
Abstract
There is a growing consensus that genetic variation in candidate genes can influence cancer progression and treatment effects. In this study, we genotyped the rs9642880 G > T polymorphism using DNA isolated from blood samples of 271 hepatocellular carcinoma (HCC) patients who received radiotherapy treatment. We found that patients who carried the GT or TT genotypes had significantly shorter median survival times (MSTs) compared to patients with the GG genotype (14.6 vs.21.4 months). The multivariate P value was 0.027, the hazard ratio (HR) was 1.38, and the 95% confidence interval was 1.04–1.84. Further analysis revealed that patients with the variant genotypes had an increased risk of poor tumour response to radiotherapy (P = 0.036 and 0.002 for stable disease and progressive disease, respectively) and higher incidence of multiple intrahepatic lesions (P = 0.026) and BCLC C stage (P = 0.027). Moreover, further stratified survival analyses revealed that at least radioresponse and BCLC stage contributed to the association between the rs9642880 G > T polymorphism and survival of HCC patients in this study (P value, 0.017 vs 0.053 for BCLC C stage vs B stage; 0.011 vs 0.531 for radioresponse SD + PD vs CR + PR). These results illustrate the potential association between rs9642880 G > T and survival in HCC patients who received radiotherapy treatment.
Similar content being viewed by others

Introduction
Hepatocellular carcinoma (HCC) is one of the most common liver malignancies, and its incidence is increasing in most parts of the world. Surgical resection is the most common treatment choice for HCC, but for a considerable number of cases, surgical resection is not suitable because of factors such as large tumour size, concomitant liver cirrhosis, or portal vein tumour thrombosis. In these inoperable HCC cases, radiotherapy can be an effective treatment option1,2.
In clinical radiobiology, HCC is an early-responding tissue with an α/β ratio >10 Gy, which means it is categorized as a radiation-sensitive tissue. However, historically, HCC radiotherapy has been limited by the lack of precise patient imaging, the inability to quantify the dose received by a given volume of tissue, and outmoded radiation therapy (RT) techniques. More recently, the development of modern RT techniques, such as helical tomotherapy (HT), has made radiation therapy for HCC a safe and effective option for many patients.
Genetic variations, such as single nucleotide polymorphisms (SNPs) in candidate genes, have been proposed to affect the survival outcomes in cancer patients3,4. In this study, we investigated the rs9642880 G > T polymorphism, which is located on 8q24, only 30 kb upstream of the c-MYC(MYC) gene. c-MYC is a transcription factor that regulates many basic cellular processes, such as cell proliferation, cell transformation, and apoptosis5,6, and the deregulation of c-MYC plays a critical role in carcinogenesis and tumour progression.
Additionally, according to previous studies, c-MYC has been revealed to be a radiosensitive locus7, and it has been found that the rs9642880 G > T polymorphism could influence the expression of c-MYC8. The overexpression of c-MYC is considered to be associated with promoting radioresistance in nasopharyngeal carcinomas9; therefore, we hypothesize that the c-MYC rs9642880 G > T polymorphism is associated with the survival of HCC patients who received radiation therapy. To confirm this hypothesis, we evaluated the frequencies of the rs9642880 G > T polymorphism in HCC patients who received radiotherapy treatment and assessed survival outcome and the impact of genotype for this polymorphism on clinical characteristics.
Results
Patient demographic and clinical information and outcomes
The demographic information and clinical characteristics of the 271 HCC patients included in this study are summarized in Table 1. The study cohort was composed of 227 men and 44 women, and the median age was 56 years (ages ranged from 26 to 87 years). Additional demographic information and clinical characteristics included Karnofsky performance status(KPS), alpha-fetoprotein(AFP), Child-Pugh classification, Barcelona Clinic Liver Cancer stage(BCLC stage), tumour size, intrahepatic tumour number, prior treatments, radiation technique, lymph node metastases(LN metastases), distant metastases, smoking status and drinking status (Table 1). At the end of the study, 53 patients (19.6%) were still alive. However, among those patients, only 35 were available for follow-up. Eight patients were lost to death unrelated to HCC, and ten patients were lost due to loss of contact. Of the 218 patients (80.4%) who died over the course of the study, 159 (72.9%) died from hepatic failure due to hepatic decompensation or tumour progression. Severe lung, brain, or bone metastases were observed in 59 patients (27.1%). Other causes of death included gastrointestinal bleeding in four patients and systemic failure in two patients.
