
Abstract
Idiopathic olfactory disorder is resistant to treatment, and the recovery time is long. This study investigated the prognostic value of the migration of nasally administered thallium-201 to the olfactory bulb (thallium migration to the OB), a measure of olfactory nerve damage, in patients with idiopathic olfactory disorders. Twenty-four patients with idiopathic olfactory disorders were enrolled in the study (7 women and 17 men; aged 23–73 years). We retrospectively analyzed potential prognostic markers in subjects who underwent thallium-based olfactory imaging with the nasal administration of thallium-201 before conventional treatment with the Japanese herbal medicine tokishakuyakusan and compared those data with the prognosis. Log-rank tests were performed to assess the relationship between thallium migration to the OB (<4.6% [low] vs. ≥4.6% [high]; data dichotomized at the optimal cutoff value) and the duration until recovery of the odor recognition threshold determined by a standard olfactory function test (T&T olfactometry) after the treatment. Upon statistical analysis, we found that high thallium migration to the OB was significantly correlated with better prognosis in patients. Our results suggest that patients with intact olfactory nerve fibers could be selected using thallium-based imaging for the long-term follow-up of olfactory dysfunction.
Similar content being viewed by others

Introduction
The most common causes of non-sinonasal-related olfactory dysfunction are postinfectious, posttraumatic and idiopathic1. According to previous studies, the prognosis of olfactory dysfunction due to respiratory infection, head trauma, or chronic sinusitis primarily depends on residual function and, secondarily, on gender, smoking habit, age, and parosmia2. Olfactory bulb volume has been shown to be a predictor of olfactory recovery in patients with postinfectious and posttraumatic olfactory loss3. By contrast, there are currently no accepted prognostic markers that can guide the selection and treatment of patients with idiopathic olfactory dysfunction.
The radioisotope thallium-201 (201Tl) is transported within the olfactory neural tract after nasal administration in rodents4, and this transport is markedly decreased by the transection of olfactory nerve fibers in mice5. Thallium has been shown to readily substitute for potassium at the (Na+/K+)-membrane ATPase activation sites6, and nasally administered 201Tl is thought to be transported into the olfactory nerve cells as a substitute for potassium.
Nasally administered 201Tl migrates to the olfactory bulb 24 h after 201Tl administration in healthy volunteers, as assessed by a combination of single-photon emission computed tomography (SPECT), X-ray computed tomography (CT), and magnetic resonance imaging (MRI)7. The thallium-based olfactory imaging method is called “olfacto-scintigraphy.” Nasal 201Tl migration to the olfactory bulb is reduced in patients with impaired olfaction due to head trauma, upper respiratory tract infection, or chronic rhinosinusitis, which are the major causes of olfactory dysfunction, compared with 201Tl migration in healthy volunteers8. The nasal administration of 201Tl is adapted for the visual diagnosis of olfactory nerve damage in patients with olfactory disorders. Furthermore, the biological safety of nasal 201Tl administration was shown in a pre-clinical study9.
The traditional Japanese herbal medicine tokishakuyakusan rapidly promotes the expression of nerve growth factor in the olfactory bulb and rescues neurons from damage in vivo 10. The usefulness of tokishakuyakusan has been shown for the treatment of olfactory-impaired patients with Alzheimer’s-type dementia in Japan11. In this study, subjects with idiopathic olfactory dysfunction received conventional treatment via the oral intake of tokishakuyakusan (TJ-23, Tsumura, Tokyo, Japan) at the standard dose of 7.5 mg per day.
Here, we retrospectively assessed the prognostic value of nasal 201Tl migration to the olfactory bulb (a measure of olfactory nerve damage), gender, age, odor recognition threshold determined using T&T olfactometry (T&T odor recognition threshold), smoking habit, parosmia, and olfactory bulb volume in patients with idiopathic olfactory dysfunction.
Results
Univariate analysis of prognostic factors in patients
To determine whether nasal 201Tl migration to the olfactory bulb can be used to predict the outcome of treatment in patients with olfactory disorder, we retrospectively compared the duration until recovery between patients with high (≥4.6%) nasal 201Tl migration to the olfactory bulb and those with low (<4.6%) nasal 201Tl migration to the olfactory bulb based on medical chart review. The data of nasal 201Tl migration to the olfactory bulb were dichotomized at the optimal cutoff value as shown in the methods.
