
Abstract
The aim of this study was to investigate the real-world effectiveness of antidepressant use in persons with schizophrenia. The register-based study cohort included all 61,889 persons treated in inpatient care due to schizophrenia during 1972–2014 in Finland. The main outcome was hospitalization due to psychosis and secondary outcomes included non-psychiatric hospitalization and all-cause mortality. We used within-individual design to compare the risk of hospitalization-based outcomes during the time periods of antidepressant use to antidepressant non-use periods within the same person, and traditional between-individual Cox models for mortality. The risk of psychosis hospitalization was lower during antidepressant use as compared to non-use (adjusted Hazard Ratio, aHR, 0.93, 95% CI 0.92–0.95). Antidepressants were associated with a decreased risk of mortality (aHR 0.80, 95% CI 0.76–0.85) and a slightly increased risk of non-psychiatric hospitalization (aHR 1.03, 95% CI 1.01–1.06). In conclusion, these results indicate that antidepressants might be useful and relatively safe to use in this population.
Similar content being viewed by others


Introduction
Depression is common among persons with schizophrenia, reaching a prevalence of 33% according to a recent meta-analysis1. Lack of treatment or treatment response to depression may result in serious consequences among persons with schizophrenia, including alcohol misuse and more frequent paranoid delusions2. Consequently, antidepressants are widely used in persons with schizophrenia to treat a variety of symptoms, such as negative and depressive symptoms. In earlier studies, the prevalence of antidepressant use in schizophrenia has been evaluated to be from 15% to 58%, however, there are differences between regions and how prevalence was measured3,4,5,6,7,8,9,10,11. Our previous study, which evaluated antidepressant use in patients with first-episode schizophrenia found that 35.4% initiated antidepressant use within 3 years after schizophrenia diagnosis3.
Only a few studies have assessed the effectiveness of antidepressant use in persons with schizophrenia in real-world settings. A previous U.S. study evaluated several outcomes related to the effectiveness and safety aspects of antidepressant augmentation12, and two previous studies have assessed the association between antidepressant use and mortality in schizophrenia in Nordic countries9,13, and one study in Taiwan10. To our knowledge, there are no previous studies investigating the effectiveness of specific antidepressants in real-world settings. The efficacy of antidepressant use in persons with schizophrenia has been investigated in several randomized controlled trials (RCTs) and meta-analyses based on these RCTs. Cochrane reviews conclude that antidepressants may be useful in improving negative symptoms14, but there is not enough evidence to support the treatment of depressive symptoms with antidepressants in schizophrenia15. Regarding add-on antidepressant treatment Helfer et al. included 82 studies with 3608 persons in their meta-analysis and concluded that add-on antidepressant treatment may have a small beneficial effect on negative and depressive symptoms and seem relatively safe to use16. Similar conclusions on antidepressant augmentation were derived in a meta-analysis by Galling et al. They concluded, based on 42 studies with a total of 1934 persons, that antidepressant augmentation to antipsychotics may be effective in reducing total and negative symptoms, although the finding on total symptoms may be driven by a reduction in negative symptoms17. These meta-analyses also noted several limitations, such as a small number of double-blinded trials, reporting bias, small study sample sizes, and confounding by secondary negative symptoms.
According to the Finnish Current Care Guideline18, antidepressants may be useful to treat negative and depressive symptoms in persons with schizophrenia. Different care guidelines seem to be relatively cautious19,20,21 with their guidance concerning the use of antidepressants in persons with schizophrenia, or state that their use is beyond the scope of the guideline22. Some even refrained from making recommendations due to the low quality of available evidence23. However, the Scottish guideline for the management of schizophrenia proposes that antidepressants may be trialed for persistent negative symptoms and depressive symptoms24.
The objectives of this study were to investigate the real-world effectiveness of antidepressant use in persons with schizophrenia, with psychosis hospitalization as the main outcome, and risk of hospitalization due to non-psychiatric and cardiovascular reasons, and all-cause mortality as secondary outcomes.
