
Abstract
The oral microflora is composed of both health-promoting as well as disease-initiating bacteria. Many of the disease-initiating bacteria are anaerobic and include organisms such as Porphyromonas gingivalis, Prevotella intermedia, Fusobacterium nucleatum, and Tannerella forsythia. Here we investigated a novel therapeutic, amixicile, that targets pyruvate:ferredoxin oxidoreductase (PFOR), a major metabolic enzyme involved in energy generation through oxidative decarboxylation of pyruvate. PFOR is present in these anaerobic pathogenic bacteria and thus we hypothesized that amixicile would effectively inhibit their growth. In general, PFOR is present in all obligate anaerobic bacteria, while oral commensal aerobes, including aerotolerant ones, such as Streptococcus gordonii, use pyruvate dehydrogenase to decarboxylate pyruvate. Accordingly, we observed that growth of the PFOR-containing anaerobic periodontal pathogens, grown in both monospecies as well as multispecies broth cultures was inhibited in a dose-dependent manner while that of S. gordonii was unaffected. Furthermore, we also show that amixicile is effective against these pathogens grown as monospecies and multispecies biofilms. Finally, amixicile is the first selective therapeutic agent active against bacteria internalized by host cells. Together, the results show that amixicile is an effective inhibitor of oral anaerobic bacteria and as such, is a good candidate for treatment of periodontal diseases.
Similar content being viewed by others


Introduction
Periodontitis is an oral inflammatory disease that affects half of the United States adult population and disproportionally affects the aging population1, 2. It is initiated by bacteria that trigger the host inflammatory response, eventually leading to irreversible bone resorption and tooth loss. Although the oral microbiota consists of over 700 bacterial species, only a small portion leads to disease development and progression3, 4. In a healthy oral condition, the majority of bacterial species are Gram positive, such as Streptococcus sp. Once this population shifts towards a more dominant Gram negative anaerobic population, disease progression begins with gingivitis and continues towards more severe periodontal diseases5, 6. Among the periodontitis-associated bacteria are Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola, which are part of the so-called red complex7,8,9,10,11. Other bacteria contributing to periodontal disease include Prevotella intermedia, Aggregatibacter actinomycetemcomitans, and Fusobacterium nucleatum 12, 13. Bacteria present in the oral cavity form dental plaque that is mainly a complex microbial biofilm capable of withstanding a variety of mechanical and host defense mechanisms. In addition to colonizing the host in the form of oral biofilms, the bacteria can also be found in saliva, inhabiting the periodontal pocket which is rich in crevicular fluid, as well as attached and internalized by host cells. The latter shields the bacteria from immune defenses, as well as serves as a reservoir for recurrent infections.
Methods for treatment of periodontal disease rely mainly on antimicrobial therapy and include scaling and root planing, followed by antibiotic treatment. The use of antibiotics following surgical therapy has been shown to reduce periodontal pathogen burden when compared to mechanical methods alone or placebo14. Although effective, antibiotic therapy is still problematic. Firstly, most of the antibiotics currently used (such as clindamycin, tetracycline, and amoxicillin) are broad spectrum and thus eliminate both “health-promoting” and “disease-promoting” bacteria15,16,17,18,19. This leaves the treated oral environment ripe for re-infection by periodontal disease-promoting pathogens, as they do not have to compete with resident microflora. Secondly, the semi-selective antimicrobial metronidazole, although specifically inhibiting growth of anaerobic bacteria, is not very commonly used in clinic as it may cause serious side effects such as nausea, neuropathies, and colitis and there are issues with compliance19,20,21,22. Finally, there are concerns with repeated antibiotic interventions that over time will contribute to antimicrobial drug resistance and to dysbiosis, not only for the oral microflora, but also for the gut microbiome, a noted risk factor for development of Clostridium difficile colitis. Thus, there is an urgent need to identify more pathogen-selective drug targets and therapeutics that can overcome these limitations. Such therapeutics could also be used for preventive alteration of the microbiome that would keep at bay the members of pathogenic bacteria, thus preventing onset and progression of periodontal disease.
A promising, druggable target that would selectively affect the disease-promoting bacteria is pyruvate:ferredoxin oxidoreductase (PFOR). PFOR catalyzes the conversion of pyruvate and coenzyme A (CoA) to CO2 and acetyl-CoA and is an important component of many metabolic pathways found in anaerobic bacteria and parasites. Recently, the Hoffman laboratory developed a therapeutic, amixicile, which is a derivative of nitazoxanide (NTZ). NTZ is an FDA-approved therapeutic for the treatment of parasitic infections such as Cryptosporidium, Trichomonas, Entamoeba, and Giardia 23, 24 and shows in vitro activity against a wide range of strictly anaerobic bacteria25, 26. These small molecules inhibit the activity of PFOR by outcompeting pyruvate for binding to the thiamine pyrophosphate (TPP) cofactor of PFOR in the active site27. Studies in the Hoffman laboratory have shown that amixicile is a more potent and soluble derivative of NTZ that is superior in treating Clostridium difficile colitis when compared to the current mainline therapeutics28, 29.
Here we show that the oral anaerobic pathogens associated with periodontal disease are highly susceptible to amixicile and that commensal bacteria that do not express PFOR, such as S. gordonii, are unharmed. Importantly, amixicile was potent against these anaerobes under conditions simulating periodontal disease such as mixed broth cultures, biofilms, as well as in cell cultures. Finally, the action of amixicile was not ablated by the presence of 10% saliva or serum, lending support to potential efficacy in treatment of periodontal disease.
Results
The pyruvate:ferredoxin oxidoreductase (PFOR) pathway is conserved in many oral pathogens
The Kyoto Encyclopedia of Genes and Genomes (KEGG) database was used to determine the presence of genes coding for proteins involved in pyruvate catabolism within bacterial strains of interest. The genomes of oral pathogenic bacteria, P. gingivalis, P. intermedia, F. nucleatum, and T. forsythia, were found to contain genes encoding pyruvate:ferredoxin oxidoreductase (PFOR) (Fig. 1). Similarly, genomes of other anaerobic pathogens, Clostridium perfringes and microaerophile Helicobacter pylori, also contain this pathway. Oral facultative and aerotolerant anaerobic bacteria such as A. actinomycetemcomitans and S. gordonii express pyruvate dehydrogenase (PDH), which is also found in humans (Fig. 1). These data suggest that P. gingivalis, P. intermedia, F. nucleatum, and T. forsythia should be susceptible to amixicile, whereas A. actinomycetemcomitans and S. gordonii would not, as they do not contain the amixicile drug target, PFOR.

Pyruvate metabolism in aerobic and anaerobic bacteria. Under aerobic conditions, bacteria utilize pyruvate dehydrogenase to convert pyruvate into acetyl-CoA and carbon dioxide. Anaerobic bacteria can only grow under reduced oxygen concentrations and use pyruvate: ferredoxin oxidoreductase to convert pyruvate into acetyl-CoA and carbon dioxide.
