
Abstract
Knee osteoarthritis (OA) is an established risk factor for falls and balance impairment. This study investigated the incidence of falls, balance-related outcomes and risk factors for falls before and after primary total knee arthroplasty (TKA). Three hundred seventy-six OA patients scheduled to undergo TKA were included. Falls data within the preoperative, first postoperative and second postoperative years were collected, balance-related functions were assessed using the Assessment of Quality of Life (AQoL), WOMAC, Falls Efficacy Scale International (FES-I), Activities-specific Balance Confidence (ABC), knee extension strength, Berg Balance Scale (BBS) and Timed Up and Go (TUG) before surgery and 1 and 2 years after surgery. Compared with preoperative values, the incidence of falls significantly decreased (14.89%, 6.23% and 3.14% within the preoperative, first postoperative and second postoperative years, respectively) and the AQoL, WOMAC, FES-I, ABC, knee extension strength, BBS and TUG significantly improved after TKA. Logistic regression analysis revealed that Kellgren-Lawrence grade ≥ 3 of the contralateral knee was an independent risk factor for falls before and after TKA. Conclusively, primary TKA is associated with a reduced incidence of falls and improved balance-related functions, and the contralateral knee should be considered in the design of fall-prevention strategies in patients with OA.
Similar content being viewed by others

Introduction
Falls are among the most common causes of injury and hospitalization in the elderly, and an estimated 1/3 of people over the age of 65 fall each year1. The reported annual incidence of falls among older Chinese community-dwelling people ranges from 11% to 34%, and the annual incidence of more than one fall is 4% to 5%2. Balance is a complex function that requires the integration of sensory information of the position of the body and the ability to make proper motor responses to body movement3. Balance is essential for maintaining postural stability while performing daily activities4, and loss of balance is a common cause of falls in older people5,6.
Osteoarthritis (OA) is a widely prevalent and age-associated joint disorder, and it is an important risk factor for falls. More than 50% of all OA patients and 64% of female OA patients report falling within one year5,7,8,9. Approximately 60% to 80% of patients with knee OA report joint instability10,11. No effective treatments are currently available to prevent or reverse OA progression12, but total knee arthroplasty (TKA) is a common surgical intervention for treating end-stage knee OA. TKA aims to relieve pain, restore loco-motor functions, correct deformities and improve quality of life13. Patients with knee OA undergoing TKA often present with residual functional deficits, and one important area of concern is balance impairments, which increase the risk of falls in these patients14,15,16,17. The incidence of falls is as high as 7% to 40% after TKA18,19,20.
An understanding of the issues associated with the recovery of balance-related functions following TKA may ultimately enhance the design of fall-prevention programmes supported by scientific evidence3. Previous studies assessed balance-related functions in OA patients only during early stages after TKA at 1 year or less in small samples, and the results were inconsistent and controversial3,5,21. OA often involves bilateral knees22, and previous studies demonstrated that the pain and knee extension strength of the contralateral knee were associated with knee functions after TKA22,23. However, few studies investigated the impact of the OA status of the contralateral knee on the incidence of falls after primary TKA. We hypothesize that the annual incidence of falls and balance-related functions will improve after primary TKA, and the OA status of the contralateral knee, age and sex are risk factors for falls before and after TKA in OA patients. This study investigated the following specific issues: (1) the annual incidence of falls before and after primary TKA; (2) the effect of primary TKA on balance-related outcomes, such as fear of falling, balance confidence and physical functions; and (3) the possible risk factors for falls before and after primary TKA in patients with knee OA.
Methods
Patients
Consecutive patients who were scheduled for primary unilateral TKA at the Department of Orthopaedics, West China Hospital, Sichuan University were assessed from August 2013 to December 2014 and invited to participate if they met the following eligibility criteria: (1) diagnosis of end-stage primary knee OA with no previous surgery on either knee; (2) absence of uncontrolled systemic diseases, neurological, cardiac, psychiatric disorders, or other medical conditions that would significantly compromise physical functions (e.g., stroke); and (3) sufficient language skills to communicate, the ability to follow verbal instructions, and no memory problems. Patients were excluded for any of the following reasons: (1) if they did not understand the nature of the study; (2) if they underwent TKA due to non-OA diseases, such as rheumatoid arthritis (RA) and traumatic injury; or (3) if they underwent reoperation of the replaced knee or received contralateral knee arthroplasty during the follow-up period.
Ethics approval was obtained from the Ethics Committee of West China Hospital, Sichuan University, and all procedures were performed according to the Declaration of Helsinki. All participants were informed of the nature of the study and signed a written informed consent before participation.
