutrient metabolism, growth, and energy harvesting3,7,8,9. Compositional shifts in the diversity or relative distributions of members of the gut microbiota have begun to be linked to several diseases1,2,3,4,5,6.
In the colorectum, there are different niches in which the gut microbiota may reside or interact with the human mucosal microenvironment. In addition to bacterial communities in the lumen, the epithelium is also covered by a mucus layer in which bacterial communities have been found. The function and prevalence of the microbiota within the colorectum likely varies by these niches (i.e. luminal vs. adherent mucosa)10,11,12. For example, studies have found the colon has the steepest oxygen gradient in the body, with anoxia sharply increasing from the mucosa to the middle of lumen13. Thus, luminal microbes are more likely to be anaerobic than mucosal communities12. Anaerobic luminal bacteria may play a key role in fermentation and metabolism of luminal contents (e.g. nutrients or carcinogens)13,14,15 while mucosal bacteria may be involved with autoimmune functions. In addition to differences in oxygen gradients, previous studies have found adherent mucosal communities are less diverse than luminal bacteria although they share many of the same predominant species10,11,13,15,16,17.
Differences in microbial communities are not only driven by niche, but can also reflect differences between individual human hosts. There have been many studies, including the Human Microbiome Project (HMP), that have observed more between-person variation than within-person variation leading to the conclusion that adults have an average unique microbial signature that is largely stable over time10,18,19,20,21,22. Individual microbial signatures have also been demonstrated in longitudinal studies. Rajilić-Stojanović et al. collected stool samples up to 9 times from 5 individuals over a decade and found that although there were some changes in abundances with age, individual-specific patterns persisted18. The findings from their study also indicated a single spot stool sample was not able to capture the presence of all core colonizers.
Many studies of the gut microbiome rely on collection and characterization of stool samples. Although stool may be the most convenient sample, it may only capture information about luminal bacteria which are more transient compared to adherent bacteria. Unfortunately, collection of mucosal samples by biopsy is a highly invasive procedure with risks of perforation that make it unfeasible for large-scale studies. Rectal swabs may prove a simple and inexpensive collection method that may sample both mucosal and luminal communities. Previous comparisons between swab and mucosal samples have shown that swab samples may capture many of the same bacteria as mucosal biopsy samples but also may be different than stool samples12,16,23. However, these previous studies have been small, did not compare samples from the same individual, collected samples post-bowel cleansing and/or did not make these comparisons using whole-genome shotgun sequencing (WGS). In addition, no previous study has evaluated within-person variation or stability for rectal swabs despite swabs being a collection method that may be more feasibly collected in a clinical setting than either stool or mucosal samples. In this study, we compared the microbial composition of stool samples, rectal swabs, and histologically normal rectal mucosa using both 16S rRNA amplicon sequencing and whole genome shotgun (WGS) sequencing and also compare composition of samples collected at two time points.
Methods
Study Population
The participants in this study were selected from the Personalized Prevention of Colorectal Cancer Trial (PPCCT), an on-going, double-blind, placebo-controlled, randomized clinical trial of 12 weeks designed to test the interaction between TRPM7 genotype and reduction of calcium/magnesium intake ratio by magnesium supplementation on colorectal carcinogenesis biomarkers. The study is registered at ClinicalTrials.gov (NCT01105169). The study was approved by the Vanderbilt Institutional Review Board. All study procedures were performed in accordance with relevant guidelines and regulations as approved by the Vanderbilt Institutional Review Board.
Eligibility for the parent trial included 40–85 years of age, in good health, ability to participate in a supplement intervention, personal history of colorectal polyps, known TRPM7 rs8042919 genotype, and daily calcium intake between 700–2000 mg/day and a ratio of daily intake of calcium and magnesium greater than 2.6. Exclusion criteria included any personal history of cancer other than non-melanoma skin cancer, colon resection or colectomy, gastric bypass, organ transplantation, inflammatory bowel disease, chronic diarrhea, chronic renal diseases, hepatic cirrhosis, chronic ischemic heart disease, or Type I diabetes mellitus. Also excluded were individuals using medications that may potentially interact with magnesium, or who were breastfeeding or pregnant. Eligible participants were randomized to receive either placebo (microcrystalline cellulose) or personalized magnesium supplementation (magnesium glycinate) for twelve weeks. Participants, health care providers and investigators were blinded to treatment assignments.