Bioinformatic analysis of PFOR in oral bacteria
To further verify the possibility that amixicile may inhibit PFOR present in oral anaerobic bacteria, we performed bioinformatic analysis of the PFOR protein sequences present in the bacteria of interest. The crystal structure of PFOR from Desulfovibrio africanus has been published30,31,32. We used that data to gain insight into the structural features of the protein and to what extent the structure is conserved among members of the PFOR family.
In Table 1, we show that there is over 50% identity between the amino acid sequences across the family when compared pairwise. As an example, the PFOR structures between D. africanus and P. gingivalis are highly conserved (Fig. 2a,b). Importantly, the TPP binding domain is highly conserved among PFORs as catalytic function is dependent on TPP being maintained in a V shape33. The Glu66 is a conserved residue that is important for stabilization of the ylide conformation necessary for formation of the C2 carbanion on the thiazolium ring (Fig. 2c). In this configuration, the N4′ aminopyrimidine moiety is positioned close to the C2 carbanion of the thiazole, thus favoring interaction with the carbonyl carbon of pyruvate (Fig. 2c). Amixicile and parent compound NTZ attack this activated TPP complex. Modeling studies (Fig. 2d) reveal that the anionic nitro group of amixicile competes with pyruvate for the protonated N4′ amino group of TPP27. Kinetic studies had previously shown that the Km for amixicile and NTZ is over two orders of magnitude lower than the Km for pyruvate23, 24. Deprotonation of the N4′ aminopyrimidine by amixicile inactivates the catalytic cycle of PFOR. Protonation temporarily inactivates amixicile, but the proton is rapidly lost to water (pKa 6.2) in reactivation of the anionic state of amixicile27. Given the catalytic mechanism and high degree of conservation among PFORs, we predicted that amixicile would show selective toxicity for the oral anaerobes27.

Conservation of the pyruvate:ferredoxin/flavodoxin oxidoreductase. (a) Overlay of the Desulfovibrio africanus crystal structure (PDB id: 2C3O) PFOR (blue) and homology model of P. gingivalis PFOR (red) monomer forms of the protein. The overlaid structures share an RMSD of 0.189 Å. The active site of the enzyme is highlighted by a black box. (b) The active site of the P. gingivalis PFOR where the enzyme catalyzes the interconversion of pyruvate and Acetyl-CoA. (c) Position and orientation of the TPP cofactor and pyruvate in the active site is maintained by conserved residues. (d) Proton abstraction mechanism of amixicile. The 5-nitro group of amixicile (AMIX) mimics the carbonyl carbon of pyruvate in forming a hydrogen bond with the aminopyrimidine of TPP. The highly conserved Arg114 of PFOR is predicted to also interact with the nitro group. In the process, anionic AMIX becomes protonated and NMR studies show that the proton localizes to the nitro or the ring nitrogen. TPP is now inactive until PFOR recycling reactivates the carbanion on the thiazole ring. Protonated AMIX loses the proton to water and the anion is restored.
Amixicile inhibits growth of anaerobic bacteria
We first examined the effect of amixicile on the growth of oral anaerobic pathogens associated with periodontal disease. As shown in Fig. 3, amixicile inhibited growth of P. gingivalis W83, P. intermedia 17, and F. nucleatum 25586. The inhibitory effect was similar to that of metronidazole, a known antibiotic active against anaerobic bacteria. From those studies we continued using the antibiotic concentration of 1 µg/mL, or even higher for biofilms and host-pathogen interactions (5 µg/mL), to ensure that growth of P. intermedia was inhibited. Thus, bacterial strains were grown anaerobically for 24 hr with 0, 1, 5 or 10 µg/mL of amixicile or clindamycin. T. forsythia was grown for 96 hr due to its slow growth rate. As shown in Fig. 4, growth of P. gingivalis, P. intermedia, F. nucleatum, and T. forsythia was inhibited in the presence of 1 µg/mL amixicile. A similar inhibition profile was seen with 5 µg/mL and 10 µg/mL amixicile. Clindamycin, used clinically to treat periodontal infection, also inhibited growth of the bacteria as expected. We also tested the susceptibility of S. gordonii to amixicile, since it lacks the drug target and utilizes PDH to metabolize pyruvate. As shown in Fig. 4e, growth of this bacterium was not affected by amixicile, indicating that this therapeutic specifically targets bacteria that use PFOR for energy generation. Another oral pathogen, A. actinomycetemcomitans, which also uses PDH for pyruvate metabolism (Fig. 1) was slightly inhibited at 5 and 10 µg/mL amixicile (Fig. 4c). Additional experiments were conducted to verify growth inhibition in cultures incubated for a prolonged period of time. P. gingivalis and S. gordonii were grown for 96 hr with 0, 1, 5 or 10 µg/mL amixicile. Growth yields, as shown in Fig. 4g,h, were similar at all times monitored: 24, 48, 72 and 96 hr. Finally, dose-dependent inhibition was done using concentrations of amixicile ranging from 0-10 µg/mL to determine the minimal inhibitory concentration (MIC) for each bacterium. F. nucleatum and T. forsythia were susceptible to 0.5 µg/mL, P. gingivalis was affected by 1 µg/mL, and P. intermedia was inhibited at 2 µg/mL (Supplemental Fig. 1). Growth of A. actinomycetemcomitans and S. gordonii was not affected by concentrations of amixicile as high as 3 µg/mL, indicating that the bacteria are not sensitive to that therapeutic.

Effect of amixicile on growth of anaerobic bacteria. Overnight cultulres of a) P. gingivalis W83, b) P. intermedia 17 and c) F. nucleatum 25586 were inoculated into BHI broth containing either amixicile (5 µg/mL) or metronidazole (5 µg/mL) to an OD600 of 0.05 under anaerobic conditions. Cultures grown in BHI without antibiotics (untreated) served as control. The bacteria were grown for 24 hr and growth of the bacteria was monitored by measuring OD600 at 0, 4, 8 and 24 hr. Means and SD from two biological replicates performed in technical triplicates are shown.

Amixicile inhibits growth of anaerobic bacteria. Bacterial strains: (a) P. gingivalis W83, (b) P. intermedia 17, (c) A. actinomycetemcomitans 33384, (d) F. nucleatum 25586, (e) T. forsythia 43037, and (f) S. gordonii 10558 were cultured in BHI broth with or without amixicile (1, 5, and 10 µg/mL) and the OD600 was measured at 24 hr. Clindamycin (10 µg/mL) was used as a positive control. (g) P. gingivalis and (h) S. gordonii were cultured in BHI broth containing various concentrations of amixicile (0, 1, 5 and 10 µg/mL) and the microbial growth was monitored over 96 hr. Results are expressed as mean ± SD. Statistical analysis was done by ANOVA. *p < 0.0332, **p < 0.0021, ***p < 0.0002 and ****p < 0.0001 compared to the untreated control.
In conclusion, amixicile at 1 µg/mL significantly inhibited growth of a variety of oral anaerobic bacteria up to 96 hr (as shown using P. gingivalis) but had no effect on PFOR-lacking bacteria, such as S. gordonii, at any of the time points measured (Fig. 4g,h).
