
Abstract
Idiopathic basal ganglia calcification-1 (IBGC1) is an autosomal dominant disorder characterized by calcification in the basal ganglia, which can manifest a range of neuropsychiatric symptoms, including parkinsonism. We herein describe a 64-year-old Japanese IBGC1 patient with bilateral basal ganglia calcification carrying a novel SLC20A2 variant (p.Val322Glufs*92). The patient also presented with dopa-responsive parkinsonism with decreased dopamine transporter (DAT) density in the bilateral striatum and decreased cardiac 123I-meta-iodobenzylguanidine uptake.
Similar content being viewed by others


Idiopathic basal ganglia calcification (IBGC), also known as Fahr disease or primary familial brain calcification (PFBC), is a disorder characterized by bilateral calcifications in the basal ganglia and other brain regions. Clinical manifestations of IBGC range from asymptomatic to neuropsychiatric symptoms, including dystonia, parkinsonism, ataxia, and cognitive impairment1. Typically, the inheritance mode of familial IBGC is an autosomal dominant one and to date, four dominant causal genes of familial IBGC have been identified, including SLC20A2 (IBGC1, MIM: #213600), PDGFRB (IBGC4, MIM: #615007), PDGFB (IBGC5, MIM: #615483), and XPR1 (IBGC6, MIM: #616413)2,3,4,5. Recently, MYORG was reported as an autosomal recessive causal gene for IBGC (IBGC7, MIM: #618317)6,7. Variants in SLC20A2, encoding the type III sodium-dependent phosphate transporter 2 (PiT-2), are a major cause of IBGC8,9. Herein, we report an IBGC1 patient with a novel variant in SLC20A2 associated with dopa-responsive parkinsonism.
The patient was a 63-year-old Japanese woman who presented to our hospital with a one-month history of lumbago and unsteady gait. Neurological examination revealed gait disturbance with stooped posture and short steps, but rigidity, tremor, weakness, and cerebellar symptoms were not observed. Computed tomography (CT) images of her brain revealed marked calcifications in the bilateral basal ganglia, thalami, and dentate nuclei (Fig. 1a). Laboratory tests showed that serum calcium, phosphate, and intact parathyroid hormone levels were all within the normal ranges. There was no family history of IBGC or parkinsonism. After written informed consent was obtained, we analyzed all the coding regions of the IBGC causative genes, SLC20A2, PDGFRB, and PDGFB, by Sanger sequencing as previously reported10. We diagnosed her as IBGC1 based on the identification of a novel heterozygous frameshift variant, p.Val322Glufs*92 (NM_006749.4:c.965_966delTG, exon 8), in SLC20A2 (Fig. 1b). The variant was absent in the following genome databases: dbSNP 151 (https://www.ncbi.nlm.nih.gov/projects/SNP/), Integrative Japanese Genome Variation Database (http://ijgvd.megabank.tohoku.ac.jp/), Exome Aggregation Consortium database version 0.3.1 (http://exac.broadinstitute.org/), and Human Gene Mutation Database (HGMD® Professional 2019.1).

