
Abstract
Digit ratio (2D:4D) is a biomarker of prenatal hormone exposure levels; this biomarker is negatively related to prenatal androgen exposure and positively related to prenatal estrogen exposure. We investigated the correlation between digit ratio (2D:4D) and blood pressure. A school-based survey of 687 adolescents aged 8–15 years was conducted. The ring finger (4D) and index finger (2D), systolic blood pressure (SBP), diastolic blood pressure (DBP), testosterone, and estradiol levels were measured. Their dietary behaviors and physical and sedentary activity time were surveyed. The results showed the 2D:4D ratio was not significantly related to SBP, DBP, or testosterone in boys and girls. However, it was significantly positively correlated with serum estradiol levels in boys. The 2D, 4D, multiplied index of digit ratio and length (MIDRL) and average of the index finger and ring finger (AIR) were directly related to SBP in both sexes (βs in boys were 4.16, 5.49, 2.95, and 5.25, respectively, P < 0.01; βs in girls were 3.43, 2.71, 3.02, and 3.36, respectively, P < 0.01) and were also indirectly associated with SBP through testosterone (P < 0.05). The 2D, 4D and AIR were indirectly related to DBP in girls through testosterone (P < 0.05). In conclusion, there were direct and indirect associations between finger-length indicators and blood pressure, which implies that prenatal hormone levels might be correlated with blood pressure in children and adolescents.
Similar content being viewed by others

Introduction
Hypertension in children and adolescents has become a public health issue worldwide [1,2,3,4]. Some studies have shown that higher blood pressure in children and adolescents can increase their risk of adult hypertension [5,6,7] as well as the incidence and rate of mortality from cardiovascular disease [8, 9]. The prevalence of high blood pressure in 122,053 adolescents was 11.2–13% in boys and 9.6% in girls, based on 55 worldwide studies [10]. The incidence of hypertension in children and adolescents has been often overlooked in daily life, and therefore, children and adolescents with high blood pressure need more attention [9].
It is well known that the risk factors for hypertension include genetics, a poor diet, a lack of physical activity, and other environmental factors. Since the hypothesis of a fetal origin of adult diseases was proposed by Professor Barker, an adverse environment for the fetus has been considered one of the important factors related to adult diseases [11]. Some animal-based studies showed that prenatal exposure to excess androgens can lead to diseases such as insulin resistance and hypertension [12, 13]. The digit ratio (2D: 4D) is an biomarker for sex hormone exposure in mothers and is associated with high levels of testosterone in the mother’s body during pregnancy [14]. A low 2D:4D has been commonly suggested to occur due to high prenatal testosterone exposure, while a high 2D:4D indicates low prenatal testosterone exposure [15]. Researchers have speculated that androgens in the mother’s uterus during embryonic development might have a certain stimulating effect on the growth of 4D, while estrogen might stimulated the growth of 2D [16]. Manning et al. [17, 18]. confirmed that the 2D:4D ratio was negatively correlated with circulating androgens in boys and was positively correlated with circulating estrogen in boys and girls. In addition, a rat experiment confirmed these results [19]. Circulating sex hormones play important roles in regulating blood pressure. However, there are few studies on the associations between finger length indicators and blood pressure in children and adolescents.
The purpose of this study was to analyze the association between finger length indicators, such as 2D:4D, and blood pressure in children and adolescents, thus indirectly showing a potential correlation between prenatal hormone levels and childhood blood pressure.
Materials and methods
Participants
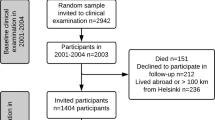
A total of 692 children and adolescents aged 8–15 years were recruited from two nine-year system schools using stratified cluster sampling. The participants were stratified by grades and clustered by classes. The effective number was 683 (98.7% of efficiency), 365 were boys (53.6%), and 318 were girls (46.4%).
