
Abstract
The present study evaluated the performance of three novel obese indicators, visceral adiposity index (VAI), lipid accumulation product (LAP) and waist circumference-triglyceride index (WTI), for identifying metabolic syndrome(MetS) in type 2 diabetes. A cross-sectional study was conducted on 711 type 2 diabetes in Qinhuangdao. The MetS was defined as the definition of Chinese Diabetes Society. Receiver operating characteristic curve analyses were performed to assess the accuracy of three obese indicators as diagnostic tests for MetS. The prevalence of MetS was 71.3%. In men, among all three obese indicators, the LAP had the highest area under curve (AUC) value (AUC = 0.894), followed by VAI (AUC = 0.860) and WTI (AUC = 0.855). In women, among all three obese indicators, the LAP had the highest AUC value (AUC = 0.906), followed by WTI (AUC = 0.887) and VAI (AUC = 0.881). However. there was no significant difference between the three obese indicators(P > 0.05). Three obese indicators were effective indicators for the screening of MetS, LAP and WTI are more simple.
Similar content being viewed by others


Introduction
Diabetes mellitus is one of the most important public health challenges of the twenty-first century1. China is one of the fastest developing countries in the world. Rapid economic progress has resulted in changes to both diet and physical activity. In China, the prevalences of diabetes and prediabetes reached 9.7% and 15.5%, respectively2. A close link exists between diabetes, cardiovascular disease and stroke, which are the most prevalent causes of morbidity and mortality in diabetic patients3, 4.
Metabolic syndrome (MetS) is a cluster of metabolic abnormalities, characterized as central obesity, elevated blood pressure, dysglycemia, elevated triglyceride (TG) levels, and low high-density lipoprotein cholesterol (HDL-C) levels. The prevalence of MetS is high in type 2 diabetes5, 6. MetS increases the risk of atherosclerotic vascular disease in type 2 diabetes7. In two prospective studies, MetS at baseline is associated with an increased risk of incident cardiovascular disease8, 9. MetS also increases the risk of stroke and is associated with stroke recurrence in type 2 diabetes10, 11.
Early identification and treatment of individuals with MetS could reduce risk of developing relevant diseases. Visceral adiposity index (VAI) and lipid accumulation product (LAP) are two novel indexes used for identifying MetS. Recently, several studies supported the use of these indexes for the screening of MetS in healthy population12,13,14,15, elderly16, 17, polycystic ovary syndrome18,19,20, and adult growth hormone deficiency21. Waist circumference-triglyceride index (WTI) is a predictor for the development of coronary artery disease22. To our knowledge no investigators have attempted to use these obese indicators for screening MetS in type 2 diabetes. The aim of our study was to evaluate the performance of three obese indicators, VAI, LAP and WTI, for identifying MetS in type 2 diabetes.
Methods
Subjects
After obtaining informed consent from subjects with type 2 diabetes a cross-sectional study was conducted. All subjects were recruited from the First Hospital of Qinhuangdao. All subjects were men and women over 18 years of age, with a diagnosis of type 2 diabetes (based on American Diabetes Association diagnostic criteria)23. The exclusion criteria included the following: (1) subjects with type 1 diabetes, (2) subjects with clinical evidence of other endocrinopathy, such as Cushing’s syndrome, hyperthyroidism, et al. (3) subjects were taking medications known to affect lipid metabolism, such as glucocorticoids, fibrates and statins, (4) subjects with acute and chronic inflammation. This study was approved by the ethics committee of the First Hospital of Qinhuangdao. All subjects provided written informed consent before study initiation. All experiments were performed in accordance with relevant guidelines and regulations.
Measurements
Anthropometric measurements, including height, weight and waist circumference(WC) were obtained while the subjects were in light clothing and barefoot. Height and weight were measured to the nearest 0.1 cm and 0.1 kg, respectively. WC was accurately measured at the level of midway between the lowest rib and the top of the iliac crest. All measurements were taken twice, and the two measurements were averaged for analysis. Blood pressure was measured three times with a mercury sphygmomanometer while the subjects were seated after 10 min of rest, and the three measurements were averaged for analysis. Body mass index(BMI) was calculated by dividing weight (kg) by height squared (m2). Waist-to-height ratio(WHtR) was calculated by dividing the WC by height.