Participants included in the analysis reported here were selected and assayed at two different time points from individuals with biospecimens who had completed the trial at the time of selection. Participants were excluded if they used oral or injected antibiotics in the past 12 months before the study or during the study period. Selection for this analysis was prioritized to include individuals with a history of colorectal adenoma and known recurrence status (50% with recurrence, 50% without recurrence), with the less common TRPM7 GA/AA genotype (n = 18), or for whom immunohistochemistry findings were completed (n = 51). From these criteria, individuals were randomly selected such that 50% were from the placebo arm and 50% from the treatment arm. A total of 60 individuals were selected from 150 participants enrolled between 4/11/2011 and 12/11/2013. Characteristics of the study participants included in this analysis are described in Supplementary Table S1.
Sample Collection
Longitudinal samples were collected from the same subject at an interval of approximately three months. Participants collected stool samples at home up to 3 days prior to their in-person clinic visits. Stool was passed in to a white plastic collection container (FisherbrandTM, Fisher Scientific, 02544208) covering the bowl of the toilet. Wearing gloves, participants scooped three portions of the stool in to four empty sterile feces collection containers (Sarstedt Inc, NC0705093). Samples were immediately frozen in their home freezer. They were also provided with a Styrofoam cooler and ice pack to use to transport the sample to the visit site. Upon receipt, the samples were placed in −80 °C freezers until future analysis. When possible, all stool samples for a participant were collected at the same time of day across the study period to avoid potential variability due to circadian rhythms. The mean (standard deviation) days between the collection and clinic visit was 1 (1.5) day.
At the clinic visits, the study physician inserted a culturette swab through the anal canal, swabbed the distal rectal mucosa, and immediately placed the swab into the empty storage vial. Rectal mucosal biopsies were then obtained through an anoscope using standard mucosal biopsy forceps and these samples were placed into separate storage vials. All the samples were immediately frozen at −80 °C until use. No colon cleansing preparation was used. The mean (standard deviation) days between the first sample collection and the last sample collection was 86.4 (6.6) days.
DNA isolation
DNA was isolated using the E.Z.N.A. Stool DNA kit (Omega Biotek Inc., Norcross, GA) following manufacturer’s instructions including the optional incubation at 95 °C to ensure optimal lysis of Gram positive bacteria. After isolation, DNA was resuspended in 10 mM Tris-HCl (pH 8), aliquoted, and stored at −80 °C long term (before and after processing) or −20 °C short term (<2 weeks processing).
16S rRNA amplicon sequencing
16S rRNA amplicon sequencing was conducted for 60 participants. 12.5 ng of total bacterial DNA was amplified using primers consisting of a locus-specific portion targeting the V1–V2 region of the bacterial 16S rRNA gene using previously described primers24,25 and overhang adapter sequences appended to the primer pair for compatibility with the specific Illumina index and sequencing adapters. The complete sequences of the primers were: F – 5′ TCGTCGGCAGCGTCAGATGTGTATAAGAGACAGAGAGTTTGATCCTGGCTCAG 3′ and R – 5′ GTCTCGTGGGCTCGGAGATGTGTATAAGAGACAGGCTGCCTCCCGTAGGAGT 3′.
Master mixes for the first round of PCR reactions contained 2× KAPA HIFI HotStart ReadyMix (KAPA Biosystems, Wilmington, MA). The thermal profile for the amplification of each sample had an initial denaturing step at 95 °C of 3 minutes, followed by a cycling of denaturing of 95 °C for 30 seconds, annealing at 55 °C for 30 seconds and a 30 second extension at 72 °C (25 cycles), a 5 minute extension at 72 °C and a final hold at 4 °C. Each 16S amplicon was purified using the AMPure XP reagent (Beckman Coulter, Indianapolis, IN) as recommended by the manufacturer. Next, each sample was amplified using a limited cycle PCR program, adding Illumina sequencing adapters and dual‐index barcodes (index 1(i7) and index 2(i5)) (Illumina, San Diego, CA) to the amplicon target. The thermal profile for sample amplification had an initial denaturing step at 95 °C of 3 minutes, followed by a cycling of denaturing of 95 °C for 30 seconds, annealing at 55 °C for 30 seconds and a 30 second extension at 72 °C (8 cycles), a 5 minute extension at 72 °C and a final hold at 4 °C. The final libraries were again purified using the AMPure XP reagent quantified and normalized prior to pooling. The DNA library pool was then denatured with NaOH, diluted with hybridization buffer and heat denatured before loading on the MiSeq reagent cartridge (Illumina) and on the MiSeq instrument (Illumina). Automated cluster generation and paired-end sequencing with dual reads were performed per the manufacturer’s instructions.