Measurements
Medical staff with standardized training were recruited to measure and survey the participants. The length of the index finger (2D) and ring finger (4D) on the left hand were measured with Vernier calipers, and the reading was accurate within 0.01 cm. The participants were asked to keep their fingers straightened and to hold their palms upwards (excluding any finger deformity). One end of the Vernier caliper was aligned with the finger near the palm, while the other end was aligned with the fingertip. Multiplying the index of the digit ratio and length was performed as follows: (MIDRL) = ((2D + 4D)/2) × (2D/4D). The average of the index and ring finger was calculated as follows: (AIR) = (2D + 4D)/2. The participants had their blood pressure measured using a mercury sphygmomanometer. Before measuring their blood pressure, the participants were prohibited from doing strenuous exercise and rested for 10 min. Then, we measured the blood pressure of the right arm two times in a sitting posture, and the second measurement was taken after an interval of 2 min. The final measure recorded was the average of the measured blood pressures. Hearing a Korotkoff I sound was defined as the systolic blood pressure (SBP) and the Korotkoff V sound was defined as the diastolic blood pressure (DBP). Radioimmunoassays were used to measure the circulating testosterone and estradiol using a DFM-96 10 tube radioimmunegamma counter and an estrogen and testosterone kit provided by the DIA source company.
Dietary behaviors were investigated by a homemade food frequency questionnaire, which including frequency of breakfast, milk, eggs, fruits, fresh vegetables, nuts, eating out, carbonated drinks, fried foods, Western-style fast food, and high-energy snacks. Each item on the dietary behaviors questionnaire was assigned 0 points for never, 0.25 points for 1 time per month, 0.5 points for 2 times per month, 2 points for 1–3 times per week, 5 points for 4–6 times per week, and 7 points for 1 time per day. Total scores for healthy dietary behaviors and risky dietary behaviors were calculated. Healthy dietary behaviors included breakfast, milk, eggs, fruits, fresh vegetables, and nuts; risky dietary behaviors included eating out, carbonated drinks, fried foods, Western-style fast food, and high-energy snacks. Physical and sedentary activities were investigated by a class questionnaire [20].
Statistical analysis
Epdiata 3.1 was used for double-entry data. SPSS 23.0 (SPSS Inc., Chicago, IL,USA) was used for statistical analysis. We used the mean ± standard deviation or median (interquartile range) for statistical descriptions of all of the variables, and the differences between the sexes were analyzed using t-tests or Wilcoxon rank tests. The correlations between finger length indicators and testosterone, estradiol, and blood pressure were analyzed by partial correlation after adjusting for their ages. The correlations among dietary behaviors score and physical activities and blood pressure, testosterone and estradiol were analyzed by Spearman rank correlation analysis. The mediating effects of testosterone and estradiol on the association between finger-length indicators and blood pressure were analyzed using multiple linear regression analysis. As shown in (Fig. 1), the independent variable X was the finger length indicators, including 2D, 4D, MIDRL, and AIR, while the dependent variable Y was blood pressure. The mediator variables M were testosterone or estradiol. c was the total effect of X on Y, including the direct effect (c') and the indirect effect (ab), a was the effect of X on M, and b was the effect of M on Y after adjusting for X. The Sobel method was used to test the indirect effect (ab).

The mediating effects of testosterone and estradiol on associations between finger length index and blood pressure
Results
The study effectively surveyed 683 primary and secondary school students, including 365 boys (53.4%) and 318 girls (46.6%). The youngest participant was 6.64 years, and the oldest participant was 15.94 years. The average age was 11.37 years. As shown in Table 1, there was no significant difference in age between boys and girls (P > 0.05). The SBP, 2D:4D, testosterone, healthy dietary behaviors, and risky dietary behaviors in boys were significantly higher than those in girls (P < 0.05). The levels of estradiol and sedentary activities in boys were lower than those in girls (P < 0.01).
