
Abstract
Prior cross-sectional analyses have demonstrated an association between subclinical hypothyroidism and metabolic syndrome and selected components. However, the temporal relation between metabolic syndrome and declining thyroid function remains unclear. In a prospective study, an unselected cohort of 66,822 participants with and without metabolic syndrome were followed. A proportional hazards regression model was used to estimate hazard ratios (HRs) and 95% CIs for hypothyroidism. Exploratory analyses for the relation between components of metabolic syndrome and declining thyroid function were also undertaken. During an average follow-up of 4.2 years, the incident rates for subclinical hypothyroidism were substantially higher in participants who began the study with metabolic syndrome compared with metabolically normal controls. After controlling for risk factors, patients with metabolic syndrome were at a 21% excess risk of developing subclinical hypothyroidism (adjusted HR 1.21; 95% CI 1.03–1.42). When individual components were analyzed, an increased risk of subclinical hypothyroidism was associated with high blood pressure (1.24; 1.04–1.48) and high serum triglycerides (1.18; 1.00–1.39), with a trend of increasing risk as participants had additional more components. Individuals with metabolic syndrome are at a greater risk for developing subclinical hypothyroidism, while its mechanisms and temporal consequences of this observation remain to be determined.
Similar content being viewed by others

Introduction
Subclinical hypothyroidism, defined as elevated TSH with free T4 concentrations at the lower end of the euthyroid range, affects approximately 4–10% of the general population1, 2. Subclinical hypothyroidism has been shown to be associated with more severe coronary and carotid artery disease3,4,5,6. Furthermore, several large longitudinal studies suggest that mortality and morbidity are higher for patients with both ischemic heart disease and subclinical hypothyroidism, particularly for younger subjects7,8,9,10,11. These observations therefore suggest that subclinical hypothyroidism may be a risk factor or a predictive biomarker for cardiovascular diseases.
Although autoimmune disease is often the accepted cause of thyroid dysfunction, it is less clearer which risk factors may predispose or modify hypothyroidism. In this regard it is important to note that many12,13,14,15, but not all16, 17, cross-sectional studies observed that metabolic syndrome and its components, including high blood pressure, elevated triglycerides level, obesity, and insulin resistance, and perhaps high serum cholesterol level, are closely related to subclinical hypothyroidism. Despite these known associations, the temporal relationships between subclinical hypothyroidism and assorted cardiovascular risk factors remain largely unexplored. The aim of this study is to prospectively compare the incidence of subclinical hypothyroidism, among general population with and without metabolic syndrome. The analyses examined further the effect of individual components of the metabolic syndrome on the occurrence of subclinical hypothyroidism.
Results
The MJ Health Screening database includes a total of 94,434 participants received medical screening in Taiwan between 1996 and 2004. Among them, 9,970 participant with only one medical check-up as well as 68,743 participant with more than one visit met the inclusion criteria. After excluding individuals with only one visit, 68,743 participants were included in our analysis (Fig. 1). Supplementary Table 1 shows the baseline demographic and clinical characteristics of participants with only one visit and those with more than one visit. Compared with individuals with one medical check-up, individual with more than once were younger and had a lower percentage of diabetes, hypertension, hypertriglyceridemia, cholesterol, chronic kidney disease, proteinuria, cardiovascular disease, gout, and arthritis (Supplementary Table 1).

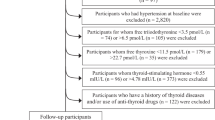
Flow chart for study participants’ enrollment.
Among them, 52.5% were women, and the mean age was 41.07 years. At the baseline, a total of 11,437 (16.6%) participants had met the criteria for metabolic syndrome and 1,151 (2%) had hypothyroidism, including 92 overt and 1,059 subclinical hypothyroidism. In the cross-sectional analysis, the following variables were significantly related to metabolic syndrome: age ≥ 40 years, male, lower educational level, smoking, drinking, and physical inactivity (Table 1). Meanwhile, hypercholesterolemia, and hyperuricemia were also positively associated with metabolic syndrome, with ORs between 2 to 3. Overt and subclinical hypothyroidism were both significantly associated with metabolic syndrome with OR 1.89 (95% CI: 1.19–2.99) and 1.48 (95% CI: 1.28–1.71) respectively.