Amixicile specifically inhibits growth of anaerobic bacteria in multispecies cultures
To investigate a more clinically relevant model, multispecies broth cultures were used to examine the effect of amixicile on growth inhibition of the PFOR-containing bacteria. Equivalent amounts of P. gingivalis, P. intermedia, A. actinomycetemcomitans, F. nucleatum, T. forsythia, and S. gordonii were used to inoculate a multispecies broth culture and growth was monitored for 48 hr. The yield of mixed species cultures was monitored in the presence of amixicile and compared to those incubated with metronidazole or grown without antibiotics. To determine specific inhibition of the anaerobic bacteria in the multispecies cultures, DNA was isolated from the cultures and levels of bacteria were determined using qPCR analysis. The analysis has shown that amixicile inhibited growth when compared to the untreated control group of all PFOR-containing bacteria: P. gingivalis, P. intermedia, F. nucleatum, and T. forsythia (Fig. 5). Similar results were obtained using metronidazole. In contrast, neither antimicrobial affected growth of S. gordonii (Fig. 5), indicating selectivity for both therapeutics. Also, the growth of A. actinomycetemcomitans was inhibited only in the presence of high concentrations of amixicile (5 µg/mL and 10 µg/mL) (Figs 4 and 5). These data demonstrate that amixicile is an effective inhibitor of growth of P. gingivalis, P. intermedia, F. nucleatum, and T. forsythia when the bacteria are grown in multispecies cultures.

Amixicile inhibits oral pathogens in multispecies broth culture. Bacterial strains were inoculated in BHI broth at an OD600 of 0.05. Broth cultures contained 10 µg/mL amixicile, 10 µg/mL metronidazole, or were left unsupplemented. 1 OD600 of each culture was harvested at 48 hr and quantified by qPCR. Pg – P. gingivalis W83, Pi – P. intermedia 17, Aa – A. actinomycetemcomitans 33384, Fn – F. nucleatum 25586, Tf – T. forsythia 4303l7, Sg – S. gordonii 10558. Results are expressed as mean ± SD compared to the untreated control from experiments performed in triplicate. Statistical analysis was done by ANOVA. *p < 0.0332, **p < 0.0021, ***p < 0.0002 and ****p < 0.0001 compared to the untreated control.
Saliva and serum do not reduce the inhibitory activity of amixicile
To determine the effect of more in vivo-like conditions, we tested the inhibitory activity of amixicile on bacteria grown in the presence of 10% saliva or serum. The multispecies cultures were prepared as above and levels of bacteria were determined using qPCR. The qPCR results shown in Fig. 6 with the A. actinomycetemcomitans and S. gordonii primers showed no significant reduction in growth resulting from the presence of amixicile in any of the media tested when compared to the untreated control. Growth of A. actinomycetecomitans was even upregulated in saliva and serum. While statistically significant, less than 2-fold upregulation of S. gordonii was observed compared to the untreated control. This is expected, given that A. actinomycetemcomitans and S. gordonii are not susceptible to amixicile. P. gingivalis, P. intermedia, and T. forsythia had similar growth patterns in BHI, 10% saliva, and 10% serum. F. nucleatum showed a higher susceptibility to amixicile in BHI than in 10% saliva or 10% serum but it was still significantly affected in all three media tested. These results indicate that amixicile should be effective in reducing bacterial growth in the oral cavity where either saliva or serum are present.

Effect of saliva and serum on the inhibitory activity of amixicile. Bacterial strains: (a) P. gingivalis W83, (b) P. intermedia 17, (c) A. actinomycetemcomitans 33384, (d) F. nucleatum 25586, (e) T. forsythia 43037, and (f) S. gordonii 10558. The absolute fold change between amixicile-treated bacteria and controls grown in different media were determined by qPCR. Multispecies cultures were grown anaerobically overnight in BHI or BHI supplemented with either 10% filtered human saliva or 10% filtered human serum in the presence of 0 (control), 0.5, 1 or 5 μg/mL amixicile. Genomic DNA was isolated from cultures grown for 24 hr and qPCR was run with 16s species-specific primers. Results are expressed as mean ± SD of amixicile-treated sample compared to the untreated control from experiment performed in triplicate. Statistical analysis was done by ANOVA. *p < 0.0332, **p < 0.0021, ***p < 0.0002 and ****p < 0.0001 compared to the untreated control.
Amixicile prevents maturation of P. gingivalis biofilms, but not of S. gordonii
Oral bacteria form biofilms known as dental plaque that aid in bacterial survival within the host. Therefore, we cultured P. gingivalis and S. gordonii in the form of monospecies biofilms for 24 hr and treated the biofilms with amixicile for an additional 24 hr. Our results show that the level of biofilm formation for the 5 µg/mL amixicile-treated P. gingivalis after 48 hr is comparable to that of the 24 hr control showing the level of biofilm prior to amixicile addition (Fig. 7). Furthermore, a higher dose of amixicile (10 µg/mL) reduced the biofilm volume after 24 hr treatment when compared to the control biofilm (Fig. 7). As expected, amixicile did not have an effect on the volume of S. gordonii biofilms as the levels of the biofilm nearly doubled despite the presence of amixicile when compared to the 24 hr control biofilm. These results suggest that amixicile can be used to inhibit growth and prevent formation of biofilms by P. gingivalis while not affecting the growth and biofilm formation of primary colonizers such as S. gordonii.

P. gingivalis monospecies biofilm maturation is inhibited by amixicile. (a) P. gingivalis 33277 and (b) S. gordonii 10558 biofilms were cultured in BHI for 24 hr. After 24 hr, fresh media containing 0, 5, or 10 µg/mL amixicile was added and the biofilms were incubated for an additional 24 hr. Biofilm volumes were measured by crystal violet staining at OD550. Results were compared to the untreated 48 hr control group. All experiments were performed in triplicate. Statistical analysis was done by ANOVA. *p < 0.0332, **p < 0.0021, ***p < 0.0002 and ****p < 0.0001 compared to the untreated control.
Amixicile selectively inhibits anaerobic bacteria in multispecies biofilms
Oral biofilms are comprised of many different species of bacteria; therefore we tested the effectiveness of amixicile against a multispecies in vitro biofilm model. Four day-old biofilms were treated with amixicile, metronidazole, or left untreated for five additional days. Biofilm DNA was harvested for qPCR analysis by 16S gDNA. Results show that amixicile and metronidazole inhibit P. gingivalis, P. intermedia, F. nucleatum, and T. forsythia levels in the biofilm starting with 10 µg/mL of amixicile, but A. actinomycetemcomitans and S. gordonii were unaffected (Fig. 8). This suggests that amixicile may potentially be a valuable tool in combating oral biofilms in vivo by selectively inhibiting many oral pathogens.