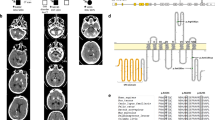
a Computed tomographic (CT) images of the patient show calcifications in the bilateral basal ganglia, thalami, and dentate nuclei. b Electropherogram and sequence of SLC20A2 (NM_006749.4) from the patient’s DNA shows the c.965_966delTG variant. DNA and corresponding amino acid sequences of wild-type and mutant SLC20A2 alleles are also shown. The c.965_966delTG variant causes a frameshift variant (p.Val322Glufs*92). c Dopamine transporter (DAT) single photon emission CT shows diffusely decreased DAT density in the bilateral striatum. The specific binding ratios (SBRs) of both striatum were 0.51 (right) and 0.14 (left). d 123I-meta-iodobenzylguanidine (123I-MIBG) myocardial scintigraphy shows decreased cardiac 123I-MIBG uptake with early and delayed heart to mediastinum (H/M) rates of 1.995 and 1.585, respectively
Ten months after her first visit, she was hospitalized because of difficulties in standing up without assistance at the age of 64. She showed severe bradykinesia, postural instability, and mild symmetric rigidity without tremor. Her Unified Parkinson Disease Rating Scale part III (UPDRS-III) score was 43 of 108 on the ninth hospital day. Her Mini-Mental State Examination score was 24 of 30, and her Hasegawa dementia scale revised was 22 of 30. Dopamine transporter (DAT) single photon emission CT using 123I-ioflupane showed diffusely decreased DAT density in the bilateral striatum (Fig. 1c). The specific binding ratios (SBRs) of both striatum were 0.51 (right) and 0.14 (left). Her 123I-meta-iodobenzylguanidine (123I-MIBG) myocardial scintigraphy revealed reduced cardiac 123I-MIBG uptake with early and delayed heart to mediastinum (H/M) rates of 1.995 and 1.585, respectively (Fig. 1d). Levodopa therapy (200 mg/day) was started on the 14th hospital day and was effective against bradykinesia and postural instability. She was able to walk without assistance in her room. On the 122nd hospital day, she received 600 mg/day of levodopa, and her UPDRS-III score markedly improved from 43 to 11.
The variants associated with IBGC are located widely in SLC20A2 among the patients with IBGC, and the correlation of genotype and phenotype remains unclear1,9,11.
Parkinsonism is one of the common clinical symptoms of IBGC. Tadic et al. showed that 13% of patients with SLC20A2 or PDGFRB variants presented with parkinsonism1. Another review reported motor improvement with dopatherapy in five patients with genetically confirmed IBGC12. Genetically confirmed Japanese IBGC1 patients presenting with parkinsonism have also been reported (Table 1)10,13,14. Among the five variants summarized in Table 1, two variants (c.516+1G>A and c.965_966delTG) are frameshift variants, presumably resulting in loss of function of SLC20A2. In addition, a decreased level of SLC20A2 protein was described in the case with the missense variant (c.1909A>C, S637R), raising the possibility of unstable mutant protein13. Although the functional investigations were not reported for the two missense variants (R71H and G90V), loss-of-function variants are considered for the three variants shown in Table 1. Consistent with previous reports, the majority of variants associated with IBGC are loss-of-function variants8,9, and the present study also suggests that loss-of-function mechanisms are likely involved in at least of the three variants. The present case demonstrated decreased DAT density in the bilateral striatum and decreased cardiac 123I-MIBG uptake (Fig. 1c, d). The decreased DAT density in the bilateral striatum suggested presynaptic dopaminergic dysfunction, which was reported in patients with IBGC14,15,16,17. Saito et al. also showed that postsynaptic dopaminergic dysfunction in the bilateral striatum matched calcified regions16. These findings suggested that basal ganglia calcification might result in dopaminergic dysfunction in IBGC patients. The three cases with reduced DAT density in the striatum (cases 2, 5, and 7. Table 1) also presented with decreased cardiac 123I-MIBG uptake, which was indistinguishable from that observed in patients with Lewy body diseases, including idiopathic Parkinson disease (PD)18. Since PD is a relatively common disease in Japan (prevalence of ~150 per 100,000 persons in Japan)19, the coincidental presence of idiopathic PD and IBGC remains a possibility concerning dopa-responsive parkinsonism of patients with IBGC1. However, it is important to pay attention to patients with IBGC who show dopa-responsive parkinsonism to provide appropriate treatment. To clarify the etiologies of dopa-responsive parkinsonism occasionally observed in patients with IBGC, further functional analyses including DAT SPECT and 123I-MIBG myocardial scintigraphy will be required in a larger number of patients with genetically confirmed IBGC.
HGV Database
The relevant data from this Data Report are hosted at the Human Genome Variation Database at https://doi.org/10.6084/m9.figshare.hgv.2603
References
Tadic, V. et al. Primary familial brain calcification with known gene mutations: a systematic review and challenges of phenotypic characterization. JAMA Neurol. 72, 460–467 (2015).