Total knee arthroplasty
The same surgical team performed all surgeries using a standard medial parapatellar approach in the same laminar air flow operating room, and a posterior stabilized knee prosthesis system (DePuy, New Jersey, USA) with a mobile or fixed bearing was used in all patients. A pneumatic tourniquet was used in all patients, which was inflated before skin incision and released after prosthesis placement, and a suction drainage was indwelled before suturing and removed the first morning after surgery. All patients received similar perioperative physiotherapy, such as enhanced perioperative education, muscle strengthening and gait re-education before surgery, flexion-extension of the ankle joints and straight leg raising immediately after anaesthesia awakening, and flexion-extension of the operated knee, muscle strengthening and gait re-education beginning on the first postoperative day (POD). Fall-prevention strategies, including an enhanced explanation of the hazards and risk factors of falls to enhance patient consciousness of fall-prevention, correcting high-risk activities, introducing methods to avoid falling during daily activities, and guided preoperative and postoperative functional exercises were performed during hospitalization (face to face) and after discharge (quarterly by telephone and at each follow-up visit). The surgical characteristics, including incision length, operative time (from the skin incision to the end of skin suture) and prosthesis type (mobile or fixed) were recorded.
Self-reported measures
After being recruited to the study, participants completed a series of self-reported questionnaires and physical performance tests for falls, quality of life, fear of falling, balance confidence and physical functions one day before surgery (T0), and 1 year (T1) and 2 years (T2) after surgery. A fall was defined as unintentionally coming to rest on the ground or at some other lower level, not as a result of a major intrinsic event, such as faint or stroke3. Preoperative fall data within the previous 1 year were collected at T0, and postoperative fall data were collected quarterly by telephone and confirmed at the yearly follow-up visit. Quality of life was measured using the self-reported Assessment of Quality of Life (AQoL), which is composed of five domains, including illness, independent living, social relationships, physical senses and psychological well-being, with three items per domain24. The utility scores for each dimension and an overall utility score from 0 to 1 (0 representing the worst health and 1 representing perfect health) were collected.
The Short Falls Efficacy Scale International (FES-I) questionnaire was used to evaluate the fear of falling25. The FES-I consists of seven items (score 1–4 for each) that evaluate the participant’s level of concern of the possibility of falling when performing certain daily activities, and the total score ranges from 7 (not concerned) to 28 (severely concerned). The self-reported Activities-specific Balance Confidence (ABC) Scale was used to quantify how confident a person feels that he or she will not lose balance while performing 16 certain daily activities on a scale from 0% (absolutely not confident) to 100% (completely confident)18. The total score was averaged across the 16 items, and higher scores indicate greater balance confidence.
Pain, stiffness and physical functions of the knee were also assessed using the Western Ontario and McMaster University Osteoarthritis Index (WOMAC)26, which assesses over three domains, including the severity of knee pain during 5 daily activities (range 0–500), stiffness (range 0–200), and physical functions of the lower extremities during 17 daily activities (range 0–1,700). The items were scored using a 100-mm visual analogue scale, where 0 represents no pain, stiffness or difficulty with physical functions, and higher scores represent worse functional health. All three subscales are summed to provide a total WOMAC score (range 0–2,400).
Physical performance tests
The knee extension strength, Berg Balance Scale (BBS), and Timed Up and Go (TUG) were used to further assess balance-related functions. The knee extension strength was measured via isometric pulling at 90° against padded straps attached to an electronic dynamometer (HANDPITM, Zhejiang, China). The highest value (kg) of the three trials was recorded and normalized to the patient’s body height and body mass using the following formula5: normalized knee extension strength = measured strength (kg)/[body height (m) × body mass (kg)] × 100. The BBS is a physical assessment of balance comprising a set of 14 balance tasks27. Each subset was scored on a 5-level ordinal scale from 0 to 4, yielding a maximum total score of 56. Higher scores indicate better balance, and scores below 45 indicate an increased risk of falls. A change of 4–7 points in the elderly is the estimated minimal detectable change at a 95% confidence level (MDC95) that may be objectively determined for a patient28. TUG is a test of functional mobility in older people29. The patient is observed and timed while getting up from an armchair, walking 3 metres, and returning to their original seated position. Older adults who take longer than 14 sec to complete the TUG have a high fall risk30, and the minimal level of detectable change at the 90% confidence level (MDC90) is 2.49 sec.31. Researchers with rich clinical experience in assessing elderly performed the physical assessments, and the researchers were blinded to the preoperative results upon performing the postoperative assessments.