Whole-genome shotgun metagenomics DNA sequencing
Whole-genome shotgun metagenomics (WGS) DNA sequencing was conducted for 50 participants including 100 stool samples, 28 rectal swabs, and 16 mucosa samples. For library preparation, 1 ng of intact genomic DNA was processed using the Nextera XT DNA Sample Preparation Kit (Illumina). The target DNA was simultaneously fragmented and tagged by the Nextera Enzyme Mix containing transposome that fragments the input DNA and adds the bridge PCR (bPCR)-compatible adaptors required for binding and clustering on the flowcell. Next, DNA was amplified using a limited-cycle PCR program adding index 1(i7) and index 2(i5) (Illumina) in unique combinations and sequences specific for cluster formation. The thermal profile for the amplification had an initial extension step at 72 °C for 3 minutes and initial denaturing step at 95 °C for 30 seconds, followed by 12 cycles of denaturing of 95 °C for 10 seconds, annealing at 55 °C for 30 seconds, a 30 second extension at 72 °C, and a final extension for 5 minutes at 72 °C. The library DNA then was purified using the Agencourt® AMPure® XP Reagent. Each sample was quantified and normalized prior to pooling. The DNA library pool was heat denatured before loading on the MiSeq reagent cartridge and on the MiSeq instrument. Automated cluster generation and paired-end sequencing with dual reads were performed per the manufacturer’s instructions.
Microbial Classification
Preprocessing of 16S rRNA Gene Sequences
Raw Illumina base call output (BCL) obtained from the MiSeq were converted, but not demultiplexed, to paired-end fastq files using CASAVA26. The resulting paired-end fastq files were joined into single-end reads using fastq-join27,28. Quality filtering was applied to the output of fastq-join requiring that greater than 80% of the base pairs be specified with a quality score of at least 25 for a read to be retained. The quality filtered reads were then demultiplexed. Reads whose index sequence was not an exact match to the specified barcode were eliminated (Table 1). Demultiplexed reads followed the QIIME29 split_libraries.py output convention and were suitable for subsequent analysis.
Demultiplexed 16S rRNA gene sequence reads were clustered into closed-reference Operational Taxonomic Units (OTUs) against the GreenGenes database30 using QIIME. For QIIME closed-reference picking, OTUs were picked with UCLUST at a similarity threshold of 0.9731. As a result, 8,375 OTUs were clustered with 8,373 classified at the phylum level, 4,052 classified at genus level and 0.23% reads remaining unclassified.
OTU count tables were then normalized as follows:
Equation (1) minimizes differences in the impact of adding the pseudo-count of 1 to each sample. OTUs absent in more than 75% of the samples were discarded.
In order to ensure that our method of normalization or our use of closed-reference OTUs did not unduly bias our results, we performed and additional analysis (Supplementary Figures S1–S3), using QIIME open-reference picking and rarefication to 10,000 sequences. In our QIIME open-reference picking pipeline, OTUs were picked with the method uclust at a similarity threshold of 0.97. OTUs with cluster less than 5 sequences were discarded. As a result, 18,162 OTUs were clustered with 15,719 of these classified at phylum level and 6,378 classified at genus and 2.16% of the reads remaining unclassified. The OTU table was then rarefied to 10,000 reads per sample. Samples with less than 10,000 reads were discarded and OTUs absent in more than 75% of the samples were discarded. OTU counts and taxonomic assignments using rarefied samples counts were then log-10 normalized with a pseudo-count of 1.
WGS sequences were also assigned taxonomy using Kraken and the taxonomic calls were normalized (Equation (1))32.
WGS Functional Classification
Paired end FASTQ files containing WGS sequences were converted to FASTA format. After filtering sequences mapping to the human genome forward WGS sequence reads were then run against the KEGG protein database33,34 using BLAST35. BLAST hits that had an e-value of 1 × 10−3 were kept. KEGG pathway abundances were calculated using HUMAnN36. KEGG gene families and pathways which were not present in at least 20% of the samples were removed (Table 2) and counts were normalized (Equation (1)).
Multidimensional Scaling (MDS)
Multidimensional scaling (MDS) was performed on normalized counts data generated by RDP classifier or Kraken (microbial classification) and BLAST (functional classifications) using Bray-Curtis dissimilarity. The R package “vegan”37 was used to calculate the MDS axes.
Statistical Analysis
Descriptive statistics of mean (standard deviation) for continuous variables and frequencies for categorical variables were derived for characteristics of the study participants. For the analysis of 16S rRNA amplicon and whole-genome metagenome sequencing data, the linear mixed effects model implemented the function “lme” from the R package “nlme” to evaluate the amount of variance due to stool vs. swab measures by controlling for time of sample collection. The p-values were generated from an ANOVA of the mixed linear models.