In univariate analysis, the duration until recovery was significantly shorter in patients with high nasal 201Tl migration to the olfactory bulb than in those with low nasal 201Tl migration to the olfactory bulb (Table 1; P = 0.0003, N = 24). The recovery rate was 67% in patients with high nasal 201Tl migration to the olfactory bulb one year after treatment. By contrast, none of the patients with low nasal 201Tl migration to the olfactory bulb showed recovery at one year after treatment. The improvement in the T&T odor recognition threshold was judged according to the criteria of the Japanese Rhinologic Society12 (cure, T&T odor recognition threshold ≤2.0; remission, decrease in T&T odor recognition threshold ≥1.0; progress, increase in T&T odor recognition threshold of ≥1.0; stable, all other cases). Cure or remission was defined as “recovery.”
To assess whether differences in the T&T odor recognition thresholds were significant in the treatment of the subjects, we compared T&T odor recognition thresholds between pre-treatment and post-treatment with Mann–Whitney tests. T&T odor recognition thresholds were significantly reduced after treatment in the patients with a high Tl-201 olfactory transport rate (Fig. 1A, N = 9, P = 0.0007). By contrast, T&T odor recognition thresholds were not significantly different after treatment in the patients with a low Tl-201 olfactory transport rate (Fig. 1B, N = 15, P = 0.470). The observation time was not significantly different between patients with a high Tl-201 olfactory transport rate and those with a low Tl-201 olfactory transport rate (P = 0.152; high Tl-201 olfactory transport rate group, 8.1 ± 7.6 months [mean ± SD]; low Tl-201 olfactory transport rate group, 13.4 ± 13.8 months [mean ± SD]) (Mann–Whitney tests were used to compare the two groups).

Differences in the odor recognition thresholds determined by T&T olfactometry (T&T odor recognition threshold) following conventional treatment with the Japanese herbal medicine tokishakuyakusan. Smaller numbers of odor recognition thresholds indicate higher sensitivities to odors. (A) Patients with high nasal 201Tl migration to the olfactory bulb (N = 9). (B) Patients with low nasal 201Tl migration to the olfactory bulb (N = 15). Bars indicate mean.
None of the other potential prognostic factors tested (gender, age, T&T odor recognition threshold, smoking habit, parosmia, or olfactory bulb volume) was significantly correlated with prognosis in the patients with olfactory dysfunction (Table 1).
Correlation between nasal 201Tl migration to the olfactory bulb and change in the T&T odor recognition threshold after treatment
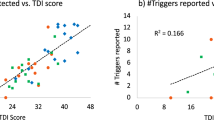
Nasal 201Tl migration to the olfactory bulb was significantly correlated with a change in the T&T odor recognition threshold after treatment (Fig. 2, Spearman r = −0.637, P = 0.0008).

The correlation between the initial nasal 201Tl migration to the olfactory bulb before treatment and the change in the T&T odor recognition threshold after treatment. The nasal 201Tl migration to the olfactory bulb was significantly correlated with the change in the T&T odor recognition threshold following treatment (Spearman r = −0.637, P = 0.0008).
Correlation between nasal 201Tl migration to the olfactory bulb and other prognostic factors
Nasal 201Tl migration to the olfactory bulb was not significantly correlated with T&T odor recognition thresholds (Spearman r = −0.374, P = 0.072), age (Spearman r = 0.392, P = 0.058) or olfactory bulb volume (Spearman r = 0.205, P = 0.337). Nasal 201Tl migration to the olfactory bulb was not significantly different between patient groups dichotomized by gender (P = 0.341), parosmia (P = 0.271), or smoking habit (P = 0.611) (Mann–Whitney tests were used to compare two groups).
Representative cases
Below, we describe two representative cases of patients with idiopathic olfactory dysfunction. The case with the better prognosis was a 49-year-old female who had relatively high nasal 201Tl migration to the olfactory bulb (11.1%; Fig. 3A). The T&T odor recognition threshold decreased from 4.2 to 0.8 after treatment with the tokishakuyakusan for a month. The case with the worse prognosis was a 40-year-old male who had low nasal 201Tl migration to the olfactory bulb (3.3%; Fig. 3B). The T&T odor recognition threshold increased from 5.0 to 5.8 after treatment with the tokishakuyakusan for 16 months.