Statistical analysis
All statistical analyses were performed using SPSS software (version 22.0, IBM, USA). All continuous variables were assessed for normality of distribution using the Kolmogorov-Smirnov and Shapiro-Wilk tests prior to data analysis. Comparisons of continuous variables between two groups were made using the t-test for normally distributed data or the Wilcoxon signed rank sum test for non-normally distributed data. Comparisons of continuous variables between three or more groups were performed using one-way analysis of variance (ANOVA) with Student-Newman-Keuls (SNK) post hoc analysis for normally distributed data or the Kruskal-Wallis H and Mann-Whitney U tests for non-normally distributed data. Comparisons of dichotomous variables were performed using the Cochran Q test for repeated measures or the Chi-square (χ 2) test for non-repeated measures. Binary logistic regression was performed to identify independent risk factors for falls, and the general and surgical factors, including age, sex, body mass index, KL grade of the contralateral knee, incision length, operative time and prosthesis type, were included in the model. A P value less than 0.05 was considered statistically significant.
Results
Subjects
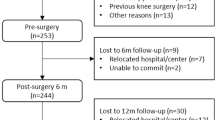
Figure 1 provides the full details of the study flow. A total of 376 OA patients (117 males) undergoing primary and unilateral TKA were included preoperatively, with a mean age of 68.88 (47–89) years. A total of 321 (85.37%) and 350 (93.09%) patients were followed-up at T1 and T2, respectively. There were no significant differences in the general and surgical characteristics, including age, gender, body mass index (BMI), KL grade of the contralateral knee, incision length, operative time and prosthesis type, between patients at T0 to T2 (all Ps < 0.05).

Flow diagram of the study. (a) Reasons for exclusion were patients undergoing bilateral TKA or undergoing TKA because of rheumatoid or traumatic arthritis. (b) Reasons for exclusion were patients who did not understand the nature of the study, refused to participate, were illiterate, or were physically or mentally unable to complete the questionnaires. (c) Patients who were included but were lost by the yearly follow-up because of various reasons, such as traffic or health problems.
Fallers and falls before and after primary TKA
Table 1 shows the details of the pre- and postoperative fallers and falls. A total of 14.89% (56/376) of patients fell, encompassing a total of 101 falls in the last preoperative year. A total of 6.23% (20/321) of patients had a total of 27 falls in the first postoperative year, and 3.14% (11/350) of patients had a total of 14 falls in the second postoperative year. A total of 58.93% (33/56) of the fallers experienced more than one fall in the last preoperative year compared to 25.00% (5/20) and 18.18% (2/11) in the first and second postoperative years, respectively. There were significant reductions in the postoperative number of total fallers (the incidence of falls) and fallers with more than one fall compared to the preoperative values (Q = 50.98, P < 0.01; Q = 46.69, P < 0.01, respectively).
A total of 76.00% (38/50, n = 321) and 90.57% (48/53, n = 350) of preoperative fallers did not fall again in the first and second postoperative years, respectively, and 2.95% (8/271, n = 321) and 2.02% (6/297, n = 350) of preoperative non-fallers fell in the first and second postoperative years, respectively. A significant shift in favour of preoperative fallers becoming postoperative non-fallers was observed (Q = 78.18, P < 0.01). A total of 13.03% (49/376) of patients required an aid to walk independently outside at T0, and this percentage was significantly reduced to 6.85% (22/321) and 3.71% (13/350) at T1 and T2, respectively (Q = 58.50, P < 0.01).
Balance-related outcomes before and after primary TKA
Table 2 shows the serial changes in balance-related outcomes. The AQoL, WOMAC (total and subscales), FES-I, ABC, knee extension strength, BBS and TUG improved significantly after primary TKA compared with preoperative values (all Ps < 0.01). The AQoL was significantly higher at T2 than at T0 and T1, but no significant difference was found between the scores at T0 and T1. The WOMAC (total and subscales) and FES-I were significantly lower at T1 and T2 than at T0, and the scores were also significantly lower at T2 than at T1. The ABC was significantly higher at T1 and T2 than at T0, and the ABC was also significantly higher at T2 than at T1. Physical performance tests revealed that the knee extension strength and BBS were significantly higher at T1 and T2 than at T0, and the knee extension strength was also significantly higher at T2 than at T1. No significant difference was observed between the BBS at T1 and T2. A total of 61.68% (198/321) and 57.71% (202/350) of patients exhibited increased BBS scores at T1 and T2, respectively, and 45.48% (146/321) and 43.71% (153/350) exceeded the MDC95 (4 points) at T1 and T2, respectively. In contrast, the TUG was significantly lower at T1 and T2 than at T0, and the TUG was also significantly lower at T2 than at T1. A total of 68.85% (221/321) and 70.86% (248/350) of these patients exhibited a decrease in TUG at T1 and T2, respectively, and 59.81% (192/321) and 62.00% (217/350) demonstrated an improvement greater than the MDC90 (2.49 sec) at T1 and T2, respectively.