Associations between patient characteristics and HCC survival outcomes
Analyses of potential predictors of survival in the 271 HCC patients are summarized in Table 2. A Cox proportional hazards regression model was used to identify predictors of survival. In the univariate analysis, we found that alanine aminotransferase (ALT, P = 0.017), aspartate aminotransferase (AST, P = 0.018), AFP (P = 0.031), Child-Pugh classification (P = 0.001), BCLC stage (P = 0.003), intrahepatic tumour number (P < 0.001), external beam radiotherapy (EBRT) dose (P = 0.029), and radiation technique (P = 0.025) were significantly associated with overall survival(OS) (Table 2). Based on these findings, factors that significantly predicted survival in the univariate analysis were used to adjust the multivariate Cox regression to eliminate possible interference with the main effects of the rs9642880 G > T polymorphism on HCC prognosis (Table 3).
Associations between rs9642880 G > T and HCC survival outcomes
The rs9642880 G > T genotypes were identified using the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) assay and verified by direct sequencing (Fig. 1). There were 105 HCC patients with the GG genotype, 130 patients with the GT genotype, and 36 patients with the TT genotype. As shown in Table 3, rs9642880 G > T was significantly associated with OS in HCC patients with radiotherapy treatment (log-rank P = 0.003). Patients who carried the TT variant genotype had significantly shorter median survival times (MSTs) compared with those with the GG genotype (13.0 vs.21.4 months), with a univariate P value of 0.003 (HR = 1.96; 95% confidence interval [CI] 1.26–3.02) and a multivariate P value of 0.026 (HR = 1.69; 95% CI 1.07–2.68). The MST of patients who carried the GT or TT genotype was shorter than that of patients with the GG genotype (14.6 vs. 21.4 months), with a univariate P value of 0.001 (HR = 1.58, 95% CI 1.20–2.09) and a multivariate P value of 0.027 (HR = 1.38; 95% CI 1.04–1.84) (Table 3). These results demonstrate that patients with at least one T allele (GT or TT genotypes) had significantly poorer survival compared with those carrying the GG homozygous genotype (log-rank P = 0.001, Fig. 2).

rs9642880 G > T genotypes were identified using a polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) assay, and the results were confirmed using direct sequencing. (a) Representative genotypes based on the PCR-RFLP assay. L1, L2, and L7 were identified as having the GG genotype; L3, L4, L5, L6, and L8 were identified as having the GT genotype; and L9 was identified as having the TT genotype. The figure of the full-length agarose gel and figure with white background and black product bands is included in the Supplementary Figs 2a and 3a; (b,c and d) Results of direct DNA sequencing of L1, L3, and L9, respectively.

Kaplan-Meier survival curves of 271 HCC patients based on rs9642880 G > T genotype (GT + TT vs GG).
Association between the rs9642880 G > T polymorphism and the clinical characteristics of HCC patients
We also analysed the association between the rs9642880 G > T polymorphism and the clinical characteristics of HCC patients. In contrast to patients with the GG genotype, patients with GT or TT genotypes had a higher incidence of multiple intrahepatic lesions (P = 0.026) and BCLC C stage (P = 0.027) and an increased risk of stable disease (SD) or progressive disease (PD) after tumour radiotherapy (P = 0.036 and P = 0.002, respectively). No significant correlation was observed with other clinical characteristics (Table 4).
Stratified survival analyses for rs9642880 G > T
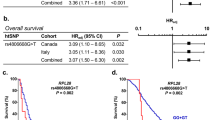
To determine the clinical characteristics that contribute to the association between the rs9642880 G > T polymorphism and survival in HCC patients who received radiation therapy in the study, stratified survival analyses by intrahepatic tumour number (solitary vs multiple), BCLC stage (B stage vs C stage), and radioresponse (CR + PR vs SD + PD) with the rs9642880 genotypes were carried out. The log-rank P value was 0.063 in the solitary subgroup (Fig. 3a), 0.094 in the multiple subgroup (Fig. 3b), 0.053 in the BCLC B stage subgroup (Fig. 3c), 0.017 in the BCLC C stage subgroup (Fig. 3d), 0.531 in the CR + PR radioresponse subgroup (Fig. 3e), and 0.011 in the SD + PD radioresponse subgroup (Fig. 3f). A significantly poor survival status associated with the variant genotypes was found in BLBC C stage patients and poor radioresponse patients but not in BLBC B stage and good radioresponse patients (P value, 0.017 vs 0.053 for BCLC C stage vs B stage; 0.011 vs 0.531 for radioresponse SD + PD vs CR + PR). However, no significant differences related to intrahepatic tumour number were found; these results indicate that at least radioresponse and BCLC stage contribute to the association between the rs9642880 G > T polymorphism and survival of HCC patients who received radiation therapy in the study.