After a 10-hour overnight fast, blood samples were collected from an antecubital vein into heparinised tubes. Fasting plasma glucose(FPG) concentration was measured using the glucose oxidase method, and serum lipid levels were measured using enzymatic assays with an autoanalyzer (Hitachi, Tokyo, Japan).
VAI, a sex-specific index based on WC, BMI, TG and HDL-C, was calculated as follows24: Males: VAI = (WC/(39.68 + (1.88 × BMI))) × (TG/1.03) × (1.31/HDL), Females: VAI = (WC/(36.58 + (1.89 × BMI))) × (TG/0.81) × (1.52/HDL). LAP was calculated as (WC (cm) − 65) × TG (mmol/L) for men, and (WC (cm) − 58) × TG (mmol/L) for women25. We used the following formula to calculate the WTI = WC(cm) × TG(mmol/L)22.
Definition of metabolic syndrome
Metabolic syndrome was defined using the definition of Chinese Diabetes Society. Participants had to meet any 3 or more of the following 5 factors: (1) WC ≥90 cm(male) and 85 cm(female), (2) FPG ≥6.1 mmol/L or 2-h plasma glucose levels ≥7.8 mmol/L after a 75-g oral glucose tolerance test (OGTT) or have been diagnosed with diabetes, (3) blood pressure ≥130/85 mmHg or have been diagnosed with hypertension, (4) TG ≥1.7 mmol/L, 5) HDL-C < 1.04 mmol/L26.
Statistical Analyses
All analyses were performed using the SPSS 11.5 statistical software (SPSS 11.5 for Windows; SPSS, Inc., Chicago, IL). Numerical variables were reported as mean ± standard deviation. Comparisons were conducted between groups using the t test. Comparison of prevalence data was performed by χ 2 analysis. For each obese indicators, we divided them into increasing sex-specific quartile values and used logistic regression analysis to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for MetS across quartiles, with quartile 1 as reference group, adjusting for potentially confounding variables such as age, BMI, drink, smoke and history of diabetes. By using receiver operating characteristic (ROC) analysis, ROC curves of each obese indicators were drawn to show how well they could separate subjects into groups with or without MetS. A test with an area under curve (AUC) of ≥0.85 is considered an accurate test27. Sensitivity and specificity of each obese indicators have been calculated at all possible cutoff points to find the optimal cutoff values. The optimal sensitivity and specificity were the values yielding maximum sums from the ROC curves. The comparisons of AUCs were performed with MedCalc 11.4.2.0 software (Ostend, Belgium). P < 0.05 was considered statistically significant.
Results
Among these subjects, 71.3% were characterized by MetS. The prevalence of MetS was similar between men and women (men 72.1% vs women 70.3%, χ 2 = 0.261, P = 0.610). Characteristics of the study population are presented in Table 1. The age, history of diabetes, drink, smoke and FPG between the two groups were similar (P > 0.05). The levels of BMI, WC, WHtR, SBP(systolic blood pressure), DBP(diastolic blood pressure), TG, VAI, LAP and WTI were all significantly higher in MetS group than in non-MetS group (P < 0.001). The level of HDL-C was significantly lower in MetS group than in non-MetS group (P < 0.001).
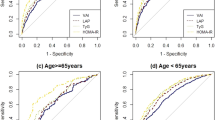
In men, among all three obese indicators, the LAP had the highest AUC value (AUC = 0.894), followed by VAI (AUC = 0.860) and WTI (AUC = 0.855). However. there was no significant difference between the three obese indicators(P > 0.05). LAP had the Youden’s index of 0.65 (Sen = 83.0%, Spe = 82.1%), with the optimal cut-off as 35.7. VAI had the Youden’s index of 0.60 (Sen = 71.9%, Spe = 88.3%), with the optimal cut-off as 2.00. WTI had the Youden’s index of 0.63 (Sen = 72.6%, Spe = 91.0%), with the optimal cut-off as 148.1. The AUC of LAP was higher than the AUCs of WC and WHtR (P < 0.05). The AUCs were similar between VAI, LAP and WTI in men (P > 0.05) (Table 2).