After excluding participants with prevalent hypothyroidism at the baseline, those with missing information or errors in the records of thyroid function test and those who had ever received thyroid medicine during the follow-up period, there were 66,822 subjects included in the longitudinal analysis. During an average follow-up of 4.2 years, a total of 1,247 new cases of hypothyroidism were identified, including 51 overt and 1,196 subclinical cases. The crude incident rates of subclinical hypothyroidism, but not overt hypothyroidism, were substantially higher in participants with metabolic syndrome than those without metabolic syndrome at the baseline. The crude HR (95% CI) was 1.39 (1.21–1.60), 1.41 (1.23–1.62), and 0.98 (0.46–2.08) for total, subclinical, and overt hypothyroidism respectively (Table 2). After the adjustment of potential risk factors, participants with metabolic syndrome still had a 21% increase in the risk of subclinical hypothyroidism (adjusted HR 1.21; 95% CI 1.03–1.42).
Regarding individual component of metabolic syndrome, participants with high blood pressure, high serum triglycerides, high waist circumference, and high fasting glucose had a higher crude incidence of subclinical hypothyroidism, but not overt hypothyroidism, than those without any individual component (Table 3). In the analyses of the independent effect associated with each metabolic component, the risk of subclinical hypothyroidism significantly increased with high blood pressure (adjusted HR 1.24; 95% CI 1.04–1.48) and high serum triglycerides level (adjusted HR 1.18; 95% CI 1.00–1.39), but not the other 3 components (Table 4). The additive effect associated with different combinations of the 5 metabolic syndrome components indicated that those who had both high blood pressure and serum triglycerides had a 49% excess risk (adjusted HR 1.49; 95% CI 1.16–1.90). A trend of increasing risk was also noted when participants had additional one, two or three components apart from hypertension and elevated serum triglycerides (Table 4). However, no significantly higher risk was noted for participants with only large waist circumference, high fasting glucose, and low HDL-cholesterol level (adjusted HR 1.06; 95% CI 0.81–1.39).
For sensitivity analyses on the associations between metabolic syndrome and subclinical hypothyroidism, we excluded physical inactivity as a covariate for adjustment, additionally controlled for hypercholesterolemia at the baseline, undertook competing risk analysis by considering overt hypothyroidism and hyperthyroidism as competing risks, and excluded participants who were possibly to have treated hypothyroidism during the follow-up period, found no substantial differences (Supplement Table 2). In the stratified analyses aimed to evaluate whether risks were modified by baseline characteristics, the risks of new hypothyroidism associated with metabolic syndrome were similar for men and women, and for those aged < 40 and ≥ 40 years in the beginning of the study (Supplement Table 3).
Discussion
In this prospective cohort study, participants with metabolic syndrome were associated with a significantly increased risk of developing subclinical hypothyroidism during an average follow-up of 4 years compared to those without metabolic syndrome at the baseline. High blood pressure and high serum triglycerides may play a more important role than other metabolic syndrome components in developing subclinical hypothyroidism, although a trend of increasing risks was observed, if participants had additional components.
While prior cross-sectional studies have reported both functional and morphological changes in thyroid gland among metabolic syndrome patients18, this longitudinal study clearly demonstrates the temporal relation between these two conditions. Metabolic syndrome appears to be a risk factor for subclinical hypothyroidism. In the context of higher cardiovascular risk associated with subclinical hypothyroidism and the metabolic syndrome, the current analyses suggests that thyroid dysfunction may be one intermediate factor between metabolic syndrome and cardiovascular disease. These cross-sectional associations are clearly multifactorial including increased inflammation, pro-thrombosis, impaired fibrinolysis, endothelial dysfunction19, insulin sensitivity and endothelium-dependent vasodilation20, 21. In a retrospective study analyzing the United Kingdom General Practitioner Research Database, Razvi and colleagues found treatment of subclinical hypothyroidism with levothyroxine was associated with fewer ischemic heart disease events in the younger individuals, supporting a beneficial effect of thyroid hormone on cardiovascular risk factors in hypothyroid patients22. Whether thyroid dysfunction has a major direct effect, or is just an intermediate mediator, or simply a “bystander” in these many pathways leading to coronary atherosclerosis needs to be continuously monitored. Thus, exploring the reverse relationship between metabolic syndrome and thyroid dysfunction as well as the temporal sequence of association of metabolic syndrome, thyroid dysfunction, and cardiovascular diseases may be a worthwhile topic for future research. Furthermore, the efficacy of hypothyroidism medicine to prevent the development of metabolic syndrome should also be investigated in future studies.