Wang, C. et al. Mutations in SLC20A2 link familial idiopathic basal ganglia calcification with phosphate homeostasis. Nat. Genet 44, 254–256 (2012).
Keller, A. et al. Mutations in the gene encoding PDGF-B cause brain calcifications in humans and mice. Nat. Genet 45, 1077–1082 (2013).
Nicolas, G. et al. Mutation of the PDGFRB gene as a cause of idiopathic basal ganglia calcification. Neurology 80, 181–187 (2013).
Legati, A. et al. Mutations in XPR1 cause primary familial brain calcification associated with altered phosphate export. Nat. Genet 47, 579–581 (2015).
Yao, X. P. et al. Biallelic mutations in MYORG cause autosomal recessive primary familial brain calcification. Neuron 98, 1116–1123 (2018). e5.
Arkadir, D. et al. MYORG is associated with recessive primary familial brain calcification. Ann. Clin. Transl. Neurol. 6, 106–113 (2019).
Hsu, S. C. et al. Mutations in SLC20A2 are a major cause of familial idiopathic basal ganglia calcification. Neurogenetics 14, 11–22 (2013).
Lemos, R. R. et al. Update and mutational analysis of SLC20A2: a major cause of primary familial brain calcification. Hum. Mutat. 36, 489–495 (2015).
Yamada, M. et al. Evaluation of SLC20A2 mutations that cause idiopathic basal ganglia calcification in Japan. Neurology 82, 705–712 (2014).
Ding, Y. & Dong, H. Q. A novel SLC20A2 mutation associated with familial idiopathic basal ganglia calcification and analysis of the genotype-phenotype association in Chinese patients. Chin. Med J. (Engl.) 131, 799–803 (2018).
Nicolas, G. et al. Phenotypic spectrum of probable and genetically-confirmed idiopathic basal ganglia calcification. Brain 136, 3395–3407 (2013).
Kimura, T. et al. Familial idiopathic basal ganglia calcification: Histopathologic features of an autopsied patient with an SLC20A2 mutation. Neuropathology 36, 365–371 (2016).
Koyama, S. et al. Clinical and radiological diversity in genetically confirmed primary familial brain calcification. Sci. Rep. 7, 12046 (2017).
Paschali, A. et al. Dopamine transporter SPECT/CT and perfusion brain SPECT imaging in idiopathic basal ganglia calcinosis. Clin. Nucl. Med 34, 421–423 (2009).
Saito, T. et al. Neuroradiologic evidence of pre-synaptic and post-synaptic nigrostriatal dopaminergic dysfunction in idiopathic Basal Ganglia calcification: a case report. J. Neuroimaging 20, 189–191 (2010).
Paghera, B., Caobelli, F. & Giubbini, R. 123I-ioflupane SPECT in Fahr disease. J. Neuroimaging 23, 157–158 (2013).
Orimo, S., Suzuki, M., Inaba, A. & Mizusawa, H. 123I-MIBG myocardial scintigraphy for differentiating Parkinson’s disease from other neurodegenerative parkinsonism: a systematic review and meta-analysis. Park. Relat. Disord. 18, 494–500 (2012).
Yamawaki, M., Kusumi, M., Kowa, H. & Nakashima, K. Changes in prevalence and incidence of Parkinson’s disease in Japan during a quarter of a century. Neuroepidemiology 32, 263–269 (2009).
Acknowledgements
This work was supported by Grant-in-Aid (No. H26-Jitsuyoka [Nanbyo]-Ippan-080) from the Ministry of Health, Labour and Welfare, Japan (S.T.).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ichikawa, Y., Tanaka, M., Kurita, E. et al. Novel SLC20A2 variant in a Japanese patient with idiopathic basal ganglia calcification-1 (IBGC1) associated with dopa-responsive parkinsonism. Hum Genome Var 6, 44 (2019). https://doi.org/10.1038/s41439-019-0073-7
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41439-019-0073-7
This article is cited by
-
The clinical and genetic spectrum of primary familial brain calcification
Journal of Neurology (2023)