Single photon emission computed tomography (SPECT), X-ray computed tomography (CT), and magnetic resonance imaging (MRI) Olfacto-scintigraphy in representative cases with idiopathic olfactory dysfunction. (A) A case of better prognosis was a 49-year-old female who had relatively high nasal 201Tl migration to the olfactory bulb (11.1%). (B) A case of worse prognosis was a 40-year-old male who had low nasal 201Tl migration to the olfactory bulb (3.3%).
Multivariable analysis of nasal 201Tl migration to the olfactory bulb, gender and age in patients
As olfaction may be correlated with gender and age, we conducted a multivariable analysis to determine whether nasal 201Tl migration to the olfactory bulb was the independent significant prognostic marker in the patients. Nasal 201Tl migration to the olfactory bulb was the significant independent predictors of prognosis in the patients with idiopathic olfactory dysfunction (Table 2). None of gender or age was significantly correlated with prognosis in the subjects (Table 2).
Discussion
In this study, we showed that nasal 201Tl migration to the olfactory bulb determined before the conventional treatment with the Japanese herbal medicine tokishakuyakusan was a useful predictor of prognosis in idiopathic olfactory-impaired patients. Nasal 201Tl migration to the olfactory bulb has been shown to be significantly decreased by the transection of olfactory nerve fibers in vivo 5. Our results support the prognostic value of nasal 201Tl migration to the olfactory bulb, suggesting that patients with intact olfactory nerve fibers could be selected using thallium-based imaging for the long-term follow-up of olfactory dysfunction.
Intravenous injection of thiamine propyldisulfide (Alinamin) induces the sensation of a garlic-like odor, and Alinamin injection is widely used as one of the subjective olfactory tests in Japan13. Nonresponders in the Alinamin test have been previously shown to have poor prognosis in the recovery of olfactory acuity14. The Alinamin test is simple but often results in vascular pain; the Alinamin test was not assessed here because five patients refused to undertake the test because of the associated pain.
The olfactory bulb volume has been shown to be a predictor of olfactory recovery in patients with postinfectious and posttraumatic olfactory loss3. In the present study, the olfactory bulb volume was not significantly correlated with the duration until recovery of olfactory recognition, although the data for olfactory bulb volume were dichotomized according to a previous study (<40 mm3 vs. ≥40 mm3)3. The reason for this discrepancy may be that the subjects in this study, but not those in the previous study, suffered from idiopathic olfactory disorder.
To evaluate olfactory nerve connectivity in patients with impaired olfaction, assessing the migration of nasally administered 201Tl to the olfactory bulb is a useful and safe method. None of the subjects examined here experienced major side effects following the nasal administration of 201Tl, perhaps due to the small dose of administered 201Tl. The absorbed doses of 201Tl were estimated as 0.59 mGy in the lens and 0.067 mGy in the brain after the nasal administration of 22 MBq 201Tl by applying the MIRD formula7, 15. Thus far, no serious side effects have been reported in subjects after olfacto-scintigraphy. Furthermore, because the facial bone surrounds the nasal turbinates, acute radiation effects to the neighboring organs, such as the lens and brain, may be tolerable.
Because olfacto-scintigraphy takes 24 h to assess 201Tl migration to the olfactory bulb, patients have to return to the hospital for SPECT-CT analysis 24 h after 201Tl administration. Therefore, for clinical applications, there is a need for an olfactory nerve tracer that can rapidly enter the central nervous system. Iodine-125-conjugated human recombinant insulin-like growth factor-1 (125I-hIGF-1) uptake can be detected in the mouse cerebrum 30 min after nasal administration16. Furthermore, unilateral olfactory bulb resection prevents nasally administered hIGF-1 from increasing the phosphorylation of extracellular signal-regulated kinase 1/2 in the mouse cerebrum in vivo 16. These findings suggest that olfactory bulb damage reduces the nasal transport of hIGF-1 to the brain in vivo. Although 125I-hIGF-1 is commercially available, its half-life (60.1 days) is too long for clinical applications. Furthermore, the low energy of Iodine-125 is not appropriate for SPECT imaging. Thus, the development of a new isotope-conjugated hIGF-1 for nasal administration warrants further investigation.