Comparisons between fallers and non-fallers before and after primary TKA
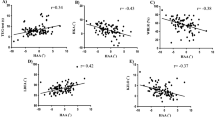
Table 3 shows that the mean age and percentage of female patients were significantly higher in fallers than in non-fallers at T0 and T1, and the KL grade of the contralateral knee was significantly higher in fallers than in non-fallers at T0 to T2 (all Ps < 0.05). There were no significant differences in BMI, incision length, operative time or prosthesis type between fallers and non-fallers (all Ps > 0.05). Figure 2 shows balance-related outcomes between fallers and non-fallers. The AQoL and the ABC at T0 to T2 and the BBS at T0 and T2 were significantly lower in fallers than in non-fallers (all Ps < 0.05). In contrast, the FES-I and the TUG were significantly higher in fallers than in non-fallers at T0 and T2 (all Ps < 0.05). There were no significant differences in WOMAC (total and subscales) or knee extension strength between fallers and non-fallers (all Ps > 0.05).

Comparisons of balance-related outcomes between fallers and non-fallers. AQoL, Assessment of Quality of Life; WOMAC, Western Ontario and McMaster University Osteoarthritis Index; FES-I, Falls Efficacy Scale International; ABC, Activities-specific Balance Confidence; BH, Body Height (m); BM, Body Mass (kg); BBS, Berg Balance Scale; TUG, Timed Up and Go. *Compared with non-fallers, P < 0.05.
Risk factors for falls before and after primary TKA
We performed binary logistic regression analysis of all factors, as shown in Table 3, to investigate the possible risk factors for falls before and after primary TKA. Table 4 shows that age (≥70 years), sex (female) and KL grade of the contralateral knee (≥3) were significant independent risk factors for a history of falling in the last preoperative year and the first postoperative year, and the latter was also a significant independent risk factor in the second postoperative year.
Discussion
Knee OA is an established risk factor for falls, and TKA is the most frequently performed surgery to treat end-stage knee OA32. Therefore, the impact of TKA on the incidence of falls and balance-related outcomes in OA patients and the possible risk factors for falls before and after TKA are of considerable interest. This study found that the annual incidence of falls, AQoL, WOMAC (total and subscales), FES-I, ABC, knee extension strength, BBS and TUG improved significantly after primary TKA compared to preoperative values. Age (≥70 years), sex (female) and KL grade of the contralateral knee (≥3) were identified as significant independent risk factors for falls in the last preoperative year and the first postoperative year, and the latter was also an independent risk factor for falls in the second postoperative year after primary TKA.
The reported annual incidence of falls ranges from 11–34% in older Chinese community-dwelling people2, and the incidence is greater than 50% in people with knee OA and ranges from 7–40% in patients after TKA5,7,8,18,19. We reported a relatively lower incidence before (14.89%) and after primary TKA (6.23% and 3.14% in the first and second postoperative year, respectively) compared to the previous studies, which may be related to multiple factors, including fall-prevention strategies, data collection, and patient sources. Campbell et al. reported that single interventions were as effective in reducing falls as interventions with multiple components33, but Gillespie et al. reported that interventions aimed to improve knowledge on fall-prevention alone did not significantly reduce the risk of falls in older community-dwelling adults7. However, few studies compared the effects of interventions to improve fall-related knowledge on the incidence of falls between community-dwelling people and post-TKA patients. The fall-prevention strategies performed in this study included interventions to improve fall-related knowledge and functions. It is difficult to investigate whether increased fall-prevention knowledge alone affected the risk of falls after TKA. Fall-prevention strategies generally commence during the preoperative period and appear to be most effective when they target high-risk populations or individuals33. However, the optimal timing and interventions to prevent falls before and after TKA are rarely reported, and therefore, these factors are important areas for further study. Previous studies have also reported that fall recollection is commonly characterised by poor sensitivity compared to prospective fall tracking34,35, and the active tracking of falls after surgery may lead to reduced falls simply from participant awareness that their falls were being recorded (Hawthorne effect)36. A small number of patients in this study could not accurately recollect the details of the falls, especially before surgery, although most patients were very sure of the number and details of their falls (Table 2). It also possible that some patients were unable to recollect their falls despite not presenting any obvious memory dysfunction, and thus, the results may have underestimated the incidence of falls. The source of patients—approximately 70% of patients were from cities—may also have contributed to the low incidence of falls in the study; however, the effect of living environment on the incidence of falls must be further investigated.