Stratified Kaplan-Meier survival curves of HCC patients who received radiotherapy, based on the rs9642880 G > T genotype. (a) Kaplan-Meier survival curves of HCC patients with solitary intrahepatic tumour; (b) Kaplan-Meier survival curves of HCC patients with multiple intrahepatic tumours; (c) Kaplan-Meier survival curves of HCC patients in BCLC B stage; (d) Kaplan-Meier survival curves of HCC patients in BCLC C stage; (e) Kaplan-Meier survival curves of HCC patients with CR or PR radioresponse; (f) Kaplan-Meier survival curves of HCC patients with SD or PD radioresponse.
Association between the rs9642880 G > T polymorphism and c-MYC expression in HCC cell lines
We analysed the genotype of the rs9642880 G > T polymorphism in different HCC cell lines, including MHCC97H, HCCLM3,HepG2, Hep3B and SMMC-7721, and found that cell lines MHCC97H and HCCLM3 had the GG genotype, HepG2 had the GT genotype, and Hep3B and SMMC-7721 had the TT genotype (Supplementary Fig. 1a). Additionally, we quantified the c-MYC mRNA levels in those HCC cell lines using a quantitative real-time PCR assay, and the results showed that the cell lines with the TT genotype (Hep3B and SMMC-7721) had higher c-MYC mRNA levels compared with the cell line with the GT genotype (HepG2); moreover, the cell lines with the GG genotype (MHCC97H and HCCLM3) had the lowest c-MYC mRNA level (Supplementary Fig. 1b) of the five cell lines. These results were confirmed at the protein level by western blot assays (Supplementary Fig. 1c) and suggested that the rs9642880 T allele was associated with the overexpression of c-MYC in HCC cell lines.
Discussion
Currently, genome-wide association studies are widely undertaken to develop more accurate diagnostic and therapeutic strategies for human diseases, including cancer10,11. In the present study, we investigated the associations between the c-MYC rs9642880 G > T polymorphism on 8q24 and survival in 271 HCC patients following radiotherapy treatment. We found that the presence of at least one T allele was significantly associated with an unfavourable survival outcome for HCC patients following radiation therapy. These results remained significant after adjusting for other potential survival-influencing factors. Moreover, further analyses revealed that three clinical characteristics were associated with the rs9642880 G > T polymorphism: tumour response to radiotherapy, intrahepatic tumour number and BCLC stage; patients with the GT or TT genotype had an increased risk of poor tumour response to radiotherapy and a higher incidence of multiple intrahepatic lesions and BCLC C stage. However, the further stratified analyses emphasized the contribution of radioresponse and BCLC stage, but not intrahepatic tumour number, to the association between the rs9642880 G > T polymorphism and survival of HCC patients. These findings indicate the potential association between rs9642880 G > T and the survival of HCC patients who received radiotherapy treatment.
The incidence of HCC is increasing in most parts of the world, and clinical data indicate that radiotherapy is a highly effective therapy1,12,13,14. However, we found that HCC patients at the same disease stage often have completely different outcomes following radiotherapy, which is believed to be due to individual variation in radiation sensitivity. There is an increasing consensus that radiation sensitivity is a genetic trait that involves the interactions of many genes15; thus, genetic variants may influence an individual’s radioresponse.
The underlying mechanism of radiotherapy is the production of irreparable DNA damage, which leads to cell death. Cells respond to DNA damage by activating DNA repair pathways, including cell cycle checkpoints and other cell cycle regulatory pathways. Therefore, the status of DNA damage or DNA repair pathways is one of the most important determinants of radiosensitivity16,17. Interestingly, c-MYC is involved in cell cycle checkpoint regulation. Wang and colleagues found that the overexpression of c-MYC activated DNA damage cell cycle checkpoints by upregulating the expression of the CHK1 and CHK2 checkpoint kinases in nasopharyngeal carcinomas, leading to the activation of DNA repair and ultimately resulting in radioresistance9.