Previous studies using factor analysis or structural equation modeling to understand the underlying structural of the co-occurrence of metabolic risk factors suggest that metabolic syndrome is represented primarily by “insulin resistance” and “obesity”, followed by “lipids”, and the “blood pressure”. Further, “insulin resistance/hyperinsulinemia” may be the common unifying factor that links all the core components23,24,25,26. Despite blood pressure being loosely associated with the central features of metabolic syndrome, the current analyses suggest that blood pressure was the metabolic factor that most strongly associated with the occurrence of thyroid hypofunction. This relationship may reflect the observation that hypertension is the most common (and perhaps earliest) manifestation within the myriad of at-risk phenotypes associated with atherosclerotic cardiovascular disease. Furthermore, among all the possible pathological pathways leading to hypertension27, several share a link with hypothyroidism including changes in circulating catecholamines, disturbances in the renin-angiotensin-aldosterone system, and increased peripheral vascular resistance28, 29. Although it is widely accepted that there is a close relation between hypercholesterolemia and overt hypothyroidism, our analyses suggest high serum triglycerides be a significant perhaps independent factor for increasing the risk of subclinical hypothyroidism. This effect remains unchanged even after controlling for high serum cholesterol. Evidence suggests that obesity results in fat accumulation in the thyroid gland in humans and a mouse model. This may affect the thyroid hormone production and result in hypothyroidism, as suggested by studies in obese mice30. Our study finding suggests that the association between thyroid hypofunction and high serum triglyceride level was stronger than that of high waist circumference. The connection between the metabolic syndrome components and the development of thyroid dysfunction merit further research to elaborate the underlying mechanisms.
It is well known that hypertension is often induced by excess salt intake and it is possible that people with hypertension may have excess ingestion of iodized salt. Increasing evidence suggests that a higher population iodine intake is associated with an increased level of serum TSH and more cases of hypothyroidism in the population31, 32. Excess iodine ingestion which results in thyroid dysfunction in susceptible individuals, however, is nevertheless well-tolerated in most people33. In Taiwan, the mandatory salt iodization program was implemented since 1967 but changed to voluntary salt iodization since 200334. We could not further examine whether the observed association between hypertension and hypothyroidism is caused by an excess intake of iodized salt owing to that the food frequency questionnaire does not specifically assess salt and iodine intake. Meanwhile, it is well known that thyroid hormones play an important role in lipid metabolism and there were many cross-sectional studies reporting the association between hypertriglyceridemia and hypothyroidism35. However, limited studies investigate the reverse, that is, the effect of high serum triglycerides level on thyroid gland morphology and function. In an animal study, Han and colleagues demonstrated that excess iodine combined with high-fat diet could cause damage to thyroid glands and lead to thyroid hormone disorder in mice36. In another study, Shao and colleagues found that rats fed a high-fat lard diet for 24 weeks had significantly increased serum triglyceride levels in both the serum and thyroid tissue, decreased serum total T4 and free T4 levels in parallel with elevated serum TSH levels, and altered macro and micro morphology of the thyroid gland37. In the present study, we could not further examine whether the observed association between hypertriglyceridemia and hypothyroidism is due to high fat intake. Further researches are warranted to evaluate the potential role of dietary factors that may influence the occurrence of thyroid hypofunction in the susceptible population.