As shown in Tables 2, 4D, AIR, and testosterone were positively related to SBP and DBP in boys and girls, respectively (P < 0.05). 2D and MIDRL were significantly correlated with SBP in boys and girls (P < 0.05). Circulating estradiol was negatively correlated with DBP in girls (P < 0.05). However, there were no significant associations between 2D:4D and SBP and DBP in boys or girls (P > 0.05).
As shown in Table 3, there were positive correlations between 2D, 4D, MIDRL, AIR, estradiol and testosterone in boys and girls (P < 0.05). The 2D:4D ratio was significantly positively correlated with estradiol in boys (P < 0.05).
A multiple linear regression analysis was conducted to analyze the mediating effects of testosterone in the association between finger length indicators and blood pressure after adjusting for age and sedentary activities. In boys, the 2D, 4D, MIDRL, and AIR were directly correlated with SBP (βs were 4.16, 5.49, 2.95, and 5.25, P < 0.01), while these parameters were also indirectly correlated with SBP through testosterone (βs were 2.40, 3.39, 1.37, and 3.40, P < 0.01). The proportion of mediating effects of the total effect were 36.6, 36.1, 31.7, and 39.3%, respectively. 2D was indirectly related to DBP through testosterone (β was 0.74, P < 0.01). There were no mediating effects of testosterone on associations among 4D, AIR and DBP in boys. See Table 4 for details.
In girls, the 2D, 4D, MIDRL, and AIR were directly correlated with SBP (βs were 3.43, 2.71, 3.02, and 3.36, P < 0.01), while these parameters were also indirectly correlated with SBP through testosterone (βs were 1.80, 1.41, 1.26, and 1.93, P < 0.01). The proportion of mediating effects of the total effects were 34.5, 34.3, 29.5, and 36.5%, respectively. In addition, the 2D, 4D, and AIR were indirectly associated with DBP through testosterone in girls (βs were 0.74, 0.72, and 0.88, P < 0.01). See Table 5 for details.
Discussion
The results of this study indicated significant differences in systolic blood pressure between boys and girls. Previous studies had shown that blood pressure was higher in boys than in girls during adolescence and puberty in response to the increase in circulating androgen levels [21]. Tebar et al. observed that body mass index and waist circumference were significantly associated with blood pressure in adolescents, and the waist circumference of male adolescents was more strongly correlated with hypertension [22]. In this study, we also found a positive association between circulating testosterone and SBP in boys and girls, and the circulating testosterone in boys was higher than that in girls. The beneficial effects of circulating testosterone were through rapid vasorelaxation of vascular smooth muscle on cardiovascular function [23]. The difference in SBP between sexes may be influenced by circulating testosterone levels.
The 2D:4D ratio is a suitable index to predict prenatal androgen exposure [24]. Previous studies suggested that there was an association between low 2D:4D and levels of fetal testosterone and estradiol [25]. An animal-based study revealed that excess prenatal testosterone exposure could cause hypertension and other problems [12, 13]. However, there was no significant association between 2D:4D ratio and blood pressure in the current study. Manning et al. [17, 18]. reported that the 2D:4D ratio was negatively correlated with circulating androgen in boys and was positively correlated with circulating estrogen in boys and girls. However, the present study showed that the 2D:4D ratio on the left hand was only positively related to circulating estradiol levels in boys, which may be related to racial differences. The previous studies showed that there were significant ethnic differences in digit ratio (2D:4D) [26], such as Finnish and ethnic South Africans (Zulus) with a low digit ratio, Spaniards and Britons with a high digit ratio [27, 28], and Chinese Han children with a lower digit ratio than the others [29]. In addition, the studies showed that the 2D:4D ratio of the right hand was more sensitive to prenatal androgen exposure than that of the left hand [30]. However, the studies of Chinese populations showed that the left hand 2D:4D ratio was more valuable for predicting neuroticism, psychoanalysis, and breast cancer than the right hand 2D:4D ratio [31,32,33]. Chinese participants holding chopsticks and writing with their right hand might influence the growth of 2D and 4D.