In this study, patients with idiopathic olfactory dysfunction received conventional treatment through the oral intake of the Japanese herbal medicine tokishakuyakusan. In contrast, the effect of olfactory training using four intense odors (rose, eucalyptus, lemon and cloves) has been reported in the treatment of patients with olfactory loss in Germany17. Olfactory training is not a conventional treatment for patients with olfactory loss in Japan because it is not clear which odors are useful for the olfactory training of Japanese patients. Thus, further investigation is required to determine whether nasal 201Tl migration to the olfactory bulb may serve as a predictor of prognosis following the olfactory training of patients with olfactory disorders.
In conclusion, the duration until recovery of odor recognition was significantly shorter in patients with idiopathic olfactory dysfunction with high nasal 201Tl migration to the olfactory bulb than in those with low nasal 201Tl migration to the olfactory bulb in this retrospective study. Our results suggest that severe olfactory nerve damage determined using thallium-based olfactory imaging predicts a worse prognosis in patients with idiopathic olfactory loss. None of the other potential prognostic factors tested (gender, age, T&T odor recognition threshold, smoking habit, parosmia, or olfactory bulb volume) was significantly correlated with prognosis in the subjects. Our thallium-based imaging “Olfacto-scintigraphy” is useful for avoiding the ineffective treatment in the patients, although the subjects need to return to hospital 24 h after nasal administration of 201Tl. To assess whether nasal 201Tl migration to the olfactory bulb is a general predictor of prognosis in patients with olfactory disorders, this study needs to be extended to a larger cohort across multiple institutes following the olfactory training of patients with olfactory impairment.
Materials and Methods
Subjects
Twenty-four subjects with idiopathic olfactory disorders were randomly selected from among patients who received follow-up visits at the smell clinic at the Kanazawa Medical University Hospital (2009–2016) and who underwent thallium-based olfactory imaging (olfacto-scintigraphy) (7 women and 17 men; aged 23–71 years). Subjects were excluded if they had a history of chronic rhinosinusitis, head injury, acute respiratory infection in the three months prior to the onset of olfactory dysfunction, congenital olfactory loss, or neurodegenerative disorder. The Medical Ethics Committees of Kanazawa Medical University and Kanazawa University approved this study in advance (trial registration number: UMIN000023519). All subjects were informed of the objectives of the study and possible side effects (e.g., allergic reactions to 201TlCl and irritation of the digestive system) and gave written informed consent. Subjects were excluded if they were pregnant or lactating or had a history of kidney disease, liver injury, or other serious illness.
The characteristics of the patients are as follows (T&T odor recognition threshold, 4.8 ± 1.0 [mean ± SD]; Smoking habit, 7 smokers/ex-smokers and 17 non-smokers; Parosmia, 6 patients with parosmia and 18 patients without parosmia).
In this study, the subjects with olfactory dysfunction were observed the day after olfacto-scintigraphy until the “recovery” of olfactory recognition or the end of the observation time. The patients with idiopathic olfactory dysfunction received conventional treatment via the oral intake of tokishakuyakusan (TJ-23, Tsumura, Tokyo, Japan) at the standard dose of 7.5 mg per day at our institute.
The duration until the “recovery” of olfactory recognition or the end of the observation time ranged from 1 to 60 months (11 ± 12 months [mean ± SD]: see definition of “recovery” as follows). The improvement in the T&T odor recognition threshold was judged according to the criteria of the Japanese Rhinologic Society12 (cure, T&T odor recognition threshold ≤2.0; remission, decrease in T&T odor recognition threshold ≥1.0; progress, increase in T&T odor recognition threshold of ≥1.0; stable, all other cases). Cure or remission was defined as “recovery”12.
T&T olfactometry
In Japan, T&T olfactometry (Daiichi Yakuhin Sangyo, Tokyo, Japan) is a standard means of measuring olfactory thresholds; the normal odor recognition threshold score of each nostril is 2.0 or less. The olfactory severities were categorized according to the mean T&T recognition thresholds, and patients were diagnosed as anosmia when the T&T recognition thresholds were 5.6 or greater12.
Each odorant was dissolved in mineral oil to form a graded series of concentrations and then was applied liberally to blotting paper, followed by presentation to patients using T&T olfactometry. The odor recognition threshold was measured on the nasal side of 201Tl administration. The T&T odor recognition thresholds in the subjects ranged from 2.6 to 5.8 (4.8 ± 1.0 [mean ± SD]).