Amixicile selectively inhibits growth of anaerobes in a multispecies biofilm model. Four day-old multispecies biofilms were treated with 10 µg/mL a), 20 µg/mL b), and 50 µg/mL c) amixicile or metronidazole. Untreated biofilms served as controls. The biofilms were incubated for five additional days with daily growth media replacement. Bacteria were then collected and DNA was harvested for qPCR analysis. Results shown are mean ± SD compared to the untreated control from an experiment performed in triplicate. Pg – P. gingivalis 33277, Pi – P. intermedia 17, Aa – A. actinomycetemcomitans 33384, Fn – F. nucleatum 25586, Tf – T. forsythia 43037, Sg – S. gordonii 10558.
Live/dead staining of bacteria exposed to amixicile
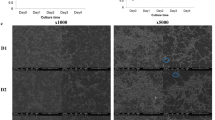
Amixicile inhibits the activity of PFOR thus reducing energy generation by the bacteria. To determine the bactericidal or bacteriostatic action of amixicile, we performed staining for live/dead bacteria. As shown in Fig. 9, as the dosage of amixicile increased, the total number of bacterial cells decreased. The green stain represents live cells while the red stain indicates dead cells, since propidium iodide cannot break through an intact cell membrane. Occasionally the stains overlap, particularly as seen in the heat-killed samples serving as a control for our studies, showing a yellow color, which also indicates dead cells. As the concentration of amixicile increased, both the total number of cells and the percentage of live cells decreased. Clindamycin was used as a bacteriostatic control and metronidazole and heat as bactericidal controls. All treatments, excluding heat, were bacteriostatic at early time points. The number of cells was reduced at 2 hr (Fig. 9a) but the cells were alive according to the green stain. At 24 hr, however, it was clear that amixicile is bactericidal as we detected cells that were stained in red. In conclusion, amixicile at high doses shows similar effectiveness to metronidazole.

Live/dead staining to determine the mechanism of amixicile. (a) P. intermedia was grown for up to 24 hr with amixicile, clindamycin, metronidazole, or without antimicrobial. Representative fluorescence microscopy images are shown. The green stain indicates live cells. Red or yellow color indicates dead cells. Cells were manually counted as live or dead. (b) Total number of cells, with the number of live cells in parentheses counted for this experiment. (c) Percentage of live cells.
Colonization of eukaryotic cells by oral bacteria is inhibited by amixicile
Many oral pathogens have adapted to the oral cavity by invading host cells to avoid destruction by the immune response34. Similarly, oral bacteria were found to invade a variety of other eukaryotic cells including the human umbilical cord endothelial cells (HUVECs)27. To determine if amixicile is effective against bacteria associated with host cells (both internalized and bound to host cells), monolayers of human oral keratinocytes (HOKs) and HUVECs were challenged with oral bacteria and then treated with amixicile, metronidazole, or left untreated. The infected eukaryotic cells were lysed at 24 hr post-treatment and viable bacteria (enumerated as CFUs) were determined according to a published protocol35. Cells treated with amixicile and metronidazole displayed significant reduction in the number of viable bacteria when compared to the untreated control group (Fig. 10). While in the presence of metronidazole, some live bacteria were still observed. No colonies were obtained using HOKs and HUVECs infected with P. intermedia or F. nucleatum when incubated in the presence of 10 µg/mL amixicile. This provides evidence that amixicile can affect both intra- and extracellular bacteria. These results were visually confirmed by confocal microscopic analysis (Supplemental Fig. 2). While bacteria were noted in the untreated HUVECs, no bacteria were detected in either the metronidazole- or amixicile-treated cells.

Amixicile inhibits bacterial colonization of HOKs and HUVECs. HOKs (a and b) and HUVECs (c) were challenged with oral bacteria (a,c - P. intermedia 17, b – F. nucleatum) at an MOI of 1:100 for 24 hr with and without the addition of amixicile or metronidazole. CFU counts of colonization at 24 hr as observed on blood agar plates seven days post-infection. Data from three biological replicates performed in duplicate are presented.
Discussion
The oral microbiome is very dynamic and it can change its composition, eventually leading to either healthy or diseased states of the host, mainly through altering the abundance of bacterial species. Previous work has shown that a “healthy” microbiome is composed primarily of Gram positive bacteria such as streptococci, with a small proportion of pathogenic Gram negative anaerobes6. The shift towards the diseased microbiome involves acquisition of a larger proportion of Gram negative anaerobic bacteria such as P. gingivalis and T. forsythia that ultimately leads to activation of host response and development of periodontal disease (PD)4, 36, 37. Our bioinformatics analysis shows that PFOR is present in the pathogenic bacteria, while it is absent in the commensal streptococci. We performed our bioinformatics analysis on a limited number of bacteria, only those used in our study, and compared our results to bacteria in which PFOR was successfully targeted by amixicile, such as Clostridium difficile and Helicobacter pylori 28, 38. Our data sets the platform for a future, more comprehensive, systems biology approach, where all available genomes for oral bacteria will be scrutinized for the presence of PFOR.
We noted high conservation of the PFOR enzyme across genera, suggesting that this is an essential enzyme for the bacteria and required for proper metabolic activity. Specifically, many of the residues vital to the catalytic activity and coordination of both the pyruvate and TPP cofactor are conserved across all of the species we observed. This is fortunate as recent docking studies reveal that amixicile binds at the same site as pyruvate and interacts with the aminopyrimidine of the TPP25. Such similarity in the active site bodes well for the effectiveness of PFOR inhibition by amixicile in bacteria relying on the enzyme for energy production.
Our MIC studies show amixicile to be effective at inhibiting growth of P. gingivalis, F. nucleatum, and T. forsythia at 1 µg/mL. A higher dose, 5 µg/mL, was required to inhibit growth of P. intermedia. However, it is noteworthy that even at 10 µg/mL, no inhibition of S. gordonii is observed. This bacterium does not rely on the PFOR enzyme for energy generation and thus was expected to have a consistent growth rate unaffected by amixicile. A. actinomycetemcomitans also does not encode PFOR and was not expected to be inhibited by amixicile. However, approximately a 10% reduction in growth rate was observed with 10 µg/mL amixicile indicating that amixicile could possibly affect the growth of the bacterium through a non-PFOR-related mechanism. A slight effect of NTZ and amixicile on bacteria not expressing PFOR was reported previously39, 40.
Our data demonstrating that amixicile is effective in multispecies broth cultures indicates that the therapeutic will be effective in in vivo conditions where multiple bacteria are found. We used a dose of 10 µg/mL, which is equivalent to a dose of 500 mg for an approximately 130 lb patient. This dose was also effective to inhibit growth of the bacteria when grown as biofilms and thus would be relevant as such a dose is used clinically40. It is noteworthy that inhibition of PFOR-containing bacteria in the multispecies mixtures was also seen with 5 µg/mL (results not shown), further reinforcing that the bactericidal dosage will be applicable to an in vivo setting.