The rs9642880 G > T polymorphism is a common variant that lies upstream of c-MYC on chromosome 8q2418,19.Various enhancers that can regulate the transcription of c-MYC are found in this region, and the rs9642880 G > T polymorphism has been reported to affect the expression of c-MYC in bladder cancer. It was found that c-MYC expression levels were significantly higher in individuals with the rs9642880 GT or TT genotype than in those with the GG genotype8, which is consistent with our analysis of c-MYC expression in HCC cell lines with different rs9642880 genotypes. Thus, the rs9642880 G > T polymorphism may influence radiosensitivity by altering c-MYC expression, ultimately leading to radioresistance. Moreover, c-MYC has been revealed to be a radiosensitive locus13, and genetic alteration in that region may influence radiosensitivity. In the present study, we confirmed that HCC patients with the rs9642880 GT or TT genotypes have poorer radioresponse. Further stratified analyses revealed that radioresponse contributed to the influence of the rs9642880 G > T polymorphism on survival.
c-MYC is a transcription factor that regulates many basic cellular processes, such as cell proliferation, cell transformation, and apoptosis5,6. Given its role in these basic cellular functions, the deregulation of c-MYC plays a critical role in carcinogenesis and tumour progression. For example, Kim et al. found that the c-MYC regulatory network accounts for similarities between embryonic stem and cancer cell transcription programs20. Additionally, Castro et al. reported that c-MYC activates GATA4, which leads to metastasis in lung adenocarcinoma21. In HCC, c-MYC is intimately involved in malignant progression; in particular, c-MYC has been implicated in driving the initial stages of hepatocarcinogenesis22 and is commonly overexpressed in HCC23. In this study, we found that patients with a GT or TT genotype at the rs9642880 SNP had higher incidences of multiple intrahepatic lesions and BCLC C stage. These findings may be explained by the potential overexpression of the oncogene c-MYC in the variant genotype. However, further stratified survival analyses revealed that only BCLC stage and not intrahepatic tumour number contributed to the association between the rs9642880 G > T polymorphism and survival of HCC patients. This suggests that BCLC stage has more impact than tumour number on HCC patient survival.
There were several limitations in our study. First, we could not rule out the possibility of selection bias in our study. However, there were no significant genotype distribution differences between the overall population and our HCC cohort6,24. Second, although we performed univariate analysis of predictors of survival in 271 HCC patients, and although significant survival prediction factors in the univariate analysis were used to adjust the univariate Cox regression results to eliminate possible interference with the main effects of rs9642880 G > T on HCC prognosis, some potential predictors of survival that were not included may still be a source of bias in the prognosis. Third, in the analyses of associations between rs9642880 G > T and clinical characteristics, there may exist interference among different clinical characteristics, although adjustment was performed.
In conclusion, the study illustrated the potential association between rs9642880 G > T and the survival of HCC patients who received radiotherapy treatment. This association may be attributed to the roles that the variant genotypes play in radioresponse and in the BCLC stage of HCC patients.
Methods
Study population
We retrospectively reviewed 271 HCC patients who received radiotherapy at Zhongshan Hospital between January 2009 and October 2014. The diagnosis of HCC was based on guidelines from the American Association for the Study of Liver Diseases25. Patients with Child-Pugh class C disease and patients who had a medical history of other cancers were excluded from our study. Clinical characteristics and demographic information were obtained from a review of the medical records. The study was approved by the Zhongshan Hospital Research Ethics Committee, and informed consent was obtained from each patient.
Therapies
For the 271 patients in the study, conventional external beam radiotherapy(EBRT) was delivered using three-dimensional conformal radiation therapy (3D-CRT) or helical tomotherapy (HT).Briefly, the patients were immobilized by a vacuum-formed mould, which roughly matched the shape of the patients. For HT patients, an anterior pressure plate was added to reduce respiration movement. Gross tumour volume included the whole intrahepatic tumour. Clinical target volume (CTV) denoted the gross tumour volume and an expanded margin of 5–10 mm, and the planning target volume added a margin of 7–10 mm to the CTV to compensate for geometric uncertainties. Treatment plans were established using TomoTherapy planning software, version 4.2 (TomoTherapy, Inc., USA) in HT patients and the XiO treatment planning system in 3D-CRT patients. A daily dose of 2 Gy was administered to every patient at five fractions per week, and the median total dose was 54 Gy (range of 31.2–60 Gy). As much of the normal liver was kept unirradiated as possible. When adverse effects or aggravated performance status occurred, a lower dose was delivered or radiotherapy was stopped.