Olfacto-scintigraphy and analysis of olfactory bulb volume
For each subject, 0.3 ml of 201TlCl (22 MBq) was administered unilaterally to the olfactory cleft, and SPECT-CT was conducted 24 h later. The data acquisition was performed using a dual-headed SPECT-CT hybrid system (Symbia T6; SIEMENS Healthcare Japan, Tokyo, Japan) equipped with low-energy high-resolution collimators. The data were acquired over 360°, with 90 projections (30 s per projection), 128 × 128 matrix (with 2.29 times zoom, pixel size 2.1 mm), and a 72-KeV photopeak with a 30% main window and 7% subwindow on both sides. Data reconstruction was performed with 3D OSEM (nine subsets and eight iterations), including attenuation and scatter correction (Flash 3D, SIEMENS).
Olfactory clefts were open in all patients. Separate MRI images were merged with the SPECT-CT images. Experienced radiologists (NW and HT) who were blind to the olfactory test data separately determined the volume of the olfactory bulb by manual segmentation of 3.0 Tesla MRI coronal slices (2-mm thick, T2 weighted image) of the olfactory bulb on the nasal side of 201Tl administration. The change in the diameter at the beginning of the olfactory tract was used as the proximal demarcation of the olfactory bulb. The averages of the two radiologists’ scores were used for the statistical analysis.
The index of 201Tl migration from the olfactory epithelium to the olfactory bulb was determined as the ratio of the total 201Tl count in the olfactory bulb region of interest to the total 201Tl count in the nasal turbinate region of interest, expressed as a mean percentage of the values calculated from both sagittal and coronal images. Experienced nuclear radiologists (JT, KO, and SK) who were blind to the olfactory test data determined two separate regions of interest for the nasal turbinate area and the anterior skull base (olfactory bulb area) on the 201Tl SPECT–MRI fusion image. On 3 sequential fused images in both sagittal and coronal planes, large regions of interest were tentatively set manually on the nasal turbinate area to cover all of the residual 201Tl activity in the nasal cavity, and the nasal cavity region of interest was defined as the area bounded by the 50% threshold of the peak 201Tl count. Next, the oval regions of interest were set manually to delineate the olfactory bulb on the side of the nasal administration of the tracer by referencing the MRI T2-weighted images.
Definition of recovery and analysis of prognostic factors
We assessed whether the duration until recovery correlated with prognostic factors, including nasal 201Tl migration to the olfactory bulb (<4.6% [low] vs. ≥4.6% [high]; data dichotomized at the optimal cutoff value [Table 3]), gender (male vs. female), age (≥60 years. vs. <60 years), T&T odor recognition thresholds (≥5.6 [anosmia] vs. <5.6 [dysosmia]), smoking habit (smokers and ex-smokers vs. non-smokers), parosmia (present vs. absent) and olfactory bulb volume (<40 mm3 vs. ≥40 mm3; data dichotomized according to the previous study3). We did not assess whether disease duration correlated with the prognosis of the patients because some patients did not clearly remember when they started to have olfactory dysfunction.
Statistical analysis
For statistical analysis, log-rank tests, two-tailed Spearman correlations, and Mann–Whitney tests were performed using Prism 5 software (GraphPad, San Diego, CA, USA). Multivariable statistical models were generated using a proportional hazards regression approach (JMP 13 software, Cary, NC, USA). The sensitivities and specificities in the receiver operating characteristic (ROC) table were also calculated using JMP 13 software (Cary, NC, USA). P values less than 0.05 were considered significant.
Compliance with ethical standards
All of the procedures performed in this study involving subjects were in accordance with the ethical standards of the institutional committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all of the individual participants included in the study. This article does not contain any studies with animals performed by any of the authors.
References
Fonteyn, S. et al. Non-sinonasal-related olfactory dysfunction: A cohort of 496 patients. Eur. Arch. Otorhinolaryngol. Head and Neck dis. 131, 87–91 (2014).
Hummel, T. & Lötsch, J. Prognostic factors of olfactory dysfunction. Arch. Otolaryngol. Head Neck Surg. 136, 347–351 (2010).
Rombaux, P., Huart, C., Deggouj, N., Duprez, T. & Hummel, T. Prognostic value of olfactory bulb volume measurement for recovery in postinfectious and posttraumatic olfactory loss. Otolaryngol. Head Neck Surg. 147, 1136–1141 (2012).