Our assumption is further reinforced by our studies performed in the presence of either saliva or serum, the two major factors that may affect the inhibitory activity of amixicile. F. nucleatum seemed to be the most susceptible to amixicile in our multispecies study in all three types of media tested. T. forsythia, although a slow-growing organism, still had significantly reduced growth rates in all media tested. P. gingivalis and P. intermedia were reduced less than expected based on the monospecies broth studies. Nevertheless, the 5 µg/mL of amixicile was an effective inhibitor of growth of those organisms in either saliva or serum. It has been shown previously that S. gordonii and other bacteria commonly found in the oral cavity can provide some protection for P. gingivalis and P. intermedia during a periodontal disease state and in times of stress. That may have evidenced itself in our multispecies cultures compared to the monospecies cultures as higher antibiotic dosage was required to inhibit growth of the anaerobes when the bacteria were grown in the six-species biofilm41.
Amixicile inhibits the growth of these pathogens at 1 µg/mL and completely abolishes growth at 5 and 10 µg/mL. Monospecies biofilm maturation is inhibited at 5 and 10 µg/mL amixicile. In these experiments, amixicile was tested against pre-formed biofilms. It has been shown that biofilms are more resistant to antibiotic action due to reduced penetration of antibiotics into the biofilm structures as well as an increase in the number of persister cells resistant to the antibiotic42. Therefore, a higher dose of antibiotic is required, in order for it to be effective against the layers of bacteria present in the biofilm. In multispecies biofilms particularly, many bacteria are protective against each other. It is noteworthy that S. gordonii growth, both in broth and biofilm maturation is not affected by amixicile at 5 or 10 µg/mL. This is a primary colonizer and thus a health-promoting bacterium.
Amixicile aids in reducing the colonization of oral bacteria in both HOKs and in HUVECs. Amixicile has been shown to be internalized by Caco-2 cell monolayers38 and this may explain why we observed the reduction of the live internalized bacteria. Most antibiotics are not taken up by eukaryotic cells and thus are not effective in reducing the intracellular microbial burden. Amixicile is thus unique in this aspect, as it will also reduce the levels of intracellular bacteria that alter host cell functions, as well as serve as a reservoir for future re-infections. This is highly significant considering the occurrence of recurrent infections due to the internalized bacteria that are not eliminated during standard periodontal therapy17, 43.
Another problem emerging in the treatment of oral infections is antibiotic resistance44. Antibiotic resistance develops as bacteria either mutate to avoid a drug’s mechanism of action or acquire the ability to export the antibiotic. Amixicile is highly novel in this regard, as the mechanism of action disrupted is the cofactor of PFOR, thiamine pyrophosphate, rather than the microbial enzyme itself, thus reducing the possibility of developing resistance to amixicile by mutation25. As noted in Kennedy et al.25, there have been no reports of drug resistance in the clinical use of nitazoxanide (NTZ), which might be an indicator of the potential longevity of this class of antimicrobials and the unique nature of mechanistic action.
Our studies show that amixicile is highly specific and affects bacteria that have the PFOR pathway. This is highly significant, as many bacteria that cause periodontal disease are indeed anaerobic and do encode PFOR. The therapeutic potential of amixicile may also have further use as the oral anaerobic bacteria also play a role in systemic diseases45 and even cancer46, 47. This is reinforced by recent findings that H. pylori is associated with higher numbers of periodontal pathogens, such as P. gingivalis, in the oral cavity, as well as is a major etiological agent in cancer development48. Targeting the pathogenic bacteria and sparing the beneficial ones will have significant potential not only for treatment of diseases but, most importantly, for preventive measures where the levels of pathogenic bacteria in microbiomes could be reduced, possibly converting such microbiomes to health-promoting ones.
Treatment of periodontal disease is primarily based on mechanical methods such as scaling and root planing to reduce of the microbial burden. Antibiotics are usually used as adjunct therapy in more severe cases due to their effect on the total microbial flora of the patient as well as the risk for development of antibiotic resistance. The antibiotics used are mostly broad-spectrum ones, thus affecting the total microbiome, both the aerobic health-promoting bacteria as well as the pathogenic anaerobic bacteria. However, several studies have shown that the use of metronidazole, a redox-active prodrug that is activated by PFOR and thus is effective against anaerobic bacteria, is as effective as mechanical methods (scaling and root planing) in treatment of periodontal disease49,50,51. Furthermore, metronidazole also reduced the need for periodontal surgery52. Such promising results of the use of antibiotic therapy in treatment of periodontal disease were halted by the toxic nature of metronidazole, as well as concerns about the development of antibiotic resistance52. Thus, metronidazole would not be a viable antibiotic for treatment of a widespread condition such as periodontal disease. Several attributes of amixicile, a novel antimicrobial targeting the anaerobic pyruvate:ferredoxin oxidoreductase (PFOR) and related enzymes, suggest it might be amenable to treatment of PD and include: (1) it is readily absorbed (systemic bioavailability), (2) it does not accumulate in or alter the gut microbiome, (3) it is well-tolerated (nontoxic) in animal models and (4) it has the ability to concentrate in areas of inflammation (serum leakage)38. The latter might prove beneficial to PD where concentration in crevicular fluid would be highly desired. Here we show that amixicile exhibits excellent in vitro activity against the oral anaerobes associated with PD. Although it has similar inhibitory activity to that of metronidazole in our in vitro studies, amixicile was more effective in eliminating bacteria in animal models of colitis38. Thus, based on the efficacy studies as well as the lack of toxicity, combined with the ability of the therapeutic to concentrate in areas with increased inflammation and spare healthy tissues, amixicile is a highly desirable treatment method that has the potential to change the way periodontal diseases will be treated.
Materials and Methods
Bacterial strains and culture conditions
Microbial strains Porphyromonas gingivalis W8353,54,55, Porphyromonas gingivalis 33277 (ATCC), Prevotella intermedia 1734, 56 (Leung Lab), Prevotella intermedia OMA 14, Aggregatibacter actinomycetemcomitans 33384 (ATCC), Fusobacterium nucleatum 25586 (ATCC), Tannerella forsythia 43037 (ATCC), and Streptococcus gordonii 10558 (ATCC) were maintained in an artificial atmosphere (composed of 80% N, 10% H, and 10% CO2) at 37 °C using a Coy anaerobic chamber (Ann Arbor, MI). Bacterial strains were cultured on blood agar plates (BAP) and in brain heart infusion (BHI) broth containing 5 µg/mL hemin (Sigma) and 0.2 µg/mL menadione (vitamin K). Additionally, 5% Fetal Bovine Serum (ΔFBS) and 10 µg/mL N-acetyl muramic acid (Sigma) was added to T. forsythia cultures. All media were pre-equilibrated anaerobically for at least 12 hr prior to being used in our experiments.