In this model (Equation (2)), the sample type (stool or swab (or mucosa for WGS sequences)), and time point are fixed effects while participant (ID of participant) is a random effect. We also evaluated the treatment effect (magnesium vs placebo) using a model similar to Equation (2) with “treatment” as an additional independent variable. Because there was no overall treatment arm effect, treatment was removed from all final models. The analysis was conducted for the first 15 MDS axes, all taxa and all KEGG gene families/pathways. ANOVA was used on the mixed effects models to test the null hypothesis that sample type and time point did not contribute to the model. In this discovery analysis, the false discovery rate (FDR) was set at 10% to adjust for multiple comparisons38. To determine differences in the amount of aerobic versus anaerobic bacteria in swab and stool samples we used a chi-square test of independence. Bacteria were labeled anaerobic or aerobic according to Bergey’s Manual of Systematic Bacteriology.
Code Availability
All R code and taxonomic tables used for this implementation is available in the GitHub repository and can be found here: https://github.com/rbarner/swabVsStool.
Data availability
The sequence reads (16S rRNA amplicon and whole-genome shotgun reads) used is available on the NCBI Short Read Archive and can be accessed with the accession code https://www.ncbi.nlm.nih.gov/bioproject/PRJNA397450.
Ethics approval
Written informed consent was obtained from all study participants, and the parent study and study protocol were approved by the Institutional Review Board at Vanderbilt University Medical Center.
Availability of data and material
The datasets generated and/or analyzed during the current study are available in the Github repository, https://github.com/rbarner/swabVsStool.
Results
Comparison of Taxa from 16S rRNA Amplicon Sequencing between Stool and Swab Samples
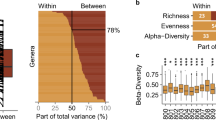
In a cohort recruited from an on-going NIH clinical study on the prevention of colorectal cancer (Supplementary Table S1), we collected stool and swab samples at two time points on average three months apart (see methods). We found substantial areas of similarity and differences between stool and swab samples based on the MDS ordination of 16S rRNA amplicon sequencing data (Fig. 1). The first two MDS axes (which accounted for almost 27% of the total variation of the microbial communities in the samples) showed nearly entirely distinct clusters between the stool (red symbols) and swab (blue symbols) (Fig. 1a). However, when comparing stool versus swab on two other MDS axes (Fig. 1b), there was a lack of distinct clusters. While the first MDS shows a difference between stool and swab that is consistent across all participants (Fig. 1c), the fourth MDS axis is much more influenced by each individual and appears to be less dependent on sample type (Fig. 1d). Also, to determine if there were significant differences in MDS clusters by sample origin, an analysis of variance was conducted using the function “adonis” in the R package “vegan”. This test showed that there is a significant difference between swab and stool in the dissimilarity matrix of the family level taxonomy counts (p = 8.01 × 10−6). To test whether the observed differences by sample type or participant were statistically significant, a linear mixed effects model was used with fixed effects for time point and sample type and a random effect for participant (Table 3). From the phylum to the OTU level, the first MDS axis was consistently associated with sample type (stool vs. swab). However, many other MDS axes had highly statistically significant effects for participant (Fig. 2) while showing no difference for sample type. This suggests that some taxa are highly specific to sample type within the colorectum (stool vs. swab) while other taxa are detectable with both sampling methods.

Multidimensional scaling (MDS) of closed-reference OTUs classified at the family level using 16S rRNA gene sequence reads. There are four samples (two each of stool and swab) from each of the 60 participants in our study colored by sample origin (red is stool and blue is swab). Repeated samples collected from individuals were collected with an average separation of 3 months. The distinct separation of colors shows that there is separation by sample type in MDS axis 1 and MDS axis 2 (a,c) but not in MDS axes 3 and 4 (b). However, MDS axis 4 shows strong clustering by participant (d).

The first 15 MDS axes were regressed against sample type (swab or stool), participant ID and time point. The −log10 (p-value) for the null hypothesis that sample type, participant ID and time point have no impact on the MDS axes are all shown. While there are significant differences in the first MDS axis in stool vs swab samples, the MDS axes thereafter are significantly different between the participants. Taxonomic calls were based on QIIME closed-referenced OTU picking against GreenGenes database.