The main strength of this study is that a large number of participants had been observed prospectively for several years. Participants received thyroid function tests and metabolic risk factor measurements at regular intervals such that detection bias due to differential lengths of follow-up could be minimized. Educational level and important lifestyle factors were controlled in the analysis to partition confounding effects due to these factors. Similar results following several sensitivity analyses adjusting for different risk factors or after taking competing risk into consideration suggest the current study findings are quite robust. There are also some limitations in this study. First, in this study, the follow-up duration may not be sufficiently long enough to determine the full clinical significance of subclinical thyroid dysfunction related to metabolic syndrome. Whether these cases associated with metabolic syndrome will progress to overt hypothyroidism, remain in the same status, or return to a euthyroid state needs to be examined in a longer prospective study. Second, the definition of metabolic syndrome in the present study was based on The Third Report of the National Cholesterol Education Program Expert Panel (NCEP) on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) with ethnic-specific values for waist circumference in order to be easy to compare findings with other research findings. The analyses did not examine the degree of deviation from normal or the most optimal cut-off point for individual metabolic component for the development of subsequent subclinical hypothyroidism. Third, the definition of overt and subclinical hypothyroidism was based on a single TSH and T4 value, without taking an age-adjusted TSH range into account or doubly confirmed by TSH elevation. It could probably introduce misclassification; however, this is a non-differential misclassification which biased the results toward the null. Finally, since the study population came from fee-paying participants, whether the results can be generalized to a less selected and/or less financially capable population remains to be determined.
In conclusion, our analyses suggest metabolic syndrome increases the risk of acquiring subclinical hypothyroidism, a condition routinely associated with a significantly increased risk of atherosclerotic heart disease morbidity and mortality. The mechanisms and clinical consequences of the observed relations among metabolic risk factors and thyroid hypofunction needed to be explored in the future studies.
Methods
Data source and study population
Potential participants for this prospective study came from a total of 94,434 individuals who participated in a self-paying comprehensive health examination program offered by a private firm (MJ Health Management Institute, Taiwan) between 1996 and 200438. The protocol was approved by the Research Ethics Committee in Leeds Institute of Genetics, Health and Therapeutics at the University of Leeds, Leeds, UK. All methods were performed in accordance with the relevant guidelines and regulations. The data used in this study were held and approved by MJ Health Management Institute, Taiwan. To comply with regulations related to the privacy of personal electronic data, the identity of each patient was encrypted and all data was analyzed anonymously. Hence, the IRB granted a waiver of informed consent.
Participants were excluded if 1) were not adequately followed during the study period; 2) initial or follow up test data were missing or in error; 3) questionnaires were missing; 4) reported to have received thyroid medicine at the baseline; and 5) began the study with diagnosed thyroid dysfunction. In the analysis of the association between metabolic syndrome and incident hypothyroidism, those who reported to have ever received thyroid medication during the follow-up period were excluded because thyroid hyper- or hypo-function could not be determined by questionnaire.
Data collection
In addition to a self-administered questionnaire for education level, lifestyle factors, and past medical history, each participant received a standard physical examination including anthropomorphic measurements, and blood and urine analyses. Overnight fasting blood and first morning voided urine were collected and analyzed.
Definition of metabolic syndrome and hypothyroidism
Metabolic syndrome was defined by at least 3 of the following 5 components: blood pressure ≥130/85 mm Hg (or receiving drug therapy for hypertension), serum triglycerides ≥150 mg/dL (or receiving drug therapy for hypertriglyceridemia),fasting glucose ≥100 mg/dL (or receiving drug therapy for hyperglycemia), HDL-cholesterol <40 mg/dL in men or <50 mg/dL in women, and waist circumference ≥90 cm (35 inch) in men or ≥80 cm (32 inch) in women.
Hypothyroidism was defined based on symptoms and laboratory values. Overt hypothyroidism was assumed if TSH was greater than 5 μU/ml and T4 less than 4.5 μg/dl. Subclinical hypothyroidism was defined as elevated TSH values (>5 μU/ml) but having T4 values between 4.5 and 12 μg/dl39.