Methods
Study population
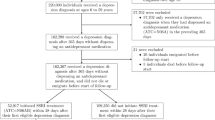
This cohort study included all persons treated in inpatient care due to schizophrenia in Finland (N = 61,889) during 1972–2014. Schizophrenia was defined as having an International Classification of Diseases (ICD) version 10 diagnosis of schizophrenia (F20) or schizoaffective disorder (F25) recorded in inpatient care. The data regarding diagnoses (including dates of admissions and discharges with discharge diagnoses) were obtained from the Hospital Discharge Register maintained by the National Institute for Health and Welfare. Prescription Register maintained by the Social Insurance Institution was utilized to obtain drug use information. Prescription Register data included ATC code, dispensing dates, purchased amount, and drug formulation (strength, package size, drug form). Data concerning dates of death and recorded causes of death were obtained from the National Death Register maintained by Statistics Finland. Data in the Prescription Register is available since 1995 and thus, follow-up for drug use in this study started at the beginning of 1996. Persons entered the cohort and the follow-up started at January 1996, or after the first diagnosis of schizophrenia for those diagnosed between 1996 and 2014. The follow-up ended either December 31, 2017 (end of data linkage) or at death.
Exposure
The exposure of this study was the use of antidepressants (N06A), which were also categorized by mechanism of action (non-selective monoamine reuptake inhibitors (TCAs, N06AA), selective serotonin reuptake inhibitors (SSRIs, N06AB) and serotonin-norepinephrine reuptake inhibitors (SNRIs, including venlafaxine, milnacipran, and duloxetine). For the analyses of specific drug substances, nine most used antidepressants and antidepressant polytherapy (defined as time periods when two or more antidepressants were used concomitantly) were included. PRE2DUP (From Prescriptions to Drug Use Periods) method was utilized to model the data from drug dispensings to drug use periods. PRE2DUP estimates drug use periods on sliding averages of daily doses, purchased amount, and drug package-specific parameters, which control the joining of purchases. PRE2DUP also considers possible inpatient care, stockpiling of drugs, and dosage changes. PRE2DUP has been described in detail previously25 and the validity of the method has been shown to be good for antidepressants26. As register data do not include drugs used during inpatient stays time in hospital care is removed from all analyses (i.e. inpatient time is not categorized as “use” nor “non-use”).
Outcomes
Main outcome was hospitalization due to psychosis (ICD-10: F20–F29). Secondary outcomes were non-psychiatric hospitalization (diagnoses other than F00–F99), hospitalization due to cardiovascular reasons (I00–I99), and all-cause mortality. Deaths recorded during the outpatient time were included, in addition to those happening during the first 2 days after admission to hospital care.
Statistical analysis
Within-individual design was utilized to minimize selection bias in the analyses of hospital-based outcomes. In this design, each person acts as his/her own control, and only time-varying covariates were adjusted for, as the impact of all time-invariant factors is eliminated by the design. Time-varying covariates included were sequential order of treatments, time since cohort entry and use of antipsychotics (ATC N05A excl. lithium), mood stabilizers: carbamazepine (N03AF01), lamotrigine (N03AX09), lithium (N05AN01) and valproic acid (N03AG01), benzodiazepines (N05BA, N05CD) and Z-drugs (N05CF). Details of the covariates are presented in Supplementary Table 1. We used stratified Cox regression to calculate adjusted hazard ratios (aHR) with 95% confidence intervals (CI).
Mortality was investigated in the traditional between-individual Cox model with time-varying exposure and covariates. One-time events such as death cannot be analyzed in within-individual design and between-individual analysis was also conducted as a sensitivity analysis for the main outcome. Between-model was adjusted for the same covariates as within-individual analyses and additionally for age, sex, number of previous hospitalizations due to psychoses, asthma/chronic obstructive pulmonary disease, cardiovascular disease, cancer, diabetes, substance use disorder, previous suicidal behavior, type of schizophrenia-spectrum disorder (schizoaffective vs. schizophrenia), liver diseases, renal diseases, and medication use, including antiepileptics, statins, antidiabetics, anti-parkinson drugs and prior use of long-acting injectable antipsychotics, or clozapine. Covariates included in between-individual model are described in Supplementary Table 1.
Stratified analyses by sex were conducted for the main outcome. We also performed a sensitivity analysis for the main outcome by omitting the first 30 days of each exposure from analyses, since the effectiveness of antidepressant medications is rarely immediate. Data management and analyses were conducted with SAS 9.4.
Permissions for this study were granted by pertinent institutional authorities at the Finnish National Institute for Health and Welfare, The Social Insurance Institution of Finland, and Statistics Finland.