In linear mixed effects models at the family level, 24 of 48 families were statistically significantly different between stool and swab samples while the variation in the logged abundance of 40 of 48 families showed significant variation due to the participant in which the sample originated (Table 4). There was substantial taxa by taxa variation (Fig. 3) in that there are families that vary by 1) sample type but not participant (e.g. Thermaceae), 2) participant but not sample type (e.g. Desulfovibrionaceae), or 3) both participant and sample type (e.g. Enterobacteriaceae) (Supplementary Figure S4). In addition, based on a chi-square test of independence, there was a statistically significant higher proportion (p = 0.02) of facultative aerobic genera that were significantly more abundant in swab samples than in stool samples (e.g. Acinetobacter, Anoxybacillus, and Geobacillus; Supplementary Table S4) consistent with a decreasing aerobic microbiota gradient from the mucosa to the lumen of the colorectum. This finding was reproduced using open-reference OTU data (p = 0.03). At species-level resolution (with WGS sequences) we observed that bacteria associated with colorectal tumors in previous studies39 (Escherichia coli and Fusobacterium nucleatum) were of higher relative abundance in swab than stool. There were also statistically significant differences in other bacteria according to the sample type (e.g. Bifidobacterium longum, Bacteroides fragilis) (Supplementary Table S5). Results using open-reference OTUs rarified to 10,000 reads show similar findings as data using relative abundance on closed-reference OTUs Supplementary Tables S2 and S3 and Supplementary Figures S1–S3 and S5. We also analyzed the differences in swab versus stool of each of the taxa using a non-parametric Wilcoxon test with taxon abundance as the dependent variable and sample source (swab versus stool) as the independent variable. These results were similar to those using the mixed models supporting the use of mixed models in this analysis (Supplemental Figure S6) suggesting that the assumptions of parametric models do not drive our results.

For each taxa at the family level present in at least 25% of samples, p-values for a null hypothesis of no difference by stool vs. swab vs. by participant. Red symbols are taxa that have a p-value that is significant at a 10% false discovery rate. Taxa higher in swab than stool have a negative x coordinate and taxa higher in stool than swab have a positive x-coordinate. Data was generated using closed-reference OTUs classified at the family level using 16S rRNA gene sequence reads.
Comparison of WGS Functional Classifications between Stool, Swab, and Mucosa Samples
To determine if sample type was distinct in microbial functions, we performed WGS on 50 participants including 100 stool samples, 28 rectal swabs, and 16 mucosa samples. We found pronounced differences in the functional pathways between the sample types based on MDS ordination for KEGG gene families using either all sample types including mucosa samples (Fig. 4) or using only stool and swab samples (Supplementary Figure S6), although stool and swab samples appear to be more closely related to each other than to mucosal biopsy samples. We also found that there was separation by sample type when we assigned taxonomy to WGS sequences (including mucosa samples (Supplementary Figure S7) and only including stool and swab samples (Supplementary Figure S8). In general, all of the KEGG pathways at Level 1 (Supplementary Table S6; Supplementary Figure S9) and Level 2 (Supplementary Table S7) were highly different between the sample types while there were only a few statistically significant differences in abundances of functional categories between participants. This observation is consistent with functional pathways being more similar across individuals than taxonomic assignments (Supplementary Figure S10) as has been observed in other studies22.

Plot of first two coordinates (a) and MDS3 vs MDS 4 (b) of an MDS ordination of the KEGG gene family abundance table for WGS sequence reads from swab samples (blue triangles), stool samples (red circles) and tissue samples (purple squares). The distinct separation of colors shows that there is separation by sample type in the first and third MDS axes. MDS axes plotted by participant ID show strong separation by sample type for MDS 1 (c) and by participant and sample type for MDS 3 (d).
Discussion
The primary purpose of this analysis was to determine similarities and differences in the microbial communities of three different types of samples that can be used to assess the gut microbiome: rectal swab samples, stool samples, and normal rectal mucosa samples. This is the first large study to evaluate the longitudinal short-term stability of the microbiota within mucosal biopsies and rectal swabs. We observed distinct differences in the microbiome composition of swab or stool samples for some, but not all, taxa. We found that differences between different sample types extends to functional categorization with whole-genome shotgun sequencing. However, the individual signature of participants was also observed and was largely stable between two time points. Thus, we found that while the distribution of some taxa was associated with these different sampling techniques, other taxa largely reflected individual differences in the microbial community that were insensitive to sampling technique.