The researchers speculated that the androgen in the mother’s uterus during embryonic development stimulated the growth of 4D, while estrogen stimulated the growth of 2D [16]. From the findings of previous studies, we suggested that the digit ratio (2D:4D) might be related to the unbalanced proportion of prenatal androgen and estrogen, and the finger length might be associated with prenatal androgen and estrogen levels, such as 2D with prenatal androgen level, 4D with prenatal estrogen level, and AIR with prenatal androgen and estrogen levels. Thus, we tried to use more information about finger length, including 2D, 4D, MIDRL, and AIR, to analyze the association between finger-length indicators and blood pressure in this study. AIR may represent the average level of androgen and estrogen in the body, while 2D:4D ratio represents the exposure of androgens, and their product can better reflect the dynamic changes of androgen and estrogen in the body. MIDRL, which is a synthesized product of the digit ratio (2D:4D), and AIR may be not only related to overall prenatal hormone exposure but also related to higher prenatal androgen exposure.
After adjusting for age, the results of partial correlations showed that the 2D, 4D, MIDRL, and AIR were significantly related to SBP and testosterone, and there were significant associations between 4D, AIR and DBP and between SBP, DBP and testosterone in boys and girls, which meant our hypothesis was supported. Models examining mediating effects of testosterone on associations between finger length indicators and blood pressure were tested. The results showed that 2D, 4D, MIDRL and AIR were directly correlated with SBP in boys and girls, while they were also indirectly correlated with SBP through testosterone, and the proportion of mediating effects on the total effect were higher than 30%. 2D was indirectly associated with DBP in boys through testosterone, and 2D, 4D and AIR were indirectly correlated with DBP in girls through testosterone. The results indicated that 2D, 4D and relative indexes were directly and indirectly related to blood pressure, especially SBP, which indirectly showed that prenatal androgen and estrogen exposure might directly influence the blood pressure of childhood offspring or be indirectly influenced by testosterone.
Early experience in utero can influence the health of the organism, and hormones, as an epigenetic signal in developmental processes, play an important role in predicting health status [33]. This hypothesis implies that there might be some association between prenatal exposure to high levels of sex hormones, especially testosterone, and blood pressure. Prenatal testosterone might play an organizational role and have resulted in prenatal programming of physiological systems related to the testosterone and estradiol levels of the offspring. Once leaving the uterus, the organism has to accommodate its new external environment, and sometimes some organisms cannot adapt to the new environment, leading to disease. Sex hormones are able to modulate blood pressure by acting on important systems, such as cardiovascular, renal, and neural systems [34]. We suggested that there might be some associations between prenatal sex hormones and blood pressure in children and adolescents, which could be roughly examined using finger-length indicators. However, the specific mechanism of the effects of prenatal hormone exposure on hormone levels in children and adolescents is not currently known, which may be a direction for our future research.
There were several limitations in the present study. Based on a cross-sectional survey, causal relationships between finger-length indicators and blood pressure and testosterone levels could not be evaluated. Given the possible influence of writing and chopsticks use on finger length of the right hand in Chinese participants, only left hand finger lengths were measured in the current study. Some studies have shown that the left hand digit ratio is more closely related to some diseases in the Chinese population [31,32,33]. Moreover, the impact of left-handed students in research has not been considered. The finger length of the right hand should be measured to validate the results in the future.
Informed consent
Informed consent was obtained from the parents of all children included in the study.
References
Ingelfinger JR. The child or adolescent with elevated blood pressure. N Engl J Med. 2014;371:1075.
Dong YH, Zou ZY, Wang ZH, Wang S, Yang ZP, Chen YJ, et al. Analysis on geographic distribution of high blood pressure prevalence in children and adolescents aged 7-18 years in China, 2014. Chin J Prev Med. 2017;38:931–7.