Statistical analyses
Baseline characteristics for all study participants were summarized. In the cross-sectional analysis, a logistic regression model was used to estimate crude odds ratios (ORs) and 95% confidence intervals (CIs) for the risk factors potentially related to metabolic syndrome. In the subsequent cohort analysis, participants with and without metabolic syndrome were followed from the first visit to the first report of hypothyroidism, or the last visit with available blood test results. The crude incident rates for total hypothyroidism, overt, and subclinical hypothyroidism were calculated. Cox proportional hazards regression models were used to estimate hazard ratios (HRs) and 95% CIs for incident hypothyroidism with the adjustment of important risk factors, such as age, sex, cigarette smoking, alcohol consumption, physical inactivity, and low educational level. The proportional hazard assumption was examined by plotting the log minus log survival curves and survival times against cumulative survival. To further explore the independent and additive effect associated with each component, further analyses were conducted to evaluate whether the risk of hypothyroidism increased with the greater numbers of metabolic syndrome components, and which combinations of metabolic syndrome components were associated with the highest risk for hypothyroidism. Several sensitivity analyses including: 1) not controlling for physical inactivity, 2) additionally controlling for hypercholesterolemia at the baseline, 3) by competing risk analysis, and 4) excluding participants who were possibly to have treated hypothyroidism at the last follow-up visit, were performed to evaluate their influence on the results.
Stratified analyses were performed to evaluate whether baseline characteristics modified the risks. Participants were stratified according to sex (men, women) and age (<40, ≥40 years). A likelihood ratio test was conducted to evaluate the interaction between gender, age, and metabolic syndrome component for possible effect modification. Two-sided p value < 0.05 was considered to be statistically significant. All statistical analyses were performed with SAS 9.4 (SAS Institute, Cary, NC).
References
Surks, M. I. et al. Subclinical thyroid disease: scientific review and guidelines for diagnosis and management. Jama 291, 228–238, doi:10.1001/jama.291.2.228 (2004).
Biondi, B. & Cooper, D. S. The clinical significance of subclinical thyroid dysfunction. Endocrine reviews 29, 76–131, doi:10.1210/er.2006-0043 (2008).
Auer, J., Berent, R., Weber, T., Lassnig, E. & Eber, B. Thyroid function is associated with presence and severity of coronary atherosclerosis. Clinical cardiology 26, 569–573 (2003).
Dullaart, R. P., de Vries, R., Roozendaal, C., Kobold, A. C. & Sluiter, W. J. Carotid artery intima media thickness is inversely related to serum free thyroxine in euthyroid subjects. Clinical endocrinology 67, 668–673, doi:10.1111/j.1365-2265.2007.02943.x (2007).
Takamura, N. et al. Thyroid function is associated with carotid intima-media thickness in euthyroid subjects. Atherosclerosis 204, e77–81, doi:10.1016/j.atherosclerosis.2008.09.022 (2009).
Cappola, A. R. & Ladenson, P. W. Hypothyroidism and atherosclerosis. The Journal of clinical endocrinology and metabolism 88, 2438–2444, doi:10.1210/jc.2003-030398 (2003).
Walsh, J. P. et al. Subclinical thyroid dysfunction as a risk factor for cardiovascular disease. Archives of internal medicine 165, 2467–2472, doi:10.1001/archinte.165.21.2467 (2005).
Razvi, S., Weaver, J. U., Vanderpump, M. P. & Pearce, S. H. The incidence of ischemic heart disease and mortality in people with subclinical hypothyroidism: reanalysis of the Whickham Survey cohort. The Journal of clinical endocrinology and metabolism 95, 1734–1740, doi:10.1210/jc.2009-1749 (2010).
Rodondi, N. et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. Jama 304, 1365–1374, doi:10.1001/jama.2010.1361 (2010).
Tseng, F. Y. et al. Subclinical hypothyroidism is associated with increased risk for all-cause and cardiovascular mortality in adults. Journal of the American College of Cardiology 60, 730–737, doi:10.1016/j.jacc.2012.03.047 (2012).
Chaker, L. et al. Subclinical Hypothyroidism and the Risk of Stroke Events and Fatal Stroke: An Individual Participant Data Analysis. The Journal of clinical endocrinology and metabolism 100, 2181–2191, doi:10.1210/jc.2015-1438 (2015).
Knudsen, N. et al. Small differences in thyroid function may be important for body mass index and the occurrence of obesity in the population. The Journal of clinical endocrinology and metabolism 90, 4019–4024, doi:10.1210/jc.2004-2225 (2005).