Falls are the most frequent type of accident and the major cause of injury-related hospitalization in the elderly. Falls may cause older people to become fearful of falling even when falls do not result in physical injury, which reduces quality of life, restricts daily activities and results in the onset of functional decline37. Fear of falling is a common problem in people with lower limb arthritis and has serious consequences in relation to reduced activity and loss of confidence and independence25. Significant reduction in fear of falling and an increase in balance confidence were found after TKA compared to before TKA in this study, and this finding may be due, at least in part, to the considerable improvements in knee pain, stiffness and physical functions (WOMAC), which were consistent with previous studies3,5,38. Levinger et al. found that the AQoL was significantly reduced 4 months postoperatively compared to preoperative scores, which may be primarily associated with impairments in independent living and social relationships5. We found that the AQoL was slightly increased 1 year after surgery and remarkably improved 2 years after surgery, which indicates that the quality of life improved at least 1 year after primary TKA. However, self-reported measures alone may fail to capture actual changes in physical ability following TKA and overestimate performance changes39,40,41. Physical performance tests are necessary to further evaluate balance-related functions.
Deficits in muscular function are consistently reported in patients with knee OA and in patients who undergo knee arthroplasty6,42,43,44,45. Knee pain and quadriceps weakness affect the sensory and mechanical functions of the joint, and these factors are associated with increased postural sway44,45,46,47, which results in balance difficulties and increased risk of falls48,49. Several methods for assessing knee extension strength have been reported, such as direct measurement (Newton, pound and kilogram) and normalization to body mass and/or body height5,50,51. However, previous findings of altered knee extension strength following TKA are inconsistent and controversial, and there is no consensus on which method performs best5,21,46,52,53. In this study, the knee extension strength was normalized to the patient’s body height and body mass according to a previous study5 and was notably improved following primary TKA. There were no significant differences in normalized knee extension strength between fallers and non-fallers, but the fallers exhibited relatively weaker strength than non-fallers. BBS and TUG are commonly used physical performance tests for lower limb functions29,54, and these measurements are related to the risk of accidental falling in community dwelling adults55,56. Swinkels et al. reported increased BBS and reduced TUG (both improvements) 6 months after TKA compared to preoperative values, and the differences between pre- and postoperative TUG reached statistical significance54. We performed this study using a longer follow-up and found that BBS and TUG improved significantly 1 and 2 years after surgery compared to preoperative scores, which suggests that TKA improved the risk of accidental falling in patients with knee OA.
Various questionnaires and physical tests have been developed to assess balance-related functions3,18. However, these tests are not without limitations, and there is no consensus on which tool performs best. Therefore, a combination of different tools has been suggested3,18. Swinkels et al. reported that BBS was significantly negatively correlated with TUG and positively correlated with ABC, stiffness and physical functions of WOMAC before and after surgery. TUG was also significantly negatively correlated with ABC54. In contrast, Minzner et al. reported poor concurrent validity between patient-reported and performance-based measures of physical functions in patients who undergo unilateral TKA57. The present study also found that AQoL was positively correlated with BBS before surgery (r = 0.15, P < 0.01) and negatively correlated with TUG 1 year and 2 years after surgery (r = −0.13, P = 0.02; r = −0.13, P = 0.01, respectively) and that ABC was negatively correlated with TUG 1 year after surgery (r = −0.14, P = 0.01). Differences in the time assessments and the methods used may have affected these results, and further studies are needed to investigate the correlations between self-reported and physical performance outcomes for the risk for falls and balance-related functions.
Age and gender are important risk factors for falls, and older patients and women exhibit a higher likelihood of falling37,58. Our study found that age (≥70 years) and gender (female) were significant independent risk factors for falls in patients with end-stage OA and during the first postoperative year following primary TKA. A large proportion of patients who undergo TKA for the treatment of end-stage OA have concurrent OA in the contralateral knee22. Many studies demonstrated that pre- and postoperative factors in the contralateral knee, such as pain and knee extension strength22,23, were associated with knee functions after TKA, but few studies investigated the impact of contralateral knee OA status on falling. We found that the OA severity of the contralateral knee was an independent risk factor for falls before and after TKA, and KL grade ≥3 of the contralateral knee was associated with an increased likelihood of falling. Therefore, surgeons and physiotherapists should pay more attention to contralateral knee status, in addition to age and gender, in patients with knee OA before and after primary TKA when designing fall-prevention strategies.
Several limitations must be considered when interpreting the findings of this study. First, the participants in this study had primary and unilateral TKA due to OA. These results may only be generalized to individuals with similar characteristics, and further studies are warranted to expand the present results and the generalizability to patients with bilateral or unicompartmental knee arthroplasty or other conditions (such as RA). Second, fall data were collected using interviews or telephone calls, which primarily rely on the retrospective recall of falls by patients and may result in an underestimation of fall prevalence. Third, no non-surgical group with similar severity of knee OA was recruited as control, and all patients in this study received a similar postoperative rehabilitation programme. Thus, this study was unable to establish the natural course of falls and whether the postoperative rehabilitation accounted for the reduced incidence of falls. Fourth, although the strength testing data was normalized to body height and body mass, the lever arm at the point of force application was not taken into account, and therefore, the data were not fully normalized to subject anthropometrics. Finally, other factors, such as psychophysiological status, comorbidities and lifestyles were not documented and may have affected the results. However, to our knowledge, our findings reported the serial changes in the incidence of falls and balance-related outcomes and identified possible risk factors for falls before and after primary TKA in the largest population and for the longest period of follow-up of any existing study.