Yan W, Li X, Zhang Y, Niu D, Mu K, Ye Y, et al. Reevaluate secular trends of body size measurements and prevalence of hypertension among Chinese children and adolescents in past two decades. J Hypertens. 2016;34:2337–43.
Hu J, Chu GP, Huang FF, Zhou YK, Teng CG, Yang HB, et al. Relation of body mass index (BMI) to the prevalence of hypertension in children: a 3years’ school-based prospective study in Suzhou, China. Inter J Cardiol. 2016;222:270–4.
Lane DA, Gill P. Ethnicity and tracking blood pressure in children. J Hum Hypertens. 2004;18:223–8.
Lurbe E, Agabiti-Rosei E, Cruickshank JK, Dominiczak A, Erdine S, Hirth A, et al. 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J Hypertens. 2016;34:1887–920.
Roulet C, Bovet P, Brauchli T, Simeoni U, Xi B, Santschi V, et al. Secular trends in blood pressure in children: a systematic review. J Clin Hypertens. 2017;19:488–97.
Ferreira HS, Lucio GM, Assuncao ML, Silva BC, Oliveira JS, Florencio TM, et al. High blood pressure among students in public and private schools in Maceio, Brazil. PLoS ONE. 2015;10:e0142982 https://doi.org/10.1371/journal.pone.0142982
Yang Y, Dong B, Wang S, Dong Y, Zou Z, Fu L, et al. Prevalence of high blood pressure subtypes and its associations with BMI in Chinese children: a national cross-sectional survey. BMC Public Health. 2017;17:598.
de Moraes AC, Lacerda MB, Moreno LA, Horta BL, Carvalho HB. Prevalence of high blood pressure in 122,053 adolescents: a systematic review and meta-regression. Med (Baltim). 2014;93:e232 https://doi.org/10.1097/MD.0000000000000232
Barker DJ, Osmond C. Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. Lancet. 1986;1:1077–81.
King AJ, Olivier NB, Mohankumar PS, Lee JS, Padmanabhan V, Fink GD. Hypertension caused by prenatal testosterone excess in female sheep. Am J Physiol Endocrinol Metab. 2007;292:E1837–41.
Demissie M, Lazic M, Foecking EM, Aird F, Dunaif A, Levine JE. Transient prenatal androgen exposure produces metabolic syndrome in adult female rats. Am J Physiol Endocrinol Metab. 2008;295:E262–68.
Szwed A, Kosinska M, Manning JT. Digit ratio (2D:4D) and month of birth: a link to the solstitial-melatonin-testosterone effect. Early Hum Dev. 2017;104:23–26.
Breedlove SM. Minireview: organizational hypothesis: instances of the fingerpost. Endocrinology. 2010;151:4116–22.
Swaddle JP. Digit ratio: a pointer to fertility, behavior, and health. Heredity. 2002;89:403.
Manning JT, Bundred PE. The ratio of 2nd to 4th digit length: a new predictor of disease predisposition? Med Hypotheses. 2000;54:855–7.
Manning JT, Scutt D, Wilson J, Lewis-Jones DI. The ratio of 2nd to 4th digit length: a predictor of sperm numbers and concentrations of testosterone, luteinizing hormone and oestrogen. Hum Reprod. 1998;13:3000–4.
Yan RH, Bunning M, Wahlsten D, Hurd PL. Digit ratio (2Dratio4D) differences between 20 strains of inbred mice. PLoS One. 2009;4:e5801 https://doi.org/10.1371/journal.pone.0005801
Huang YJ, Wong SH, Salmon J. Reliability and validity of the modified Chinese version of the Children’s Leisure Activities Study Survey (CLASS) questionnaire in assessing physical activity among Hong Kong children. Pediatr Exerc Sci. 2009;21:339–53.
Reckelhoff JF. Gender differences in the regulation of blood pressure. Hypertension. 2001;37:1199–208.