In women, among all three obese indicators, the LAP had the highest AUC value (AUC = 0.906), followed by WTI (AUC = 0.887) and VAI (AUC = 0.881). However. there was no significant difference between the three obese indicators(P > 0.05). LAP had the Youden’s index of 0.65 (Sen = 84.4%, Spe = 80.4%), with the optimal cut-off as 44.0. WTI had the Youden’s index of 0.64 (Sen = 70.6%, Spe = 93.4%), with the optimal cut-off as 151.7. VAI had the Youden’s index of 0.62 (Sen = 78.4%, Spe = 83.6%), with the optimal cut-off as 2.28. The AUCs of VAI, LAP and WTI were higher than the AUCs of WC and WHtR (P < 0.01). The AUCs were similar between VAI, LAP and WTI in women (P > 0.05) (Table 2).
The VAI, LAP and WTI were strongly associated with the odds of having MetS in both men and women, after adjustment for age, BMI, drink, smoke and history of diabetes. ORs for MetS increased with increasing quartiles of all variables(P < 0.001) (Tables 3, 4 and 5).
Discussion
In this population, we found that 71.3% of participants had MetS. The prevalence of MetS was very common in type 2 diabetes, which is similar to previous study5, 6. The performances of WC and WHtR were similar in our study. Several visceral adiposity indicators, such as LAP in men and LAP, WTI, VAI in women appeared to be better indices to predict presence of MetS, relative to WC and WHtR. Our study presents evidence that the LAP may simple and useful tool for the screening of MetS in type 2 diabetes.
It is now widely acknowledged that, the core of MetS is central obesity (also known as visceral adiposity), overweight with adipose tissue accumulation particularly around the waist. The evaluate of visceral adipose tissue, such as magnetic resonance imaging and computed tomography, is very expensive, may involve exposure to radiation, and their availability is limited. WC is the most accurate surrogate marker of visceral adiposity in adults, and are good indicators of insulin resistance28, 29. However, two pepole are the same in WC but different in height, so the cardiovascular risk factors maybe different. WHtR is defined as their WC divided by their height and has been widely recommended30. But the performances of WC and WHtR were similar in our study. Robust statistical evidence from studies involving 12 studies(men) and 13 studies(women) in several ethnic groups, shows the improvement in AUC (WHtR > WC) for detecting MetS is slightly in men (0.003) and women(0.009)31.
WC may be not appropriate for identifying MetS on its own. First, metabolically obese, normal-weight (MONW) individuals are very common in type 2 diabetes32. Second, obesity is a heterogeneous condition, thus metabolic abnormalities and cardiometabolic risk vary among obese individuals, with a significant proportion considered to be “metabolically healthy”33. Kahn et al. developed the LAP as an accurate index for identifying United States adults at cardiovascular risk25. LAP is an index based on a combination of WC and TG. In our study, LAP is preferred to WC and WHtR, both men and women. Dual metabolic defects are required to produce hypertriglyceridemia in obese subjects with similar levels of visceral adiposity. Mirmiran et al. found that LAP is associated with insulin resistance, lipid peroxidation, and systemic inflammation in type 2 diabetic patients34. Sambataro et al. found that LAP in relationships with insulin sensitivity (evaluated by the quantitative insulin sensitivity check index) in overweight type 2 diabetic subjects35. These results emphasize the clinical importance of assessing LAP in type 2 diabetes to identify subjects at high cardiovascular risk. WTI is similar to LAP22. Compared with LAP, WTI has better specificities but poor sensitivities.
VAI is an index estimated with the use of both anthropometric (BMI and WC) and metabolic (TG and HDL-C) parameters. This index is more complicated, but is not superior to LAP and WTI. It is consistent with previous results. In elderly, the VAI showed the lowest discriminatory power for MetS16. In the Chinese rural adults, the AUC of VAI for the screening of MetS was less than that of LAP in both men and women36.