In conclusion, the data of this study suggest that primary TKA is associated with a reduced incidence of falls and improved balance-related functions in patients with OA. OA severity of the contralateral knee is a significant independent risk factor for falls, and surgeons and physiotherapists should pay more attention to the contralateral knee when designing fall-prevention strategies before and after primary TKA in patients with OA.
References
Close, J. et al. Prevention of falls in the elderly trial (PROFET): a randomised controlled trial. Lancet 353(9147), 93–97 (1999).
Kwan, M. M., Close, J. C., Wong, A. K. & Lord, S. R. Falls incidence, risk factors, and consequences in Chinese older people: a systematic review. J Am Geriatr Soc 59(3), 536–643 (2011).
Moutzouri M. et al. The effect of total knee arthroplasty on patients’ balance and incidence of falls: a systematic review. Knee Surg Sports Traumatol Arthrosc (2016).
Sibley, K. M., Beauchamp, M. K., Van Ooteghem, K., Straus, S. E. & Jaglal, S. B. Using the systems framework for postural control to analyze the components of balance evaluated in standardized balance measures: a scoping review. Arch Phys Med Rehabil 96(1), 122–132.e129 (2015).
Levinger, P. et al. Physiological risk factors for falls in people with knee osteoarthritis before and early after knee replacement surgery. Knee Surg Sports Traumatol Arthrosc 19(7), 1082–1089 (2011).
Wang, X. et al. Mobility and muscle strength together are more strongly correlated with falls in suburb-dwelling older chinese. Sci Rep 6, 25420 (2016).
Gillespie, L. D. et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev 9, Cd007146 (2012).
Williams, S. B., Brand, C. A., Hill, K. D., Hunt, S. B. & Moran, H. Feasibility and outcomes of a home-based exercise program on improving balance and gait stability in women with lower-limb osteoarthritis or rheumatoid arthritis: a pilot study. Arch Phys Med Rehabil 91(1), 106–114 (2010).
Xing, D. et al. Osteoarthritis and all-cause mortality in worldwide populations: grading the evidence from a meta-analysis. Sci Rep 6, 24393 (2016).
Fitzgerald, G. K., Piva, S. R. & Irrgang, J. J. Reports of joint instability in knee osteoarthritis: its prevalence and relationship to physical function. Arthritis Rheum 51(6), 941–946 (2004).
Schmitt, L. C., Fitzgerald, G. K., Reisman, A. S. & Rudolph, K. S. Instability, laxity, and physical function in patients with medial knee osteoarthritis. Phys Ther 88(12), 1506–1516 (2008).
Glyn-Jones, S. et al. Osteoarthritis. Lancet 386(9991), 376–387 (2015).
Vielgut, I. et al. Sports activity after low-contact-stress total knee arthroplasty - a long term follow-up study. Sci Rep 6, 24630 (2016).
Nguyen, U. S. et al. The impact of knee instability with and without buckling on balance confidence, fear of falling and physical function: the Multicenter Osteoarthritis Study. Osteoarthritis Cartilage 22(4), 527–534 (2014).
Sorensen, R. R., Jorgensen, M. G., Rasmussen, S. & Skou, S. T. Impaired postural balance in the morning in patients with knee osteoarthritis. Gait Posture 39(4), 1040–1044 (2014).
Duffell, L. D., Southgate, D. F., Gulati, V. & McGregor, A. H. Balance and gait adaptations in patients with early knee osteoarthritis. Gait Posture 39(4), 1057–1061 (2014).
Khalaj, N., Abu Osman, N. A., Mokhtar, A. H., Mehdikhani, M. & Wan Abas, W. A. Balance and risk of fall in individuals with bilateral mild and moderate knee osteoarthritis. PLoS One 9(3), e92270 (2014).
Chan, A. C. & Pang, M. Y. Assessing Balance Function in Patients With Total Knee Arthroplasty. Phys Ther 95(10), 1397–1407 (2015).
Swinkels, A., Newman, J. H. & Allain, T. J. A prospective observational study of falling before and after knee replacement surgery. Age Ageing 38(2), 175–181 (2009).