Roos, A., Bakker, S. J., Links, T. P., Gans, R. O. & Wolffenbuttel, B. H. Thyroid function is associated with components of the metabolic syndrome in euthyroid subjects. The Journal of clinical endocrinology and metabolism 92, 491–496, doi:10.1210/jc.2006-1718 (2007).
Ruhla, S. et al. A high normal TSH is associated with the metabolic syndrome. Clinical endocrinology 72, 696–701, doi:10.1111/j.1365-2265.2009.03698.x (2010).
Nader, N. S. et al. Relationships between thyroid function and lipid status or insulin resistance in a pediatric population. Thyroid: official journal of the American Thyroid Association 20, 1333–1339, doi:10.1089/thy.2010.0180 (2010).
Garduno-Garcia Jde, J. et al. TSH and free thyroxine concentrations are associated with differing metabolic markers in euthyroid subjects. European journal of endocrinology/European Federation of Endocrine Societies 163, 273–278, doi:10.1530/eje-10-0312 (2010).
Mehran, L., Amouzegar, A., Tohidi, M., Moayedi, M. & Azizi, F. Serum free thyroxine concentration is associated with metabolic syndrome in euthyroid subjects. Thyroid: official journal of the American Thyroid Association 24, 1566–1574, doi:10.1089/thy.2014.0103 (2014).
Ayturk, S. et al. Metabolic syndrome and its components are associated with increased thyroid volume and nodule prevalence in a mild-to-moderate iodine-deficient area. European journal of endocrinology/European Federation of Endocrine Societies 161, 599–605, doi:10.1530/eje-09-0410 (2009).
Meigs, J. B. Invited commentary: insulin resistance syndrome? Syndrome X? Multiple metabolic syndrome? A syndrome at all? Factor analysis reveals patterns in the fabric of correlated metabolic risk factors. American journal of epidemiology 152, 908–911 discussion 912 (2000).
Fernandez-Real, J. M., Lopez-Bermejo, A., Castro, A., Casamitjana, R. & Ricart, W. Thyroid function is intrinsically linked to insulin sensitivity and endothelium-dependent vasodilation in healthy euthyroid subjects. The Journal of clinical endocrinology and metabolism 91, 3337–3343, doi:10.1210/jc.2006-0841 (2006).
Javed, A. et al. Association between thyrotropin levels and insulin sensitivity in euthyroid obese adolescents. Thyroid: official journal of the American Thyroid Association 25, 478–484, doi:10.1089/thy.2015.0005 (2015).
Razvi, S., Weaver, J. U., Butler, T. J. & Pearce, S. H. Levothyroxine treatment of subclinical hypothyroidism, fatal and nonfatal cardiovascular events, and mortality. Archives of internal medicine 172, 811–817, doi:10.1001/archinternmed.2012.1159 (2012).
Hanley, A. J. et al. Factor analysis of metabolic syndrome using directly measured insulin sensitivity: The Insulin Resistance Atherosclerosis Study. Diabetes 51, 2642–2647 (2002).
Shen, B. J. et al. Are metabolic risk factors one unified syndrome? Modeling the structure of the metabolic syndrome X. American journal of epidemiology 157, 701–711 (2003).
Pladevall, M. et al. A single factor underlies the metabolic syndrome: a confirmatory factor analysis. Diabetes care 29, 113–122 (2006).
Woolston, A., Tu, Y. K., Baxter, P. D. & Gilthorpe, M. S. A comparison of different approaches to unravel the latent structure within metabolic syndrome. PloS one 7, e34410, doi:10.1371/journal.pone.0034410 (2012).
Oparil, S., Zaman, M. A. & Calhoun, D. A. Pathogenesis of hypertension. Annals of internal medicine 139, 761–776 (2003).
Fletcher, A. K. & Weetman, A. P. Hypertension and hypothyroidism. Journal of human hypertension 12, 79–82 (1998).
Stabouli, S., Papakatsika, S. & Kotsis, V. Hypothyroidism and hypertension. Expert review of cardiovascular therapy 8, 1559–1565, doi:10.1586/erc.10.141 (2010).