Mono- and multispecies growth studies
Bacteria from blood agar plates were used to establish broth cultures. The bacteria were grown for 48 hr and then used as inoculum for an overnight (O/N) culture. That culture was then used to inoculate aliquots of BHI broth supplemented with various concentrations of amixicile (initial culture OD600 of 0.1 and containing amixicile at 0, 1, 5 or 10 µg/mL). Clindamycin, an antibiotic known to be an effective inhibitor for all bacteria used in our study, was used as a positive control for inhibition of bacterial growth. Bacterial growth was monitored by measuring the absorbance at OD600 for up to 96 hr. For the multispecies culture experiments, all bacterial species were added at the same time, at an OD600 of 0.05 and were incubated with various concentrations of amixicile or metronidazole for 48 hr. To test the effect of saliva and serum on the ability of the antimicrobial to inhibit bacterial growth, BHI supplemented with 10% filtered human saliva (Lee Biosystems) or 10% filtered human serum (Valley Biomedical) were used to prepare both mono- and multispecies cultures.
DNA isolation and qPCR
An OD600 of 1 was used for DNA isolation from the above cultures. Cell pellets were resuspended in 50 mM EDTA containing 10 mg/mL lysozyme and 100 U/mL mutanolysin (Sigma) and incubated at 37°C for 1 hr. The DNA pellets were rehydrated at 65°C for 1 hr in rehydration buffer. DNA was isolated using the Wizard Genomic DNA purification kit (Promega) according to manufacturer’s instructions. The DNA was then used to quantify the presence of bacterial species in the various samples using a 7500 Fast Real-time PCR machine (Thermo-Fisher). Purified DNA (1 µL) and species-specific primers were added to Fast SYBR Green Mastermix (Thermo-Fisher) and run using standard cycle conditions: 95°C for 20 sec (1 cycle); 95°C for 3 sec, 60°C for 30 sec (40 cycles). The species-specific 16S gDNA primer sequences used in this study are shown in Supplemental Table 1. The cycle threshold (Ct) data were collected and then converted to absolute fold change.
Saliva coating of plates for biofilm experiments
Human saliva was obtained from Lee Biosolutions. Saliva (10 mL) was diluted 1:2 in PBS and centrifuged at 5,500 rpm for 15 min at 4 °C. The supernatant was collected and a proteinase inhibitor cocktail tablet (Roche #11836170001) was added, then the solution was filter-sterilized through a 0.22 µM filter (Millex). The conditioned saliva was used to coat wells of 24-well tissue culture-treated plates (Falcon) at 37°C for 30 min and residual saliva was washed off the wells using sterile PBS.
Crystal violet biofilm assays
The formation of monospecies biofilms was determined using crystal violet staining. O/N bacterial cultures were diluted with fresh BHI to an OD600 of 0.1 and then 1 mL was transferred to each well of the 24-well plate. These plates were incubated anaerobically for 24 hr. Media was replaced with BHI containing 0, 5 or 10 µg/mL amixicile for an additional 24 hr. Wells were washed with PBS and stained with crystal violet. Wells were then washed with PBS and dried. 30% acetic acid was then added to each well and the absorbance was read at OD550 using a BioTek Synergy HI Hybrid Plate Reader. T. forsythia was allowed to grow for 96 hr due to its slow growth rate, with amixicile added for the last 24 hr.
Multispecies biofilms
Conditioned saliva was used to coat 12-well tissue culture-treated plates. Wells were washed with PBS to remove residual saliva and BHI broth was added to the wells. The wells were inoculated with 0.05 OD600 of S. gordonii from an O/N culture. After 24 hr, wells were washed with PBS and fresh media was added. O/N cultures of P. gingivalis, P. intermedia, A. actinomycetemcomitans, F. nucleatum, and T. forsythia were added to the wells at an OD600 of 0.05. Fresh media was added every 24 hr for 3 additional days. On the fourth day, BHI containing no drug, and BHI supplemented with 10 µg/mL, 20 µg/mL, and 50 µg/mL amixicile or metronidazole was added to the wells and replaced with fresh antibiotic-containing media every 24 hr up to nine days. Wells were washed with PBS and the remaining biofilm was harvested for DNA isolation and qPCR analysis.
LIVE/DEAD staining
Overnight cultures were diluted to an OD600 of 0.5 in 3 mL of BHI broth containing 0, 1, 5, or 10 μg/mL amixicile. Clindamycin and metronidazole were used as positive controls at 10 μg/mL. At time points 0, 2, and 24 hr, 50 μL of each sample was transferred to a 96-well plate and mixed with 50 μL Live/Dead BacLight Bacterial Viability Kit components (Invitrogen). Further steps were done following manufacturer’s protocol. Briefly, plates were incubated aerobically in the dark for 15 min. Cells were visualized by fluorescence microscopy on the Image Express Micro XLS (Molecular Devices). Images were taken at 60X. All live and dead cells present in the view (numbers are given in Fig. 9) were manually counted to determine total cells and percent live/dead. A representative portion of each original image is shown in Fig. 9.
HOKs and HUVECs colonization assays
Primary Human Oral Keratinocytes (HOKs, ScienCell) and Primary Human Umbilical Vein Endothelial Cells (HUVECs, Lifeline Cell Technology) were maintained at 37°C with 5% CO2 using oral keratinocyte medium (ScienCell) and basal media (Lifeline), respectively. For colonization experiments, HOKs and HUVECs were placed under anaerobic conditions at 37°C with pre-equilibrated media. Oral bacteria were added to monolayers of HOKs or HUVECs for 30 min anaerobically at an MOI of 100:1 in a 12-well tissue culture plate. Wells were washed three times with sterile PBS and media was then replaced with media containing no drug, 10 µg/mL amixicile, or 10 µg/mL metronidazole for 24 hr. Cells from the 12-well plate were lysed to release internalized bacteria and the mixture was spread on blood agar plates to determine colony forming unit (CFU) counts.
Microscopy analysis
Briefly, oral bacteria was grown to mid-log phase and stained with BCECF-AM 0.2 mM solution to a final concentration of 2 µM. The culture was then incubated at 37°C in the dark for 30 min. Cells were pelleted and washed with PBS to remove residual BCECF-AM dye. HUVECs monolayers grown on 8-chamber glass slides were infected at an MOI of 100:1 and then incubated at 37°C for 30 min to allow bacterial binding and internalization. Non-attached bacteria were then washed off with PBS. Amixicile- or metronidazole-supplemented media (antibiotic concentration at 10 µg/mL) was then added and cells were incubated for 20 hr. The slides containing infected HUVECs were then washed 3x with PBS. They were incubated in 4% paraformaldehyde for 10 min, and washed 3x with PBS. 0.2% Triton X-100 was added for 10 min and the slides were again washed 3x with PBS. The cells were then stained with TRITC Phalloidin for 45 min followed by a final wash with PBS. Finally, Vectashield mounting medium with DAPI was added and the cover slides were sealed using nail polish. Images were taken via LSM 710 confocal microscope (Zeiss).
Bioinformatics analysis
The P. gingivalis PFOR 3D homology model was constructed using the one-to-one threading option of the Phyre2 web portal for protein modeling, prediction, and analysis57. The homology model utilized the crystal structure of the D. africanus crystal structure (PDB id: 2C3O) as a template. All models and crystal structures were visualized using UCSF chimera58. Clustal-omega (part of the EMBL-EBI online resources) was utilized to align multiple PFOR protein sequences and generate the sequence identities between the selected bacteria59.