D, L. R. & G, J. G. A longitudinal comparative study of falls in persons with knee arthroplasty and persons with or at high risk for knee osteoarthritis. Age Ageing 45(6), 794–800 (2016).
Petterson, S. C. et al. Improved function from progressive strengthening interventions after total knee arthroplasty: a randomized clinical trial with an imbedded prospective cohort. Arthritis Rheum 61(2), 174–183 (2009).
Maxwell, J. et al. The influence of the contralateral knee prior to knee arthroplasty on post-arthroplasty function: the multicenter osteoarthritis study. J Bone Joint Surg Am 95(11), 989–993 (2013).
Zeni, J. A. Jr. & Snyder-Mackler, L. Early postoperative measures predict 1- and 2-year outcomes after unilateral total knee arthroplasty: importance of contralateral limb strength. Phys Ther 90(1), 43–54 (2010).
Tilbury, C. et al. Outcome of total hip arthroplasty, but not of total knee arthroplasty, is related to the preoperative radiographic severity of osteoarthritis. A prospective cohort study of 573 patients. Acta Orthop 87(1), 67–71 (2016).
Kempen, G. I. et al. The Short FES-I: a shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 37(1), 45–50 (2008).
Faschingbauer M. et al. Predictive values of WOMAC, KOOS, and SF-12 score for knee arthroplasty: data from the OAI. Knee Surg Sports Traumatol Arthrosc (2016).
Berg, K. O., Maki, B. E., Williams, J. I., Holliday, P. J. & Wood-Dauphinee, S. L. Clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehabil 73(11), 1073–1080 (1992).
Donoghue, D. & Stokes, E. K. How much change is true change? The minimum detectable change of the Berg Balance Scale in elderly people. J Rehabil Med 41(5), 343–346 (2009).
Podsiadlo, D. & Richardson, S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39(2), 142–148 (1991).
Shumway-Cook, A., Brauer, S. & Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther 80(9), 896–903 (2000).
Kennedy, D. M., Stratford, P. W., Wessel, J., Gollish, J. D. & Penney, D. Assessing stability and change of four performance measures: a longitudinal study evaluating outcome following total hip and knee arthroplasty. BMC Musculoskelet Disord 6, 3 (2005).
Arden, N. K. et al. Knee pain, knee osteoarthritis, and the risk of fracture. Arthritis Rheum 55(4), 610–615 (2006).
Campbell, A. J. & Robertson, M. C. Rethinking individual and community fall prevention strategies: a meta-regression comparing single and multifactorial interventions. Age Ageing 36(6), 656–662 (2007).
Mackenzie, L., Byles, J. & D’Este, C. Validation of self-reported fall events in intervention studies. Clin Rehabil 20(4), 331–339 (2006).
Ganz, D. A., Higashi, T. & Rubenstein, L. Z. Monitoring falls in cohort studies of community-dwelling older people: effect of the recall interval. J Am Geriatr Soc 53(12), 2190–2194 (2005).
Sedgwick, P. & Greenwood, N. Understanding the Hawthorne effect. Bmj 351, h4672 (2015).
Gale, C. R., Cooper, C. & Aihie Sayer, A. Prevalence and risk factors for falls in older men and women: the English longitudinal study of ageing. Age Ageing 45(6), 789–794 (2016).
Swanik, C. B., Lephart, S. M. & Rubash, H. E. Proprioception, kinesthesia, and balance after total knee arthroplasty with cruciate-retaining and posterior stabilized prostheses. J Bone Joint Surg Am 86-a(2), 328–334 (2004).
Stratford, P. W., Kennedy, D. M., Maly, M. R. & Macintyre, N. J. Quantifying self-report measures’ overestimation of mobility scores postarthroplasty. Phys Ther 90(9), 1288–1296 (2010).
Stratford, P. W. & Kennedy, D. M. Performance measures were necessary to obtain a complete picture of osteoarthritic patients. J Clin Epidemiol 59(2), 160–167 (2006).
Stratford, P. W., Kennedy, D. M. & Woodhouse, L. J. Performance measures provide assessments of pain and function in people with advanced osteoarthritis of the hip or knee. Phys Ther 86(11), 1489–1496 (2006).
Shakoor, N. et al. Asymmetries and relationships between dynamic loading, muscle strength, and proprioceptive acuity at the knees in symptomatic unilateral hip osteoarthritis. Arthritis Res Ther 16(6), 455 (2014).
Levinger, P. et al. Lower limb proprioception deficits persist following knee replacement surgery despite improvements in knee extension strength. Knee Surg Sports Traumatol Arthrosc 20(6), 1097–1103 (2012).
Cammarata, M. L., Schnitzer, T. J. & Dhaher, Y. Y. Does knee osteoarthritis differentially modulate proprioceptive acuity in the frontal and sagittal planes of the knee? Arthritis Rheum 63(9), 2681–2689 (2011).