Lee, M. H. et al. Thyroid Dysfunction Associated With Follicular Cell Steatosis in Obese Male Mice and Humans. Endocrinology 156, 1181–1193, doi:10.1210/en.2014-1670 (2015).
Laurberg, P. et al. Iodine intake as a determinant of thyroid disorders in populations. Best Pract. Res. Clin. Endoc. Metab. 24, 13–27, doi:10.1016/j.beem.2009.08.013 (2010).
Sun, X., Shan, Z. & Teng, W. Effects of Increased Iodine Intake on Thyroid Disorders. Endocrinology and Metabolism 29, 240–247, doi:10.3803/EnM.2014.29.3.240 (2014).
Leung, A. M. & Braverman, L. E. Consequences of excess iodine. Nat. Rev. Endocrinol. 10, 136–142, doi:10.1038/nrendo.2013.251 (2014).
Tang, K. T. et al. Iodine status of adults in Taiwan 2005-2008, 5 years after the cessation of mandatory salt iodization. J. Formos. Med. Assoc. 115, 645–651, doi:10.1016/j.jfma.2015.06.014 (2016).
Rizos, C. V., Elisaf, M. S. & Liberopoulos, E. N. Effects of Thyroid Dysfunction on Lipid Profile. The Open Cardiovascular Medicine Journal 5, 76–84, doi:10.2174/1874192401105010076 (2011).
Han, H. et al. Excess Iodine and High-Fat Diet Combination Modulates Lipid Profile, Thyroid Hormone, and Hepatic LDLr Expression Values in Mice. Biol. Trace Elem. Res. 147, 233–239, doi:10.1007/s12011-011-9300-x (2012).
Shao, S. S. et al. Dietary high-fat lard intake induces thyroid dysfunction and abnormal morphology in rats. Acta Pharmacol. Sin. 35, 1411–1420, doi:10.1038/aps.2014.82 (2014).
Wen, C. P. et al. All-cause mortality attributable to chronic kidney disease: a prospective cohort study based on 462 293 adults in Taiwan. Lancet (London, England) 371, 2173–2182, doi:10.1016/s0140-6736(08)60952-6 (2008).
Surks, M. I. et al. Subclinical thyroid disease - Scientific review and guidelines for diagnosis and management. JAMA-J. Am. Med. Assoc. 291, 228–238, doi:10.1001/jama.291.2.228 (2004).
Acknowledgements
The data used in this study were provided by the MJ Health Management Institute, Taiwan.
Author information
Authors and Affiliations
Contributions
Y.K.T. had full access to all data used in the study, takes responsibility for the integrity of the data and the accuracy of analysis, performed the data collection and revised the article critically. C.H.C. contributed substantially to the conception and design of the study, drafted the manuscript and were involved in the interpretation of data. Y.C.Y. analyzed data and were involved in the interpretation of data. J.L.C. were involved in the interpretation of data and revised the article critically. S.R.S. revised the article critically. L.M.C. revised the article critically and supervised the study.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chang, CH., Yeh, YC., Caffrey, J.L. et al. Metabolic syndrome is associated with an increased incidence of subclinical hypothyroidism – A Cohort Study. Sci Rep 7, 6754 (2017). https://doi.org/10.1038/s41598-017-07004-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-07004-2
This article is cited by
-
Body mass index as a dominant risk factor for metabolic syndrome among indonesian adults: a 6-year prospective cohort study of non-communicable diseases
BMC Nutrition (2024)
-
Association of subclinical hypothyroidism with metabolic syndrome and its components among outpatients with first-episode drug-naïve major depressive disorder: a large-scale cross-sectional study
European Archives of Psychiatry and Clinical Neuroscience (2024)
-
Cardiometabolic-related dietary patterns and thyroid function: a population-based cross-sectional study
European Journal of Medical Research (2023)
-
Prevalence and factors associated with metabolic syndrome in first hospitalization for major depression disorder patients
Scientific Reports (2023)
-
A systematic review and meta-analysis investigating the relationship between metabolic syndrome and the incidence of thyroid diseases
Endocrine (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