SNP selection
c-MYC was identified as a radiosensitive locus. We searched for SNPs in the c-MYC enhancer region on 8q24 within the dbSNP database and found three SNPs (rs6983267, rs11986220 and rs9642880) that were previously identified as functional variants of enhancer activity. However, SNPs rs6983267 and rs11986220 are hundreds of kb distal to the c-MYC gene. In contrast, the rs9642880 G > T variant is located only 30 kb upstream of c-MYC. Therefore, we ultimately selected the rs9642880 G > T SNP for genotyping in our studies.
Follow-up and response evaluation
The median follow-up time for the cohort was 15.3 months, with a range of 1.5–76.6 months. Patients were advised to receive an initial follow-up examination approximately 1.5 months after the completion of EBRT. The examination included a CT scan, which was performed by doctors who were blinded to the study. Patients were monitored every three months thereafter. Tumour response was evaluated according to the new Response Evaluation Criteria in Solid Tumours (version 1.1)26. A complete response (CR) was defined as the complete disappearance of the intrahepatic tumour. A partial response (PR) was defined as a 50% reduction in intrahepatic tumour size. Progressive disease (PD) was defined as an increase of 25% in intrahepatic tumour size. Finally, stable disease (SD) was classified as any response between PR and PD.
Genotyping
Blood samples were collected from each subject and stored at −80 °C.Genomic DNA was isolated from peripheral blood lymphocytes using a QIAamp DNA Blood Mini Kit (Qiagen, Germany).The rs9642880 G > T genotypes were identified using a polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) assay according to the protocol described in our previous study27. Briefly, target fragments containing the rs9642880 site were amplified using the following primers: forward, 5′- CCACCACTCTCAGCCTTTTC-3′ and reverse, 5′-TGGGATTACAAGTGTGAACCTG-3′. The 203 bp PCR products were digested by the StyI-HF restriction enzyme (New England BioLabs, USA), and a 2% agarose gel electrophoresis was conducted to identify the rs9642880 genotypes. The genotypes were assessed as follows: the wild-type homozygotes (GG) produced one band at 203 bp; the variant homozygotes (TT) produced two bands at 135 and 68 bp; and the heterozygotes (GT) produced three bands at 203, 135, and 68 bp (Fig. 1a). PCR products from approximately 10% of the samples were randomly selected and verified by direct sequencing using an ABI 3730 DNA analyser (Applied Biosystems, USA), and the results were 100% concordant with the electrophoresis results (Fig. 1b,c,d).
Quantitative real-time PCR assay
Total RNA was isolated from cells using TRIzol reagent (Invitrogen, USA) according to the manufacturer’s protocol. The reverse transcription-polymerase chain reaction was performed with a ProFlex PCR system (Applied Biosystems, USA). Briefly, 800 ng total RNA was used for cDNA synthesis with a PrimeScript RT reagent kit (TakaraBio, Japan), and real-time PCR was performed with an ABI 7500 detection system (Applied Biosystems, USA) using HiffTM qPCR SYBR Green Master Mix (Shanghai YEASEN Biotechnology Co.Ltd., China). The expression of c-MYC was normalized to GAPDH expression using the 2−ΔΔCt method, and the primers for human c-MYC were as follows: 5-TCCCTCCACTCGGAAGGAC-3(forward) and 5-CTGGTGCATTTTCGGTTGTTG-3(reverse). The GAPDH primers were as follows: 5-CTGGGCTACACTGAGCACC-3(forward) and 5-AAGTGGTCGTTGAGGGCAATG-3(reverse).