Results
Altogether 61,889 persons were included in the study, and 50.3% were men (N = 31,104). The mean age at cohort entry was 46.2 [standard deviation, SD 16.0]. Characteristics of antidepressant users (49.3% of the cohort, N = 30,508) are described in Table 1. Number of events, number of users, and person-years per exposure are presented in Table 2. Most commonly used antidepressants were citalopram (used by 21.0% of the cohort), mirtazapine (12.6%), sertraline (8.3%), followed by fluoxetine (7.3%), and escitalopram (6.8%).
During the follow-up (median 14.8 years, IQR 7.5–22.0), 36,923 (59.7%) persons were rehospitalized due to psychosis at least once. Antidepressant use was associated with a lower risk of psychosis hospitalization compared to non-use (aHR 0.93, 95% CI 0.92–0.95). Similar lower risks were observed within antidepressant groups SSRIs (aHR 0.91, 95% CI 0.89–0.93), SNRIs (aHR 0.92, 95% CI 0.88–0.97), and TCAs (aHR 0.93, 95% CI 0.89–0.98). Of the individual drug substances, use of sertraline (aHR 0.87, 95% CI 0.83–0.91), fluoxetine (0.88, 0.83–0.92), citalopram (0.92, 0.90–0.95), venlafaxine (0.93, 0.88–0.97) and escitalopram (0.93, 0.88–0.99) and other antidepressants (0.95, 0.91–0.996) was associated with lower risk of psychosis hospitalization (Fig. 1).

Adjusted hazard ratios (aHRs) with 95% Confidence Intervals (CIs). Polytherapy refers to the concomitant use of two or more antidepressants. Other ADs include the rest of the antidepressants marketed in Finland.
In sensitivity analyses, we observed similar results as in the main analysis when comparing men and women (Supplementary Fig. 1). We also performed an analysis of the main outcome when the first 30 days were omitted from all use and non-use periods, and the results were similar as in the main analysis (Supplementary Fig. 2). In a between-individual analysis of the main outcome, the results were generally similar, except for antidepressant polytherapy, which was associated with an increased risk of psychosis hospitalization (aHR 1.09, 95% CI 1.02–1.17) (Supplementary Fig. 3).
During the follow-up, 43,609 (70.5%) persons were hospitalized due to non-psychiatric reasons at least once, with 12,696 (20.5%) persons being hospitalized due to cardiovascular reasons. We found an increased risk of non-psychiatric hospitalization associated with antidepressant use compared to non-use (aHR 1.03, 95% CI 1.01–1.06). Considering individual drugs, this increased risk was observed with citalopram (aHR 1.05, 95% CI 1.02–1.09), escitalopram (aHR 1.08, 95% CI 1.01–1.16), and polytherapy (aHR 1.08, 95% CI 1.03–1.13) (Fig. 2A). We found no association with risk of hospitalization due to cardiovascular reasons during any use (aHR 0.95, 95% CI 0.87–1.03) compared to non-use of antidepressants (Fig. 2B).

Hospitalization due to A non-psychiatric reasons and B cardiovascular reasons. Adjusted hazard ratios (aHRs) with 95% Confidence Intervals (CIs). Polytherapy refers to the concomitant use of two or more antidepressants. Other ADs include the rest of the antidepressants marketed in Finland.
Altogether 14,813 persons died during the follow-up. The risk of all-cause mortality was lower with antidepressant use compared to non-use (aHR 0.80, 95% CI 0.76–0.85). This lower risk was observed with sertraline (aHR 0.67, 95% CI 0.56–0.80), escitalopram (0.71, 0.59–0.86), amitriptyline (0.73, 0.59–0.91), mianserin (0.76, 0.60–0.95), citalopram (0.76, 0.69–0.83) and other antidepressants (0.80, 0.70–0.91) compared with non-use of antidepressants (Fig. 3).

Adjusted hazard ratios (aHRs) with 95% Confidence Intervals (CIs). Polytherapy refers to the concomitant use of two or more antidepressants. Other ADs include the rest of the antidepressants marketed in Finland.
Discussion
In this study, we found that antidepressant use was associated with about 10% decreased risk of hospitalization due to psychosis and 20% decreased risk of all-cause mortality. None of the studied drugs were related to an increased risk of psychosis or mortality. However, we found that the use of antidepressants was associated with a slightly increased risk of hospitalization due to non-psychiatric reasons.