There were differences between the results of VAI and WTI in men and women. The AUCs of WC and WHtR in women were slightly lower than men. The AUCs of LAP and WTI in women were slightly higher than men. Therefore, LAP and WTI appeared to be better indices to predict presence of MetS only in women, relative to WC and WHtR. The results suggest that WC may be more practical in men. Kim et al. found that the diagnostic values of the visceral fat area and WC for predicting the presence of multiple metabolic risk factors are influenced by gender. Although the WC and visceral fat area are similar in men, the WC is inferior to the visceral fat area in women37. WC correlates with hepatic fat accumulation in male Japanese patients with non-alcoholic fatty liver disease, but not in females38.
There are limitations to our study. First, the LAP was derived from studies of white, non-Hispanic blacks and Mexican Americans and the VAI was established in Caucasian populations24, 25. The suitability for other populations need to be further investigated. Second, the relationship between LAP, VAI, WTI and diabetic complication should be studied in the futrure. Third, the study population was relatively small. A larger sample size may be helpful in further strengthen the conclusion. Fourth, the levels of insulin were not measured in our study. We can not compare the performances of LAP, VAI and insulin resistance. Fifth, I did not record the information of excluded patients. This maybe cause some selective bias.
In summary, the prevalence of MetS was high in type 2 diabetes. Three novel obese indicators were effective indicators for the screening of MetS, LAP and WTI are more simple.
References
Zimmet, P., Alberti, K. G., Magliano, D. J. & Bennett, P. H. Diabetes mellitus statistics on prevalence and mortality: facts and fallacies. Nature reviews. Endocrinology 12, 616–622, doi:10.1038/nrendo.2016.105 (2016).
Yang, W. et al. Prevalence of diabetes among men and women in China. The New England journal of medicine 362, 1090–1101, doi:10.1056/NEJMoa0908292 (2010).
Leon, B. M. & Maddox, T. M. Diabetes and cardiovascular disease: Epidemiology, biological mechanisms, treatment recommendations and future research. World journal of diabetes 6, 1246–1258, doi:10.4239/wjd.v6.i13.1246 (2015).
Peters, S. A., Huxley, R. R. & Woodward, M. Diabetes as a risk factor for stroke in women compared with men: a systematic review and meta-analysis of 64 cohorts, including 775,385 individuals and 12,539 strokes. Lancet 383, 1973–1980, doi:10.1016/S0140-6736(14)60040-4 (2014).
Foroozanfar, Z. M., Najafipour, H. P., Khanjani, N. P. M., Bahrampour, A. P. M. & Ebrahimi, H. M. The Prevalence of Metabolic Syndrome According to Different Criteria and its Associated Factors in Type 2 Diabetic Patients in Kerman, Iran. Iranian journal of medical sciences 40, 522–525 (2015).
Udenze, I. C. et al. The prevalence of metabolic syndrome in persons with type 2 diabetes at the Lagos University Tteaching Hospital, Lagos, Nigeria. West African journal of medicine 32, 126–132 (2013).
Hanefeld, M., Koehler, C., Gallo, S., Benke, I. & Ott, P. Impact of the individual components of the metabolic syndrome and their different combinations on the prevalence of atherosclerotic vascular disease in type 2 diabetes: the Diabetes in Germany (DIG) study. Cardiovasc Diabetol 6, 13, doi:10.1186/1475-2840-6-13 (2007).
Guzder, R. N., Gatling, W., Mullee, M. A. & Byrne, C. D. Impact of metabolic syndrome criteria on cardiovascular disease risk in people with newly diagnosed type 2 diabetes. Diabetologia 49, 49–55, doi:10.1007/s00125-005-0063-9 (2006).
Bonora, E. et al. The Metabolic Syndrome is an independent predictor of cardiovascular disease in Type 2 diabetic subjects. Prospective data from the Verona Diabetes Complications Study. Diabetic medicine: a journal of the British Diabetic Association 21, 52–58 (2004).
Zhu, S. et al. Recurrent vascular events in lacunar stroke patients with metabolic syndrome and/or diabetes. Neurology 85, 935–941, doi:10.1212/WNL.0000000000001933 (2015).
Yao, M. F. et al. Gender Differences in Risks of Coronary Heart Disease and Stroke in Patients with Type 2 Diabetes Mellitus and Their Association with Metabolic Syndrome in China. International journal of endocrinology 2016, 8483405, doi:10.1155/2016/8483405 (2016).