A few studies have directly compared the microbiome composition of rectal swabs with rectal mucosal and/or stool samples12,16,23. From these and our study, there is increasing evidence that the microbiome composition within the colorectum varies from the mucosa to the lumen, and that swab samples may capture a different microbiome composition profile than either mucosa or stool. However, previous studies reported on small sample sizes. In one such small study (n = 11) of rectal swabs and normal rectal mucosa from individuals with and without a history of colorectal adenoma, bacterial α-diversity was higher in swabs than in mucosa and the swabs also had higher abundances of Eubacteria and Lactobacillus spp.16. In our study, we also found Lactobacillaceae was more abundant in swab than stool. Another study, which compared select phyla in rectal swabs with stool samples in 10 patients with IBD, observed a high intra-subject correlation of Bacteroidetes abundance and Shannon diversity measures while there was little difference by sample type among the subjects, which is consistent with our finding of no statistically significant difference between stool and swab abundances for this phylum23. Unlike our study, they did not observe a high correlation in a collective measure of Actinobacteria, Firmicutes, Fusobacteria, and Verrucomicrobia whereas we did find significant differences when these phyla were evaluated individually. In a study of swab and stool samples from 7 pediatric patients and serial stool and rectal mucosa samples from 10 adult patients, differences in taxa were primarily due to differences between mucosa and stool samples with rectal swabs being most similar to the mucosal samples in taxa composition12. They further identified 6 genera, which they observed only in mucosa and swab samples and not in stool samples. We observed 3 of 6 of these genera (Anaerococcus, Murdochiella, and Peptoniphilus) to be present in both swab and stool samples in our study which had a larger sample size, although, in general, the relative abundances were lower in stool versus swab. This suggests the importance of sufficient sample sizes to capture rarer taxa regardless of sample type as well as the possibility that the degree to which mucosally associated bacteria slough off into the lumen may vary across individuals due to individual differences or bacterial composition. We also found the similarities between swab and stool samples were highly taxa-specific even within the same phylum or family. Another potential explanation for the small differences between our studies is that the previous study used swab and mucosal samples from different individuals which could have confounded inter-niche differences with inter-person differences. As our study did, this previous study also found evidence of a decreasing aerobic microbiota gradient from the mucosa to the lumen of the colorectum12.
In addition to evaluating the sample type, we also considered whether there was variability in the composition over time by evaluating samples collected 3 months apart. We found variability in composition was almost entirely explained by the sample type and inter-person variability indicating that the microbiome composition is relatively stable in all of the sample types during this period of time regardless of season of collection. To our best knowledge, no previous study has evaluated the stability of the microbiota within mucosal biopsies or rectal swabs. However, our findings are largely consistent with other studies which have evaluated repeated stool collections19,22,40. In a small study (n = 5) with multiple stool collections across 8 or more years, inter-individual variation was substantially greater than intra-person variability across time although some taxa appeared to have more variation than other taxa18. Nonetheless, most of the variation was due to changes in the species abundance versus a presence or absence of the species indicating that an individual-specific microbiota pattern may exist. This was also observed in a study evaluating stool samples collected a year apart (n = 43) in which intra-person variation in the stool metagenome was much smaller than inter-person variability and individual-specific variation patterns over time also remained stable40.
It has been reported in several studies that, despite large inter-person differences in the taxa composition of the microbiome, inter-person variability in the gene composition, and, thus the functional activity, of the microbiota is much less10,18,19,20,21,22. However, few studies have evaluated differences in the gene composition of the microbiota between samples types within the colorectum. In our study, we found extensive variation in the samples between KEGG pathways due to sample type (stool, swab, rectal mucosa). In a small study of inferred gene content from 16S rRNA analysis comparing rectal swabs (n = 7), stool (n = 28), and rectal mucosa (n = 10) from different individuals, Albenberg et al. reported that genes in carbohydrate metabolism are in lower abundance in swab vs. stool or mucosa12. We found that the KEGG pathway carbohydrate metabolism was highest in stool and lowest in mucosa with rectal swabs being more similar in relative abundance to stool. This pathway included gene families mapping to enzymes involved in the degradation of colonic mucus such as sialate O-acetylesterase and N-acetylneuraminate lyase. In general, this finding of a relative abundance for swab falling between stool and mucosa was similar for most pathways and gene families, particularly those for metabolism. These findings further indicate the choice of stool, swab, and mucosa samples will measure different aspects of the microbiota within the colorectum.
There are some limitations to our study. We conducted this study among individuals with a history of colorectal polyps. Thus, our findings are generalizable insofar as the gut microbiome characteristics across sample type are consistent between individuals with and without a history of polyps. The sample size, particularly for the metagenomics analysis of colorectal mucosa, is modest and we may thus have had insufficient statistical power to observe differences. However, the comparisons of stool and swab were more robust and the largest to-date. For analysis of the stability of the measurements, samples were collected approximately three months apart and so we could not evaluate stability over a longer time period. However, we were able to capture variability in season of collection. Future studies with multiple repeated collections are needed to further ascertain whether the short-term reliability holds up longitudinally. Lastly, we cannot exclude the possibility of human contamination in the metagenomics analysis of colorectal mucosa.
There are also several strengths to consider. Unlike some previous studies, by including sample types from within the same individual, we were able to evaluate the relative contributions of inter-person vs. inter-niche differences. We were also able to evaluate differences across time by including samples from two time points. Finally, we were able to collect swab and mucosa samples from individuals who had not undergone a bowel cleansing preparation.
Conclusions
In summary, despite structural differences in the microbial communities being driven largely by the sample type, the individual signature of each participant was still evident and was also stable over time. It thus seems, at least in this southern US population, a single spot sample may be sufficient to capture the microbial signature of an individual. Future studies which compare the microbiome findings with markers of disease are needed to better understand which type of sample may be the most appropriate for the research question.