Tebar WR, Ritti-Dias RM, Farah BQ, Zanuto EF, Vanderlei LCM, Christofaro DGD. High blood pressure and its relationship to adiposity in a school-aged population: body mass index vs waist circumference. Hypertens Res. 2018;41:135–40.
Traish AM, Guay A, Feeley R, Saad F. The dark side of testosterone deficiency: I. Metabolic syndrome and erectile dysfunction. J Androl. 2009;30:10–22.
Berenbaum SA, Bryk KK, Nowak N, Quigley CA, Moffat S. Fingers as a marker of prenatal androgen exposure. Endocrinology. 2009;150:5119–24.
Lutchmaya S, Baron-Cohen S, Raggatt P, Knickmeyer R, Manning JT. 2nd to 4th digit ratios, fetal testosterone and estradiol. Early Hum Dev. 2004;77:23–28.
Manning JT, Stewart A, Bundred PE, Trivers RL. Sex and ethnic differences in 2nd to 4th digit ratio of children. Early Hum Dev. 2004;80:161–8.
Manning JT, Henzi P, Venkatramana P, Martin S, Singh D. Second to fourth digit ratio: ethnic differences and family size in English, Indian and South African populations. Ann Hum Biol. 2003;30:579–88.
Manning JT, Barley L, Walton J, Lewis-Jones DI, Trivers RL, Singh D, et al. The 2nd:4th digit ratio, sexual dimorphism, population differences, and reproductive success. evidence for sexually antagonistic genes? Evol Hum Behav. 2000;21:163–83.
Xi H, Li M, Fan Y, Zhao L. A comparison of measurement methods and sexual dimorphism for digit ratio (2D:4D) in Han ethnicity. Arch Sex Behav. 2014;43:329–33.
Mayhew TM, Gillam L, McDonald R, Ebling FJ. Human 2D (index) and 4D (ring) digit lengths: their variation and relationships during the menstrual cycle. J Anat. 2007;211:630–8.
Hong L, Zhan-Bing M, Zhi-Yun S, Xiao-Xia S, Jun-Li Z, Zheng-Hao H. Digit ratio (2D:4D) in Chinese women with breast cancer. Am J Hum Biol. 2014;26:562–4.
Qian W, Huo Z, Lu H, Sheng Y, Geng Z, Ma Z. Digit ratio (2D:4D) in a Chinese population with schizophrenia. Early Hum Dev. 2016;98:45–48.
Sindermann C, Li M, Sariyska R, Lachmann B, Duke E, Cooper A, et al. The 2D:4D-ratio and neuroticism revisited: empirical evidence from Germany and China. Front Psychol. 2016;7:811.
Fowden AL, Forhead AJ. Hormones as epigenetic signals in developmental programming. Exp Physiol. 2009;94:607–25.
Acknowledgements
The authors would like to thank the students who participated in the current study and thank Weige JIANG and Yu LIU for their assistance recruiting students.
Author contributions
YZ and YZ analyzed the data and prepared the first draft of the manuscript, and they contributed equally. TL, ZL, LW, YM, YW, YY, and HH collected data for this study. LF conceived of and designed the study, and revised the manuscript. All authors read and approved the final manuscript.
Funding
This research was supported by grants from the National Natural Science Foundation of China (81502823) and the Outstanding Young Talent Key program of College and University in Anhui province (gxyqZD2017063).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
This project was approved by the Medical Research Ethics Committee of the Bengbu Medical College ([2015] No.003).
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhang, Y., Zhou, Y., Li, T. et al. The association between digit ratio (2D:4D) and blood pressure among children and adolescents. Hypertens Res 42, 876–882 (2019). https://doi.org/10.1038/s41440-018-0199-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-018-0199-x
Keywords
This article is cited by
-
Effects of Puberty on Blood Pressure Trajectories — Underlying Processes
Current Hypertension Reports (2023)