Protein levels detected by Western blot analysis
Total protein was extracted from cells using Beyotime Cell Lysis Buffer for Western and IP (Beyotime, China) containing protease inhibitors. Proteins were separated by 8% SDS-PAGE and transferred to a methanol-activated PVDF membrane. The membrane was blocked for 1 h in 5% nonfat milk and subsequently probed with an antibody against human c-MYC (1:1500; Cell Signaling Technology, USA) at 4 °C overnight. β-Actin served as a loading control (1:1500; Beyotime, China). Membranes were washed three times for 5 min each with phosphate-buffered saline with 0.05% Tween-20 (PBST) and were incubated with goat anti-rabbit or anti-mouse IgG (1:2500; Beyotime, China) for 1 h, washed three times with PBST and detected with Super ECL Detection Reagent (Shanghai YEASEN Biotechnology Co. Ltd, China). Bands were imaged by the Tanon 5200 Chemiluminescent Imaging System (Tanon, China).
Statistical analysis
The Cox proportional hazards regression model was used to check for potential predictors of survival among all variables. The multivariate analysis of the rs9642880 G > T polymorphism was adjusted for clinical variables that were significantly associated with overall survival in the univariate Cox proportional hazards regression model. The survival analysis was performed using the Kaplan-Meier method and log-rank test. Associations between the rs9642880 G > T polymorphism and clinical characteristics were calculated using a binary logistic regression model. All statistical analyses were performed using SPSS software, version 20.0 (SPSS Inc., USA).
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
References
Mornex, F. et al. Feasibility and efficacy of high-dose three-dimensional-conformal radiotherapy in cirrhotic patients with small-size hepatocellular carcinoma non-eligible for curative therapies–mature results of the French Phase II RTF-1 trial. International journal of radiation oncology, biology, physics 66, 1152–1158, https://doi.org/10.1016/j.ijrobp.2006.06.015 (2006).
Zeng, Z. C. et al. A comparison of chemoembolization combination with and without radiotherapy for unresectable hepatocellular carcinoma. Cancer journal (Sudbury, Mass.) 10, 307–316 (2004).
Zheng, J. et al. A sequence polymorphism in miR-608 predicts recurrence after radiotherapy for nasopharyngeal carcinoma. Cancer research 73, 5151–5162, https://doi.org/10.1158/0008-5472.CAN-13-0395 (2013).
Schoenfeld, J. D. et al. A single nucleotide polymorphism in inflammatory gene RNASEL predicts outcome after radiation therapy for localized prostate cancer. Clinical cancer research: an official journal of the American Association for Cancer Research 19, 1612–1619, https://doi.org/10.1158/1078-0432.CCR-12-2718 (2013).
DePinho, R. A., Schreiber-Agus, N. & Alt, F. W. myc family oncogenes in the development of normal and neoplastic cells. Advances in cancer research 57, 1–46 (1991).
O’Donnell, K. A., Wentzel, E. A., Zeller, K. I., Dang, C. V. & Mendell, J. T. c-Myc-regulated microRNAs modulate E2F1 expression. Nature 435, 839–843, https://doi.org/10.1038/nature03677 (2005).
Wade, M. A. et al. c-MYC is a radiosensitive locus in human breast cells. Oncogene 34, 4985–4994, https://doi.org/10.1038/onc.2014.427 (2015).
Wang, M. et al. Common genetic variants on 8q24 contribute to susceptibility to bladder cancer in a Chinese population. Carcinogenesis 30, 991–996, https://doi.org/10.1093/carcin/bgp091 (2009).
Wang, W. J. et al. MYC regulation of CHK1 and CHK2 promotes radioresistance in a stem cell-like population of nasopharyngeal carcinoma cells. Cancer research 73, 1219–1231, https://doi.org/10.1158/0008-5472.CAN-12-1408 (2013).
Kim, H. et al. Whole-genome and multisector exome sequencing of primary and post-treatment glioblastoma reveals patterns of tumor evolution. Genome research 25, 316–327, https://doi.org/10.1101/gr.180612.114 (2015).
Wallace, C., Dobson, R. J., Munroe, P. B. & Caulfield, M. J. Information capture using SNPs from HapMap and whole-genome chips differs in a sample of inflammatory and cardiovascular gene-centric regions from genome-wide estimates. Genome research 17, 1596–1602, https://doi.org/10.1101/gr.5996407 (2007).
Park, W. et al. Local radiotherapy for patients with unresectable hepatocellular carcinoma. International journal of radiation oncology, biology, physics 61, 1143–1150, https://doi.org/10.1016/j.ijrobp.2004.08.028 (2005).