Kanayama, Y., Enomoto, S., Irie, T. & Amano, R. Axonal transport of rubidium and thallium in the olfactory nerve of mice. Nucl. Med. Biol. 32, 505–512 (2005).
Kinoshita, Y. et al. Thallium transport and the evaluation of olfactory nerve connectivity between the nasal cavity and olfactory bulb. Chem. Senses. 33, 73–78 (2008).
Ando, A. et al. Biodistributions of radioactive alkaline metals in tumor bearing animals: comparison with 201Tl. Eur. J. Nucl. Med. 14, 352–357 (1988).
Shiga, H. et al. Evaluation of the olfactory nerve transport function by SPECT-MRI fusion image with nasal thallium-201 administration. Mol. Imaging Biol. 13, 1262–1266 (2011).
Shiga, H. et al. Assessment of olfactory nerve by SPECT-MRI image with nasal thallium-201 administration in patients with olfactory impairments in comparison to healthy volunteers. PLOS ONE. 8, e57671, doi:10.1371/journal.pone.0057671 (2013).
Washiyama, K. et al. Biological safety of nasal thallium-201 administration: a preclinical study for olfacto-scintigraphy. J. Rad. Res. (Tokyo) 52, 450–455 (2011).
Song, Q. H., Toriizuka, K., Jin, G. B., Yabe, T. & Cyong, J. C. Long term effects of Toki-shakuyaku-san on brain dopamine and nerve growth factor in olfactory-bulb-lesioned mice. Jpn. J. Pharmacol. 86, 183–188 (2001).
Shimada, K., Ogino, H. & Takemoto, I. Effect of Toki-Shakuyaku-San on central olfactory disturbances. Jpn. J. Taste Smell Res. 4, 339–340 (1997). (in Japanese).
Oka, H. et al. Olfactory changes after endoscopic sinus surgery in patients with chronic rhinosinusitis. Auris Nasus Larynx. 40, 452–457 (2013).
Takakura, H. et al. Cortical hemodynamic responses to intravenous thiamine propyldisulphide administration detected by multichannel near infrared spectroscopy (NIRS) system. Brain Topogr. 24, 114–126 (2011).
Furukawa, M., Kamide, M., Miwa, T. & Umeda, R. Significance of intravenous olfaction test using thiamine propyldisulfide (Alinamin) in olfactometry. Auris Nasus Larynx. 15, 25–31 (1988).
Shiga, H. et al. Reduced nasal transport of insulin-like growth factor-1 to the mouse cerebrum with olfactory bulb resection. Chem. Senses. 39, 595–599 (2014).
Kinase, S. et al. Internal dosimetry for nasal thallium-201 administration. KEK Proceedings. 7, 35–40 (2012).
Hummel, T. et al. Effects of olfactory training in patients with olfactory loss. Laryngoscope. 119, 496–499 (2009).
Acknowledgements
This study was funded, in part, by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science & Technology of Japan (C25462670 and C17K11369 to HS). We are grateful to Dr. Kinase for the internal dose calculation and to Dr. Washiyama, Dr. Amano, and Dr. Furukawa for their helpful suggestions. We also thank Prof. Hummel and Prof. Kikuchi for their expert comments. We are supported by the help of the technical staff in the Division of Radioisotopes in Kanazawa University Hospital and in the Division of Radiology in Kanazawa Medical University Hospital.
Author information
Authors and Affiliations
Contributions
All authors had full access to all of the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. H.S., J.T., and T.M. created the study concept and design and directed the patient acquisitions. H.S., J.T., and K.O. participated in the drafting and editing of the manuscript. H.S. and H.N. performed statistical analysis. J.T., K.O., S.K., N.W., and H.T. contributed to the imaging analysis. All of the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shiga, H., Taki, J., Okuda, K. et al. Prognostic value of olfactory nerve damage measured with thallium-based olfactory imaging in patients with idiopathic olfactory dysfunction. Sci Rep 7, 3581 (2017). https://doi.org/10.1038/s41598-017-03894-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-03894-4
This article is cited by
-
Thallium-201 Imaging in Intact Olfactory Sensory Neurons with Reduced Pre-Synaptic Inhibition In Vivo
Molecular Neurobiology (2020)
-
Usefulness of our proposed olfactory scoring system during endoscopic sinus surgery in patients with chronic rhinosinusitis
European Archives of Oto-Rhino-Laryngology (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