Taverna, M. J., Martinez-Larrad, M. T., Frechtel, G. D. & Serrano-Rios, M. Lipid accumulation product: a powerful marker of metabolic syndrome in healthy population. European journal of endocrinology / European Federation of Endocrine Societies 164, 559–567, doi:10.1530/EJE-10-1039 (2011).
Chiang, J. K. & Koo, M. Lipid accumulation product: a simple and accurate index for predicting metabolic syndrome in Taiwanese people aged 50 and over. BMC cardiovascular disorders 12, 78, doi:10.1186/1471-2261-12-78 (2012).
Motamed, N., Razmjou, S., Hemmasi, G., Maadi, M. & Zamani, F. Lipid accumulation product and metabolic syndrome: a population-based study in northern Iran, Amol. Journal of endocrinological investigation 39, 375–382, doi:10.1007/s40618-015-0369-5 (2016).
Schuster, J., Vogel, P., Eckhardt, C. & Morelo, S. D. Applicability of the visceral adiposity index (VAI) in predicting components of metabolic syndrome in young adults. Nutricion hospitalaria 30, 806–812, doi:10.3305/nh.2014.30.4.7644 (2014).
de Oliveira, C. C., Roriz, A. K., Ramos, L. B. & Gomes Neto, M. Indicators of Adiposity Predictors of Metabolic Syndrome in the Elderly. Annals of nutrition & metabolism 70, 9–15, doi:10.1159/000455333 (2017).
Goldani, H. et al. Applicatility of the Visceral Adiposity Index (Vai) in the Prediction of the Components of the Metabolic Syndrome in Elderly. Nutricion hospitalaria 32, 1609–1615, doi:10.3305/nh.2015.32.4.9589 (2015).
Xiang, S. et al. Lipid accumulation product is related to metabolic syndrome in women with polycystic ovary syndrome. Experimental and clinical endocrinology & diabetes: official journal, German Society of Endocrinology [and] German Diabetes Association 121, 115–118, doi:10.1055/s-0032-1333261 (2013).
Macut, D. et al. Lipid accumulation product is associated with metabolic syndrome in women with polycystic ovary syndrome. Hormones (Athens, Greece) 15, 35–44, doi:10.14310/horm.2002.1592 (2016).
Techatraisak, K., Wongmeerit, K., Dangrat, C., Wongwananuruk, T. & Indhavivadhana, S. Measures of body adiposity and visceral adiposity index as predictors of metabolic syndrome among Thai women with PCOS. Gynecological endocrinology: the official journal of the International Society of Gynecological Endocrinology 32, 276–280, doi:10.3109/09513590.2015.1112785 (2016).
Chan, L. et al. Lipid Accumulation Product: a Simple and Accurate Index for Predicting Metabolic Syndrome in Patients with Adult Growth Hormone Deficiency. Experimental and clinical endocrinology & diabetes: official journal, German Society of Endocrinology [and] German Diabetes Association 124, 220–224, doi:10.1055/s-0035-1569402 (2016).
Yang, R. F., Liu, X. Y., Lin, Z. & Zhang, G. Correlation study on waist circumference-triglyceride (WT) index and coronary artery scores in patients with coronary heart disease. European review for medical and pharmacological sciences 19, 113–118 (2015).
American Diabetes, A. Diagnosis and classification of diabetes mellitus. Diabetes care 37 Suppl 1, S81-90, doi:10.2337/dc14-S081 (2014).
Amato, M. C. et al. Visceral Adiposity Index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes care 33, 920–922, doi:10.2337/dc09-1825 (2010).
Kahn, H. S. The “lipid accumulation product” performs better than the body mass index for recognizing cardiovascular risk: a population-based comparison. BMC cardiovascular disorders 5, 26, doi:10.1186/1471-2261-5-26 (2005).
Society, C. D. Chinese guideline for type 2 diabetes. Chin J Endocrinol Metab 30, 893–942 (2014).
Zou, K. H., O’Malley, A. J. & Mauri, L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation 115, 654–657, doi:10.1161/CIRCULATIONAHA.105.594929 (2007).