We found an association between a lower risk of psychosis hospitalization with antidepressant use in general and with certain antidepressants. This is in line with the findings of Stroup et al. who found a lower risk of hospital admission due to psychiatric reasons for antidepressant initiators (aHR 0.84, 95% CI 0.80–0.88)12. However, they investigated add-on antidepressant use comparing it with the initiation of another antipsychotic as a reference, and included hospitalization due to any mental disorder for this outcome. These differences make direct comparisons between the studies difficult. Stroup and colleagues did not assess specific antidepressants for this outcome. Our study showed a lower risk of psychosis hospitalization associated with sertraline, fluoxetine, citalopram, venlafaxine, and escitalopram. We did not observe a lower risk associated with mirtazapine and mianserin use. One reason for this might be that they are widely used for insomnia in Finland, and usually, the dosage with this indication is relatively small compared to other indications, especially with mirtazapine27. We found an association with antidepressant polytherapy, referring to the concomitant use of two or more antidepressants, and increased risk of psychosis hospitalization in between-individual analysis. More severely ill patients are often treated with several medications, which might explain this finding.
We found a 20% lower risk of mortality associated with antidepressant use. Similar findings considering antidepressant use have been found in a previous study comparing different levels of antidepressant exposure with non-use (15–40% lower risk depending on the level of exposure)9. Another study comparing the levels of antidepressant exposure found 17% lower risk associated with low exposure and 9% lower risk with moderate exposure, but there was no difference in risk with the highest exposure10. Similar trend was also seen in a previous Finnish study, even though the results were not statistically significant (HR 0.57, 95% CI, 0.28–1.16)13. However, the study cohort was considerably smaller (N = 2588) than in our study. Stroup and colleagues also evaluated mortality outcomes and they did not find an association between antidepressant use and mortality (aHR 0.97, 95% CI 0.81–1.17)12. Considering specific drugs, we found a lower risk of mortality with sertraline, escitalopram, amitriptyline, mianserin, and citalopram compared to non-use of antidepressants, and none of the studied specific drugs was associated with increased risk of mortality.
There was a somewhat increased risk of non-psychiatric hospitalization associated with citalopram (5% increased), escitalopram (8%) use, and polytherapy (8%). Citalopram and escitalopram were so widely used altogether that this may have affected to results of all antidepressants observed as a whole. Similarly, as Stroup and colleagues12, we found no association with cardiovascular hospitalizations, and it seems we lacked the statistical power with this outcome (as indicated by wide confidence intervals). Antidepressant use has been associated with certain adverse events28, such as fractures, cardiovascular events, and hyponatremia. However, if these adverse effects would be very severe, contrary to what we found, it probably would have been seen as a higher risk of mortality. Another possible explanation for the small increase in the risk of non-psychiatric hospitalization is that reduction of negative or depressive symptoms, or reduction in diagnostic overshadowing led to improvement in detection of physical diseases and consequently, resulted in a necessary hospitalization.
The strengths of this study are that we used a large nationwide study cohort, including all persons diagnosed with schizophrenia in inpatient care in Finland during a moderately long time period. The inpatient care register has high specificity to identify schizophrenia diagnosis (i.e. no false positive cases)29. In addition, our study enabled a long-term follow-up of up to 22 years, which is required for relatively rare outcomes such as mortality. PRE2DUP method, which we used in this study to derive time periods when drugs were used vs. not used, has been evaluated to estimate antidepressant and antipsychotic use well26,30. For the hospitalization-based outcomes, we used within-individual design, which eliminates the impact of all time-invariant factors such as sex and needs to be adjusted for only time-varying factors. These were sequential order of treatments, time since cohort entry, and use of certain medications.
There are certain limitations in this study. We did not have information on depressive symptoms which can act as a confounder. It is likely that antidepressant use is initiated when the symptoms are present or worsening but the full efficacy of antidepressants is reached after a delay of 2–4 weeks. To overcome this, we ran analyses by omitting the first 30 days from all exposures and the results remained nearly the same as in the main analysis. However, as it was not possible to remove the impact of fluctuation or severity of depressive symptoms in time, our results on the effectiveness of antidepressants in preventing hospitalizations due to psychosis might be an underestimation. Although the diagnosis of schizophrenia is often made in inpatient care, some patients with a less severe course of illness who have been treated only in outpatient care may be missing from our study cohort. Adherence to medication is a common problem in persons with schizophrenia. From the register-based data, we only have information on the dispensed drugs, and it is possible that they are not actually taken. Another limitation is that Finnish registers do not record indications for prescribed medications, i.e., mirtazapine might have been used for the treatment of insomnia, often with relatively low doses, which might affect our results.