References
Manichanh, C. et al. Reduced diversity of faecal microbiota in Crohn’s disease revealed by a metagenomic approach. Gut 55, 205–211 (2006).
Willing, B. P. et al. A pyrosequencing study in twins shows that gastrointestinal microbial profiles vary with inflammatory bowel disease phenotypes. Gastroenterology 139, 1844–1854.e1 (2010).
Boleij, A. & Tjalsma, H. Gut bacteria in health and disease: a survey on the interface between intestinal microbiology and colorectal cancer. Biol Rev Camb Philos Soc 87, 701–730 (2012).
Karlsson, F. H. et al. Symptomatic atherosclerosis is associated with an altered gut metagenome. Nat Commun 3, 1245 (2012).
Paun, A. & Danska, J. S. Modulation of type 1 and type 2 diabetes risk by the intestinal microbiome. Pediatr Diabetes 17, 469–477 (2016).
Clarke, G. et al. Minireview: Gut microbiota: the neglected endocrine organ. Mol. Endocrinol. 28, 1221–1238 (2014).
Lepage, P. et al. A metagenomic insight into our gut’s microbiome. Gut 62, 146–158 (2013).
Azcárate-Peril, M. A., Sikes, M. & Bruno-Bárcena, J. M. The intestinal microbiota, gastrointestinal environment and colorectal cancer: a putative role for probiotics in prevention of colorectal cancer? Am. J. Physiol. Gastrointest. Liver Physiol. 301, G401–424 (2011).
Vipperla, K. & O’Keefe, S. J. The microbiota and its metabolites in colonic mucosal health and cancer risk. Nutr Clin Pract 27, 624–635 (2012).
Stearns, J. C. et al. Bacterial biogeography of the human digestive tract. Sci Rep 1, 170 (2011).
Eckburg, P. B. et al. Diversity of the human intestinal microbial flora. Science 308, 1635–1638 (2005).
Albenberg, L. et al. Correlation between intraluminal oxygen gradient and radial partitioning of intestinal microbiota. Gastroenterology 147, 1055–1063.e8 (2014).
Espey, M. G. Role of oxygen gradients in shaping redox relationships between the human intestine and its microbiota. Free Radic. Biol. Med. 55, 130–140 (2013).
Wu, G. D. et al. Linking long-term dietary patterns with gut microbial enterotypes. Science 334, 105–108 (2011).
Sonnenburg, J. L., Angenent, L. T. & Gordon, J. I. Getting a grip on things: how do communities of bacterial symbionts become established in our intestine? Nat. Immunol. 5, 569–573 (2004).
Araújo-Pérez, F. et al. Differences in microbial signatures between rectal mucosal biopsies and rectal swabs. Gut Microbes 3, 530–535 (2012).
Ukhanova, M. et al. Gut microbiota correlates with energy gain from dietary fibre and appears to be associated with acute and chronic intestinal diseases. Clin Microbiol Infect 18(Suppl 4), 62–66 (2012).
Costello, E. K. et al. Bacterial community variation in human body habitats across space and time. Science 326, 1694–1697 (2009).
Rajilić-Stojanović, M., Heilig, H. G. H. J., Tims, S., Zoetendal, E. G. & de Vos, W. M. Long-term monitoring of the human intestinal microbiota composition. Environ. Microbiol. https://doi.org/10.1111/1462-2920.12023 (2012).
Human Microbiome Project, C. A framework for human microbiome research. Nature 486, 215–221 (2012).
Human Microbiome Project, C. Structure, function and diversity of the healthy human microbiome. Nature 486, 207–214 (2012).
Claesson, M. J. et al. Composition, variability, and temporal stability of the intestinal microbiota of the elderly. Proc. Natl. Acad. Sci. USA 108(Suppl 1), 4586–4591 (2011).
Budding, A. E. et al. Rectal swabs for analysis of the intestinal microbiota. PLoS ONE 9, e101344 (2014).
Edwards, U., Rogall, T., Blöcker, H., Emde, M. & Böttger, E. C. Isolation and direct complete nucleotide determination of entire genes. Characterization of a gene coding for 16S ribosomal RNA. Nucleic Acids Res. 17, 7843–7853 (1989).
Fierer, N., Hamady, M., Lauber, C. L. & Knight, R. The influence of sex, handedness, and washing on the diversity of hand surface bacteria. Proc. Natl. Acad. Sci. USA 105, 17994–17999 (2008).