Nazare, J. A. et al. Usefulness of measuring both body mass index and waist circumference for the estimation of visceral adiposity and related cardiometabolic risk profile (from the INSPIRE ME IAA study). The American journal of cardiology 115, 307–315, doi:10.1016/j.amjcard.2014.10.039 (2015).
Lim, J. S. et al. Optimal Waist Circumference Cutoff Value Based on Insulin Resistance and Visceral Obesity in Koreans with Type 2 Diabetes. Diabetes & metabolism journal 39, 253–263, doi:10.4093/dmj.2015.39.3.253 (2015).
Ashwell, M. & Hsieh, S. D. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. International journal of food sciences and nutrition 56, 303–307, doi:10.1080/09637480500195066 (2005).
Ashwell, M., Gunn, P. & Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obesity reviews: an official journal of the International Association for the Study of Obesity 13, 275–286, doi:10.1111/j.1467-789X.2011.00952.x (2012).
Ruderman, N., Chisholm, D., Pi-Sunyer, X. & Schneider, S. The metabolically obese, normal-weight individual revisited. Diabetes 47, 699–713 (1998).
Samocha-Bonet, D., Chisholm, D. J., Tonks, K., Campbell, L. V. & Greenfield, J. R. Insulin-sensitive obesity in humans - a ‘favorable fat’ phenotype? Trends in endocrinology and metabolism: TEM 23, 116–124, doi:10.1016/j.tem.2011.12.005 (2012).
Mirmiran, P., Bahadoran, Z. & Azizi, F. Lipid accumulation product is associated with insulin resistance, lipid peroxidation, and systemic inflammation in type 2 diabetic patients. Endocrinology and metabolism (Seoul, Korea) 29, 443–449, doi:10.3803/EnM.2014.29.4.443 (2014).
Sambataro, M. et al. Lipid accumulation in overweight type 2 diabetic subjects: relationships with insulin sensitivity and adipokines. Acta diabetologica 50, 301–307, doi:10.1007/s00592-011-0366-x (2013).
Guo, S. X. et al. Visceral Adiposity and Anthropometric Indicators as Screening Tools of Metabolic Syndrome among Low Income Rural Adults in Xinjiang. Scientific reports 6, 36091, doi:10.1038/srep36091 (2016).
Kim, H. I. et al. Gender differences in diagnostic values of visceral fat area and waist circumference for predicting metabolic syndrome in Koreans. J Korean Med Sci 26, 906–913, doi:10.3346/jkms.2011.26.7.906 (2011).
Ishibashi, E. et al. Waist circumference correlates with hepatic fat accumulation in male Japanese patients with non-alcoholic fatty liver disease, but not in females. Journal of gastroenterology and hepatology 23, 908–913, doi:10.1111/j.1440-1746.2008.05366.x (2008).
Author information
Authors and Affiliations
Contributions
Fuzai Yin conceptualized and designed the study. Chunming Ma and Na Lu analyzed the data and drafted the initial manuscript. Rui Wang, Xiao-Li Liu and Qiang Lu revised it critically for important intellectual content.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ma, CM., Lu, N., Wang, R. et al. Three novel obese indicators perform better in monitoring management of metabolic syndrome in type 2 diabetes. Sci Rep 7, 9843 (2017). https://doi.org/10.1038/s41598-017-10446-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-10446-3
This article is cited by
-
Assessing the predictive value of insulin resistance indices for metabolic syndrome risk in type 2 diabetes mellitus patients
Scientific Reports (2024)
-
Association between anthropometric indices and hyperuricemia: a nationwide study in China
Clinical Rheumatology (2024)
-
Relationship between body adiposity parameters and insulin resistance: a preliminary study of surrogate markers in Japan
Hormones (2024)
-
Cardiometabolic Index (CMI), Lipid Accumulation Products (LAP), Waist Triglyceride Index (WTI) and the risk of acute pancreatitis: a prospective study in adults of North China
Lipids in Health and Disease (2023)
-
Cut-off values and clinical efficacy of body roundness index and other novel anthropometric indices in identifying metabolic syndrome and its components among Southern-Indian adults
Diabetology International (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