Hassan, B. S., Doherty, S. A., Mockett, S. & Doherty, M. Effect of pain reduction on postural sway, proprioception, and quadriceps strength in subjects with knee osteoarthritis. Ann Rheum Dis 61(5), 422–428 (2002).
Valtonen, A., Poyhonen, T., Heinonen, A. & Sipila, S. Muscle deficits persist after unilateral knee replacement and have implications for rehabilitation. Phys Ther 89(10), 1072–1079 (2009).
Gauchard, G. C., Vancon, G., Meyer, P., Mainard, D. & Perrin, P. P. On the role of knee joint in balance control and postural strategies: effects of total knee replacement in elderly subjects with knee osteoarthritis. Gait Posture 32(2), 155–160 (2010).
Hunt, M. A. et al. Lateral trunk lean explains variation in dynamic knee joint load in patients with medial compartment knee osteoarthritis. Osteoarthritis Cartilage 16(5), 591–599 (2008).
Grabiner, M. D. et al. Trunk kinematics and fall risk of older adults: translating biomechanical results to the clinic. J Electromyogr Kinesiol 18(2), 197–204 (2008).
Huang, H., Guo, J., Yang, J., Jiang, Y., Yu, Y. Isokinetic angle-specific moments and ratios characterizing hamstring and quadriceps strength in anterior cruciate ligament deficient knees. 7(1), 7269 (2017).
de Zwart, A. H. et al. Falls Associated with Muscle Strength in Patients with Knee Osteoarthritis and Self-reported Knee Instability. J Rheumatol 42(7), 1218–1223 (2015).
Fuchs, S., Thorwesten, L. & Niewerth, S. Proprioceptive function in knees with and without total knee arthroplasty. Am J Phys Med Rehabil 78(1), 39–45 (1999).
Gage, W. H., Frank, J. S., Prentice, S. D. & Stevenson, P. Postural responses following a rotational support surface perturbation, following knee joint replacement: frontal plane rotations. Gait Posture 27(2), 286–293 (2008).
Swinkels, A. & Allain, T. J. Physical performance tests, self-reported outcomes, and accidental falls before and after total knee arthroplasty: an exploratory study. Physiother Theory Pract 29(6), 432–442 (2013).
Viccaro, L. J., Perera, S. & Studenski, S. A. Is timed up and go better than gait speed in predicting health, function, and falls in older adults? J Am Geriatr Soc 59(5), 887–892 (2011).
Muir, S. W., Berg, K., Chesworth, B. & Speechley, M. Use of the Berg Balance Scale for predicting multiple falls in community-dwelling elderly people: a prospective study. Phys Ther 88(4), 449–459 (2008).
Mizner, R. L. et al. Measuring functional improvement after total knee arthroplasty requires both performance-based and patient-report assessments: a longitudinal analysis of outcomes. J Arthroplasty 26(5), 728–737 (2011).
Wei, F. & Hester, A. L. Gender difference in falls among adults treated in emergency departments and outpatient clinics. J Gerontol Geriatr Res 3, 152 (2014).
Acknowledgements
The authors would like to thank all of the patients who participated in this study, and the support of the China Postdoctoral Science Foundation (No. 2017M610604), the Postdoctoral Research and Development Project of Sichuan University (No. 2017SCU12041) and the Sichuan Provincial Health and Family Planning Commission Research Program (No. 17PJ124).
Author information
Authors and Affiliations
Contributions
Si H.b. and Ning N. conceived and designed this study. Si H.b., Ning N. and Shen B. recruited and monitored patients. Si H.b., Zeng Y., Zhong J. and Zhou Z.k. gathered the data. Si H.b., Lu Y.r., Cheng J.q., Ning N. and Shen B. analysed and interpreted the data. Si H.b. and Ning N. drafted the manuscript. All authors approved the manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Si, Hb., Zeng, Y., Zhong, J. et al. The effect of primary total knee arthroplasty on the incidence of falls and balance-related functions in patients with osteoarthritis. Sci Rep 7, 16583 (2017). https://doi.org/10.1038/s41598-017-16867-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-16867-4
This article is cited by
-
Significantly earlier ambulation and reduced risk of near-falls with continuous infusion nerve blocks: a retrospective pilot study of adductor canal block compared to femoral nerve block in total knee arthroplasty
BMC Musculoskeletal Disorders (2022)
-
Fall classification, incidence and circumstances in patients undergoing total knee replacement
Scientific Reports (2022)
-
Evaluation of the balance function before and after total knee arthroplasty using Berg balance scale
Archives of Orthopaedic and Trauma Surgery (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