In conclusion, antidepressant use was associated with decreased risk of hospitalization due to psychosis and lower mortality among patients with schizophrenia. Although there was a somewhat increased risk of non-psychiatric hospitalization associated with citalopram and escitalopram, we observed a decreased risk of mortality with these substances and with antidepressant use in general, which suggests that antidepressants are relatively safe to use in persons with schizophrenia. However, more studies evaluating the safety and benefits of antidepressant use in persons with schizophrenia are needed.
Data availability
Study datasets include health data and therefore are not publicly available to secure participant privacy. Researchers can apply access to the data from the pertinent register holders: the Social Insurance Institution of Finland (Prescription Register), the National Institute for Health and Welfare (Hospital Discharge Register), and Statistics Finland (National Death Register).
References
Etchecopar-Etchart, D. et al. Comorbid major depressive disorder in schizophrenia: a systematic review and meta-analysis. Schizophr. Bull. 47, 298–308 (2021).
Fond, G. et al. Remission of depression in patients with schizophrenia and comorbid major depressive disorder: results from the FACE-SZ cohort. Br. J. Psychiatry 213, 464–470 (2018).
Puranen, A., Koponen, M., Tanskanen, A., Tiihonen, J. & Taipale, H. Use of antidepressants and mood stabilizers in persons with first-episode schizophrenia. Eur. J. Clin. Pharmacol. 76, 711–718 (2020).
Taipale, H. et al. Antipsychotic use among persons with schizophrenia in Sweden and Finland, trends and differences. Nord. J. Psychiatry 75, 315–322 (2021).
Chakos, M. H. et al. Baseline use of concomitant psychotropic medications to treat schizophrenia in the CATIE trial. Psychiatr. Serv. 57, 1094–1101 (2006).
Himelhoch, S. et al. Antidepressant prescribing patterns among VA patients with schizophrenia. Schizophr. Res. 136, 32–35 (2012).
Olfson, M., Marcus, S. C. & Wan, G. J. Treatment patterns for schizoaffective disorder and schizophrenia among Medicaid patients. Psychiatr. Serv. 60, 210–216 (2009).
Karagianis, J. et al. Worldwide-Schizophrenia Outpatient Health Outcomes (W-SOHO): baseline characteristics of pan-regional observational data from more than 17,000 patients. Int. J. Clin. Pract. 63, 1578–1588 (2009).
Tiihonen, J., Mittendorfer-Rutz, E., Torniainen, M., Alexanderson, K. & Tanskanen, A. Mortality and cumulative exposure to antipsychotics, antidepressants, and benzodiazepines in patients with schizophrenia: an observational follow-up study. Am. J. Psychiatry 173, 600–606 (2016).
Lin, J. Y., Yeh, L. L. & Pan, Y. J. Exposure to psychotropic medications and mortality in schizophrenia: a 5-year national cohort study. Psychol. Med. 22, 1–10 (2022).
Bareis, N., Olfson, M., Wall, M. & Stroup, T. S. Variation in psychotropic medication prescription for adults with schizophrenia in the United States. Psychiatr. Serv. 73, 492–500 (2022).
Stroup, T. S. et al. Comparative effectiveness of adjunctive psychotropic medications in patients with schizophrenia. JAMA Psychiatry 76, 508–515 (2019).
Tiihonen, J., Suokas, J. T., Suvisaari, J. M., Haukka, J. & Korhonen, P. Polypharmacy with antipsychotics, antidepressants, or benzodiazepines and mortality in schizophrenia. Arch. Gen. Psychiatry 69, 476–483 (2012).
Rummel-Kluge, C., Kissling, W. & Leucht, S. Antidepressants for the negative symptoms of schizophrenia (Review). Cochrane Database Syst. Rev. 2006, 1–55 (2006).
Whitehead, C., Moss, S., Cardno, A., Lewis, G. & Furtado, V. A. Antidepressants for people with both schizophrenia and depression. Cochrane Database Syst. Rev. 2002, CD002305 (2002).
Helfer, B. et al. Efficacy and safety of antidepressants added to antipsychotics for schizophrenia: a systematic review and meta-analysis. Am. J. Psychiatry 173, 876–886 (2016).