Statistical Analysis
Graphpad Prism 5.0 was used to analyze the results with ANOVA. All experiments were performed in triplicate unless otherwise noted. P values for statistical significance were calculated as follows: *p < 0.0332, **p < 0.0021, ***p < 0.0002 and ****p < 0.0001 compared to the untreated control26, 29, 51.
References
Eke, P. I. et al. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J. Periodontol. 86, 611–622 (2015).
Eke, P. I. et al. Risk Indicators for Periodontitis in US Adults: National Health and Nutrition Examination Survey (NHANES) 2009–2012. J. Periodontol., 1–18 (2016).
Aas, J. A., Paster, B. J., Stokes, L. N., Olsen, I. & Dewhirst, F. E. Defining the normal bacterial flora of the oral cavity. J. Clin. Microbiol. 43, 5721–5732 (2005).
Kumar, P. S. et al. Changes in periodontal health status are associated with bacterial community shifts as assessed by quantitative 16S cloning and sequencing. J. Clin. Microbiol. 44, 3665–3673 (2006).
Sbordone, L. & Bortolaia, C. Oral microbial biofilms and plaque-related diseases: microbial communities and their role in the shift from oral health to disease. Clin. Oral Investig. 7, 181–188 (2003).
Kilian, M. et al. The oral microbiome - an update for oral healthcare professionals. Br. Dent. J. 221, 657–666 (2016).
Ximenez-Fyvie, L. A., Haffajee, A. D. & Socransky, S. S. Microbial composition of supra- and subgingival plaque in subjects with adult periodontitis. J. Clin. Periodontol. 27, 722–732 (2000).
Ximenez-Fyvie, L. A., Haffajee, A. D. & Socransky, S. S. Comparison of the microbiota of supra- and subgingival plaque in health and periodontitis. J. Clin. Periodontol. 27, 648–657 (2000).
Wade, W. G. New aspects and new concepts of maintaining “microbiological” health. J. Dent. 38(Suppl 1), S21–5 (2010).
Wade, W. G. The oral microbiome in health and disease. Pharmacol. Res. 69, 137–143 (2013).
Holt, S. C. & Ebersole, J. L. Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia: the “red complex”, a prototype polybacterial pathogenic consortium in periodontitis. Periodontol. 2000 38, 72–122 (2005).
Stingu, C. S. et al. Microbial profile of patients with periodontitis compared with healthy subjects. Quintessence Int. 43, e23–31 (2012).
van Winkelhoff, A. J., Loos, B. G., van der Reijden, W. A. & van der Velden, U. Porphyromonas gingivalis, Bacteroides forsythus and other putative periodontal pathogens in subjects with and without periodontal destruction. J. Clin. Periodontol. 29, 1023–1028 (2002).
Burmolle, M. et al. Enhanced biofilm formation and increased resistance to antimicrobial agents and bacterial invasion are caused by synergistic interactions in multispecies biofilms. Appl. Environ. Microbiol. 72, 3916–3923 (2006).
Needleman, I. G. et al. Retention, antimicrobial activity, and clinical outcomes following use of a bioerodible tetracycline gel in moderate-to-deep periodontal pockets. J. Periodontol. 69, 578–583 (1998).
Vandekerckhove, B. N., Quirynen, M. & van Steenberghe, D. The use of tetracycline-containing controlled-release fibers in the treatment of refractory periodontitis. J. Periodontol. 68, 353–361 (1997).
Santos, R. S. et al. The use of systemic antibiotics in the treatment of refractory periodontitis: A systematic review. J. Am. Dent. Assoc. 147, 577–585 (2016).
Bidault, P., Chandad, F. & Grenier, D. Systemic antibiotic therapy in the treatment of periodontitis. J. Can. Dent. Assoc. 73, 515–520 (2007).
Ferrer, M., Mendez-Garcia, C., Rojo, D., Barbas, C. & Moya, A. Antibiotic use and microbiome function. Biochem. Pharmacol. pii: S0006-2952(16)30286-6. doi:10.1016/j.bcp.2016.09.007 (2016).
Ohnishi, K. et al. Subjective adverse reactions to metronidazole in patients with amebiasis. Parasitol. Int. 63, 698–700 (2014).
Nitzan, O., Elias, M., Peretz, A. & Saliba, W. Role of antibiotics for treatment of inflammatory bowel disease. World J. Gastroenterol. 22, 1078–1087 (2016).
Agarwal, A., Kanekar, S., Sabat, S. & Thamburaj, K. Metronidazole-Induced Cerebellar Toxicity. Neurol. Int. 8, 6365 (2016).
Hemphill, A., Mueller, J. & Esposito, M. Nitazoxanide, a broad-spectrum thiazolide anti-infective agent for the treatment of gastrointestinal infections. Expert Opin. Pharmacother. 7, 953–964 (2006).
Hoffman, P. S. et al. Antiparasitic drug nitazoxanide inhibits the pyruvate oxidoreductases of Helicobacter pylori, selected anaerobic bacteria and parasites, and Campylobacter jejuni. Antimicrob. Agents Chemother. 51, 868–876 (2007).
Kennedy, A. J. et al. Synthesis and Antimicrobial Evaluation of Amixicile-Based Inhibitors of the Pyruvate-Ferredoxin Oxidoreductases of Anaerobic Bacteria and Epsilonproteobacteria. Antimicrob. Agents Chemother. 60, 3980–3987 (2016).
Pankuch, G. & Appelbaum, P. Activities of tizoxanide and nitazoxanide compared to those of five other thiazolides and three other agents against anaerobic species. Antimicrob Agents Chemother. 50, 1112–1117 (2006).
Dorn, B., Burks, J., Seifert, K. & Progulske-Fox, A. Invasion of endothelial and epithelial cells by strains of Porphyromonas gingivalis. FEMS Microbiol Lett. 187(2), 139–44 (2000).
Warren, C. A. et al. Amixicile, a novel inhibitor of pyruvate: ferredoxin oxidoreductase, shows efficacy against Clostridium difficile in a mouse infection model. Antimicrob. Agents Chemother. 56, 4103–4111 (2012).
Meyer-Baumer, A. et al. Periodontal pathogens and associated factors in aggressive periodontitis: results 5–17 years after active periodontal therapy. J. Clin. Periodontol. 41, 662–672 (2014).
Chabriere, E. et al. Crystal structure of the free radical intermediate of pyruvate:ferredoxin oxidoreductase. Science 294, 2559–2563 (2001).
Chabriere, E., Volbeda, A., Fontecilla-Camps, J. C., Roth, M. & Charon, M. H. Combination of methods used in the structure solution of pyruvate:ferredoxin oxidoreductase from two crystal forms. Acta Crystallogr. D Biol. Crystallogr. 55, 1546–1554 (1999).
Chabriere, E. et al. Crystal structures of the key anaerobic enzyme pyruvate:ferredoxin oxidoreductase, free and in complex with pyruvate. Nat. Struct. Biol. 6, 182–190 (1999).