Hosseini, P., Tremblay, A., Matthews, B. F. & Alkharouf, N. W. An efficient annotation and gene-expression derivation tool for Illumina Solexa datasets. BMC Res Notes 3, 183 (2010).
Aronesty, E. ea-utils: Command-line tools for processing biological sequencing data (2011).
Aronesty, E. Comparison of Sequencing Utility Programs. The Open Bioinformatics Journal 7, 1–8 (2013).
Caporaso, J. G. et al. QIIME allows analysis of high-throughput community sequencing data. Nat. Methods 7, 335–336 (2010).
DeSantis, T. Z. et al. Greengenes, a chimera-checked 16S rRNA gene database and workbench compatible with ARB. Appl Environ Microbiol 72, 5069–5072 (2006).
Edgar, R. C. Search and clustering orders of magnitude faster than BLAST. Bioinformatics 26, 2460–2461 (2010).
Wood, D. E. & Salzberg, S. L. Kraken: ultrafast metagenomic sequence classification using exact alignments. Genome Biol. 15, R46 (2014).
Bates, D., Mächler, M., Bolker, B. & Walker, S. Fitting Linear Mixed-Effects Models usinglme4. arXiv:1406.5823 [stat] (2014).
Kanehisa, M. & Goto, S. KEGG: kyoto encyclopedia of genes and genomes. Nucleic Acids Res 28, 27–30 (2000).
Kanehisa, M. et al. Data, information, knowledge and principle: back to metabolism in KEGG. Nucleic Acids Res. 42, D199–205 (2014).
Altschul, S. F., Gish, W., Miller, W., Myers, E. W. & Lipman, D. J. Basic local alignment search tool. J Mol Biol 215, 403–410 (1990).
Oksanen, J. et al. vegan: Community Ecology Package. (2016).
Benjamini, Y. & Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. Journal of the Royal Statistical Society. Series B (Methodological) 57, 289–300 (1995).
Brennan, C. A. & Garrett, W. S. Gut Microbiota, Inflammation, and Colorectal Cancer. Annu. Rev. Microbiol. 70, 395–411 (2016).
Schloissnig, S. et al. Genomic variation landscape of the human gut microbiome. Nature 493, 45–50 (2013).
Acknowledgements
The authors thank the research staff and investigators who have contributed to the Personalized Prevention of Colorectal Cancer Trial, the study participants who contributed their time and biospecimens for research, and Dr. Jay Fowke for sharing his protocol for rectal biopsy collection. This study was supported by grants R03CA183019 (MJS), R01CA149633 (QD and CY), and R01DK110166 (QD and MJS), as well as the Ingram Cancer Center Endowment Fund. Data collection, sample storage and processing for this study were partially conducted by the Survey and Biospecimen Shared Resource, which is supported in part by P30CA68485. Clinical visits to the Vanderbilt Clinical Research Center were supported in part by the Vanderbilt CTSA grant UL1 RR024975 from NCRR/NIH. The UNC Microbiome Core Facility is supported in part by the NIH/National Institute of Diabetes and Digestive and Kidney Diseases grant P30DK34987. The parent study data were stored in Research Electronic Data Capture (REDCap) and data analyses (VR12960) were supported in part by the Vanderbilt Institute for Clinical and Translational Research (UL1TR000445). The content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
Q.D., C.Y., and M.J.S. contributed to study conception, design, and supervision. Q.D., C.Y., X.Z., H.J.M., R.M.N., D.L.S., M.A.A.P., and M.J.S. contributed to acquisition of data. X.Z. and M.J.S. provided administrative, technical, or material support. R.B.J., X.Z., E.M., Q.D., S.S., C.Y., A.A.F., and M.J.S. contributed to analysis and interpretation of data. All authors contributed to writing, review, and/or revision of the manuscript and approved the final manuscript. M.J.S. is the guarantor of the submitted manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jones, R.B., Zhu, X., Moan, E. et al. Inter-niche and inter-individual variation in gut microbial community assessment using stool, rectal swab, and mucosal samples. Sci Rep 8, 4139 (2018). https://doi.org/10.1038/s41598-018-22408-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-22408-4
This article is cited by
-
Proportion-based normalizations outperform compositional data transformations in machine learning applications
Microbiome (2024)
-
Validation of method for faecal sampling in cats and dogs for faecal microbiome analysis
BMC Veterinary Research (2023)
-
A consortia of clinical E. coli strains with distinct in vitro adherent/invasive properties establish their own co-colonization niche and shape the intestinal microbiota in inflammation-susceptible mice
Microbiome (2023)
-
Rectal swabs as a viable alternative to faecal sampling for the analysis of gut microbiota functionality and composition
Scientific Reports (2023)
-
Designs and methodologies to recreate in vitro human gut microbiota models
Bio-Design and Manufacturing (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