Galling, B. et al. Efficacy and safety of antidepressant augmentation of continued antipsychotic treatment in patients with schizophrenia. Acta Psychiatr. Scand. 137, 187–205 (2018).
Finnish Medical Society Duodecim. Schizophrenia: Current Care Guideline (accessed 14 March 2022) https://www.kaypahoito.fi/hoi35050 (2022).
Remington, G. et al. Guidelines for the pharmacotherapy of schizophrenia in adults. Can. J. Psychiatry 62, 604–616 (2017).
American Psychiatric Association. The American Psychiatric Association Practice Guideline for the Treatment of Patients with Schizophrenia (American Psychiatric Association Publishing, 2020).
Galderisi, S. et al. EPA guidance on treatment of negative symptoms in schizophrenia. Eur. Psychiatr. 64, e21 (2021).
National Institute of Health and Clinical Excellence. Psychosis and schizophrenia in adults. The NICE Guideline on Treatment and Management (National Institute of Health and Clinical Excellence, accessed 13 January 2022); https://www.nice.org.uk/guidance/cg178/evidence/full-guideline-490503565 (2014).
Buchanan, R. W. et al. The 2009 schizophrenia PORT psychopharmacological treatment recommendations and summary statements. Schizophr. Bull. 36, 71–93 (2010).
Scottish Intercollegiate Guideline Network. Management of Schizophrenia—A National Clinical Guideline http://sign.ac.uk/pdf/sign131.pdf (2013).
Tanskanen, A. et al. From prescription drug purchases to drug use periods – a second generation method (PRE2DUP). BMC Med. Inform. Decision Mak. 15, 21 (2015).
Forsman, J., Taipale, H., Masterman, T., Tiihonen, J. & Tanskanen, A. Comparison of dispensed medications and forensic-toxicological findings to assess pharmacotherapy in the Swedish population 2006 to 2013. Pharmacoepidemiol. Drug Saf. 27, 1112–1122 (2018).
Finnish Medical Society Duodecim. Current Care Guideline: Insomnia (accessed 14 March 2023); https://www.kaypahoito.fi/hoi50067 (2023).
Correll, C. U., Detraux, J., De Lepeleire, J. & De Hert, M. Effects of antipsychotics, antidepressants and mood stabilizers on risk for physical diseases in people with schizophrenia, depression and bipolar disorder. World Psychiatry 14, 119–136 (2015).
Isohanni, M. et al. A comparison of clinical and research DSM-III-R diagnoses of schizophrenia in a Finnish national birth cohort. Clinical and research diagnoses of schizophrenia. Soc. Psychiatry Psychiatr. Epidemiol. 32, 303–308 (1997).
Taipale, H. et al. Agreement between PRE2DUP register data modeling method and comprehensive drug use interview among older persons. Clin. Epidemiol. 8, 363–371 (2016).
Acknowledgements
J.T., H.T., and A.T. have participated in research projects funded by grants from Janssen-Cilag and Eli Lilly to their employing institution. H.T. reports personal fees from Gedeon Richter, Janssen-Cilag, Lundbeck, and Otsuka. J.T. reports personal fees from Eli Lilly, Evidera, Janssen-Cilag, Lundbeck, Mediuutiset, Otsuka, Sidera, and Sunovion; is a consultant to HLS Therapeutics, Orion, and WebMed Global. M.L. is a board member of Genomi Solutions ltd., Springflux ltd., and has received honoraria from Janssen, Janssen-Cilag, Otsuka, Lundbeck, and Recordati and research funding from the Finnish Medical Foundation. This work was supported by the Academy of Finland (grant numbers 315969, 320107, 345326). The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Author information
Authors and Affiliations
Contributions
Study design: all authors, Data acquisition: J.T., Data analyses: A.P., H.T., Drafting the manuscript: A.P., all authors contributed with intellectual input, discussion of the results, and complementing text in the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Puranen, A., Koponen, M., Lähteenvuo, M. et al. Real-world effectiveness of antidepressant use in persons with schizophrenia: within-individual study of 61,889 subjects. Schizophr 9, 34 (2023). https://doi.org/10.1038/s41537-023-00364-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41537-023-00364-x
This article is cited by
-
Excess mortality and its causes among older adults with schizophrenia versus those with bipolar disorder and major depressive disorder: a 5-year prospective multicenter study
European Archives of Psychiatry and Clinical Neuroscience (2024)