Seong, J. et al. A multicenter retrospective cohort study of practice patterns and clinical outcome on radiotherapy for hepatocellular carcinoma in Korea. Liver international: official journal of the International Association for the Study of the Liver 29, 147–152, https://doi.org/10.1111/j.1478-3231.2008.01873.x (2009).
Zeng, Z. C. et al. A comparison of treatment combinations with and without radiotherapy for hepatocellular carcinoma with portal vein and/or inferior vena cava tumor thrombus. International journal of radiation oncology, biology, physics 61, 432–443, https://doi.org/10.1016/j.ijrobp.2004.05.025 (2005).
Guo, Z., Shu, Y., Zhou, H., Zhang, W. & Wang, H. Radiogenomics helps to achieve personalized therapy by evaluating patient responses to radiation treatment. Carcinogenesis 36, 307–317, https://doi.org/10.1093/carcin/bgv007 (2015).
Ahmed, M. et al. ATM mutation and radiosensitivity: An opportunity in the therapy of mantle cell lymphoma. Critical reviews in oncology/hematology 107, 14–19, https://doi.org/10.1016/j.critrevonc.2016.08.008 (2016).
Lobachevsky, P. et al. Compromized DNA repair as a basis for identification of cancer radiotherapy patients with extreme radiosensitivity. Cancer letters 383, 212–219, https://doi.org/10.1016/j.canlet.2016.09.010 (2016).
Hallikas, O. et al. Genome-wide prediction of mammalian enhancers based on analysis of transcription-factor binding affinity. Cell 124, 47–59, https://doi.org/10.1016/j.cell.2005.10.042 (2006).
Jia, L. et al. Functional enhancers at the gene-poor 8q24 cancer-linked locus. PLoS genetics 5, e1000597, https://doi.org/10.1371/journal.pgen.1000597 (2009).
Kim, J. et al. A Myc network accounts for similarities between embryonic stem and cancer cell transcription programs. Cell 143, 313–324, https://doi.org/10.1016/j.cell.2010.09.010 (2010).
Castro, I. C. et al. MYC-induced epigenetic activation of GATA4 in lung adenocarcinoma. Molecular cancer research: MCR 11, 161–172, https://doi.org/10.1158/1541-7786.MCR-12-0414-T (2013).
Kaposi-Novak, P. et al. Central role of c-Myc during malignant conversion in human hepatocarcinogenesis. Cancer research 69, 2775–2782, https://doi.org/10.1158/0008-5472.CAN-08-3357 (2009).
Kress, T. R. et al. Identification of MYC-Dependent Transcriptional Programs in Oncogene-Addicted Liver Tumors. Cancer research 76, 3463–3472, https://doi.org/10.1158/0008-5472.CAN-16-0316 (2016).
Yates, D. R. et al. Genetic polymorphisms on 8q24.1 and 4p16.3 are not linked with urothelial carcinoma of the bladder in contrast to their association with aggressive upper urinary tract tumours. World journal of urology 31, 53–59, https://doi.org/10.1007/s00345-012-0954-6 (2013).
Bruix, J. & Sherman, M., Practice Guidelines Committee, A. A. f. t. S. o. L. D. Management of hepatocellular carcinoma. Hepatology 42, 1208–1236, https://doi.org/10.1002/hep.20933 (2005).
Eisenhauer, E. A. et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). European journal of cancer 45, 228–247, https://doi.org/10.1016/j.ejca.2008.10.026 (2009).
Zhao, X. M. et al. Association between IRS-2 G1057D polymorphism and risk of gastric cancer. World journal of gastrointestinal oncology 4, 9–15, https://doi.org/10.4251/wjgo.v4.i1.9 (2012).
Acknowledgements
The authors thank all the patients who agreed to participate in this study. This work was supported by the National Natural Science Foundation of China (Grant No. U1505229) and the Young Researcher Project of Zhongshan Hospital, Fudan University(Grant no. 2015ZSQN18).
Author information
Authors and Affiliations
Contributions
This study was designed by X.Z., Z.X. and Z.Z. Experiments were performed by X.Z., P.Y. and Y.C. Data were analysed by X.Z. and Y.H. The paper was written by X.Z. and Z.Z.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhao, XM., Xiang, ZL., Chen, YX. et al. A sequence polymorphism on 8q24 is associated with survival in hepatocellular carcinoma patients who received radiation therapy. Sci Rep 8, 2264 (2018). https://doi.org/10.1038/s41598-018-20700-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-20700-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