Cavazza, C. et al. Flexibility of thiamine diphosphate revealed by kinetic crystallographic studies of the reaction of pyruvate-ferredoxin oxidoreductase with pyruvate. Structure 14, 217–224 (2006).
Dorn, B. R., Leung, K. L. & Progulske-Fox, A. Invasion of human oral epithelial cells by Prevotella intermedia. Infect. Immun. 66, 6054–6057 (1998).
Wunsch, C. M. & Lewis, J. P. Porphyromonas gingivalis as a Model Organism for Assessing Interaction of Anaerobic Bacteria with Host Cells. J. Vis. Exp. (106), :e53408, doi:10.3791/JoVE53408 (2015).
Kumar, P. S., Griffen, A. L., Moeschberger, M. L. & Leys, E. J. Identification of candidate periodontal pathogens and beneficial species by quantitative 16S clonal analysis. J. Clin. Microbiol. 43, 3944–3955 (2005).
Griffen, A. L. et al. Distinct and complex bacterial profiles in human periodontitis and health revealed by 16S pyrosequencing. ISME J. 6, 1176–1185 (2012).
Hoffman, P. S. et al. Preclinical studies of amixicile, a systemic therapeutic developed for treatment of Clostridium difficile infections that also shows efficacy against Helicobacter pylori. Antimicrob. Agents Chemother. 58, 4703–4712 (2014).
Chahales, P., Hoffman, P. S. & Thanassi, D. G. Nitazoxanide Inhibits Pilus Biogenesis by Interfering with Folding of the Usher Protein in the Outer Membrane. Antimicrob. Agents Chemother. 60, 2028–2038 (2016).
Tchouaffi-Nana, F. et al. Nitazoxanide inhibits biofilm formation by Staphylococcus epidermidis by blocking accumulation on surfaces. Antimicrob. Agents Chemother. 54, 2767–2774 (2010).
Whitmore, S. E. & Lamont, R. J. The pathogenic persona of community-associated oral streptococci. Mol. Microbiol. 81, 305–314 (2011).
Rogers, G. B., Carroll, M. P. & Bruce, K. D. Enhancing the utility of existing antibiotics by targeting bacterial behaviour? Br. J. Pharmacol. 165, 845–857 (2012).
Johnson, J. D. et al. Persistence of extracrevicular bacterial reservoirs after treatment of aggressive periodontitis. J. Periodontol. 79, 2305–2312 (2008).
Walker, C. The supplemental use of antibiotics in periodontal therapy. Compend. Contin. Educ. Dent. 20, 4–12 quiz 34 (1999).
Han, Y. W. & Wang, X. Mobile microbiome: oral bacteria in extra-oral infections and inflammation. J. Dent. Res. 92, 485–491 (2013).
Abed, J. et al. Fap2 Mediates Fusobacterium nucleatum Colorectal Adenocarcinoma Enrichment by Binding to Tumor-Expressed Gal-GalNAc. Cell. Host Microbe 20, 215–225 (2016).
Han, Y. W. Fusobacterium nucleatum: a commensal-turned pathogen. Curr. Opin. Microbiol. 23, 141–147 (2015).
Hu, Z. et al. Effect of Helicobacter pylori infection on chronic periodontitis by the change of microecology and inflammation. Oncotarget 7(41), 66700–66712 (2016).
Stelzel, M. & Flores-de-Jacoby, L. Topical metronidazole application compared with subgingival scaling. A clinical and microbiological study on recall patients. J. Clin. Periodontol. 23, 24–29 (1996).
Pedrazzoli, V., Kilian, M. & Karring, T. Comparative clinical and microbiological effects of topical subgingival application of metronidazole 25% dental gel and scaling in the treatment of adult periodontitis. J. Clin. Periodontol. 19, 715–722 (1992).
Knoll-Kohler, E. Metronidazole dental gel as an alternative to scaling and root planing in the treatment of localized adult periodontitis. Is its efficacy proved? Eur. J. Oral Sci. 107, 415–421 (1999).
Loesche, W. J., Giordano, J. R., Hujoel, P., Schwarcz, J. & Smith, B. A. Metronidazole in periodontitis: reduced need for surgery. J. Clin. Periodontol. 19, 103–112 (1992).
Schenkein, H. A., Fletcher, H. M., Bodnar, M. & Macrina, F. L. Increased opsonization of a prtH-defective mutant of Porphyromonas gingivalis W83 is caused by reduced degradation of complement-derived opsonins. J. Immunol. 154, 5331–5337 (1995).
Lewis, J. P. & Macrina, F. L. IS195, an insertion sequence-like element associated with protease genes in Porphyromonas gingivalis. Infect. Immun. 66, 3035–3042 (1998).
Chen, T., Siddigui, H. & Olsen, I. Comparative genomics and proteomics of 13 Porphyromonas gingivalis strains. J Oral Microbiol. 7, 29008, doi:10.3402/jom.v7.29008 (2015).
Yu, F., Anaya, C. & Lewis, J. P. Outer membrane proteome of Prevotella intermedia 17: identification of thioredoxin and iron-repressible hemin uptake loci. Proteomics 7, 403–412 (2007).
Kelley, L. A., Mezulis, S., Yates, C. M., Wass, M. N. & Sternberg, M. J. The Phyre2 web portal for protein modeling, prediction and analysis. Nat. Protoc. 10, 845–858 (2015).
Pettersen, E. F. et al. UCSF Chimera—a visualization system for exploratory research and analysis. J. Comput. Chem. 25, 1605–1612 (2004).
Sievers, F. et al. Fast, scalable generation of high-quality protein multiple sequence alignments using Clustal Omega. Mol. Syst. Biol. 7, 539 (2011).
Acknowledgements
We thank Dr. Todd Kitten for providing us with Streptococcus sp. strains. This work was supported by grants R01DE023304 and R21DE023745 to J. P. Lewis. Microscopy was performed at the VCU Microscopy Facility, supported, in part, by funding from the NIH-NCI Cancer Center Support Grant P30 CA016059 with the help of Dr. Scott Henderson.
Author information
Authors and Affiliations
Contributions
J.A.H. and K.M.S. performed the experiments, prepared figures for the manuscript, and contributed to writing of the manuscript. B.R.B. performed the structural and bioinformatics analysis as well as contributed to writing of the manuscript. Q.G. performed experiments, prepared figures for the manuscript, and contributed to writing of the manuscript. J.P.L. initiated and supervised all of the work reported in this manuscript. She also revised drafts as well as wrote portions of the manuscript. P.S.H. provided the amixicile as well as helpful comments for this work, and revised the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hutcherson, J.A., Sinclair, K.M., Belvin, B.R. et al. Amixicile, a novel strategy for targeting oral anaerobic pathogens. Sci Rep 7, 10474 (2017). https://doi.org/10.1038/s41598-017-09616-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-09616-0
This article is cited by
-
MinION sequencing from sea ice cryoconites leads to de novo genome reconstruction from metagenomes
Scientific Reports (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
