
Abstract
Study design
Retrospective cohort study.
Objectives
Although intramedullary astrocytoma is associated with a high mortality rate, the optimal treatment has not reached a consensus. This study aimed at evaluating neurologic function and overall survival rate (OSR) in the treatment of this tumor.
Setting
The single institution in Japan.
Methods
This study enrolled 67 subjects who underwent surgical treatment for intramedullary astrocytoma. Demographic, imaging, and surgical information were collected from each participant. Tumors were histologically categorized using the World Health Organization classification, and subjects were divided into low-grade (I and II; n = 40) and high-grade (III and IV; n = 27) groups. Neurologic status was evaluated using the modified McCormick scale (MMS). OSR was assessed using Kaplan–Meier methods.
Results
The OSR decreased when the pathological grade increased (p < 0.01). Regarding the therapeutic efficacy for low-grade astrocytomas, subjects who underwent gross total resection (GTR) showed a higher OSR than those who did not (p = 0.02). GTR prevented worsening of MMS score, while non-GTR increased the MMS score (p < 0.01). In the high-grade group, 19 and 10 underwent radiation therapy and chemotherapy, respectively. However, both treatments did not improve OSR. Cordotomy was performed for subjects whose lesional area was at the thoracic level, but the OSR did not significantly increase.
Conclusions
The most beneficial therapeutic strategy for low-grade astrocytomas was GTR, whereas that for the high-grade tumors was unclear. Further studies with a larger sample size are warranted to validate the effective treatment for malignant astrocytomas.
Similar content being viewed by others

Introduction
Intramedullary astrocytoma is quite rare, accounting for 6–8% of spinal cord tumors [1, 2]. Astrocytoma is the second most common intramedullary tumor, following ependymoma [2, 3]. The average age at diagnosis was 30 years, and it was more common in men [1, 4,5,6]. Although low-grade malignant tumors such as pilocytic astrocytoma are associated with relatively high survival rates of about 80% at 10 years and a higher malignancy grade, the survival rate decreases substantially to 0–20% [1, 5, 7,8,9,10].
Previous studies have evaluated various effective therapies for spinal cord astrocytomas, but the optimal treatment has not reached a consensus. Particularly, the efficacy of surgical resection is highly controversial. Several studies have shown that gross total resection (GTR) prolongs survival and reduces the recurrence rate [4, 5, 11,12,13,14], whereas others have reported that adjuvant radiation therapy after biopsy leads to better survival than the more invasive surgical resection [1, 15, 16]. The discrepancy could be attributed to the limited number of studied subjects due to the rarity of this tumor. Furthermore, most studies combined both high- and low-grade gliomas in analyzing clinical outcomes, triggering a controversial discussion on the optimal treatment for intramedullary astrocytomas.
Spinal cordotomy or cordectomy is a surgical option for preventing rostral progression of malignant astrocytomas at the thoracic level. In the absence of a beneficial therapy for high-grade malignant tumors, attention has been paid to this procedure as a backstop measure [17, 18]. To minimize the surgical invasiveness and risk of tumor dissemination through the cerebrospinal fluid, we have adopted cordotomy for malignant tumors [18]. However, the efficacy of this approach remains elusive due to insufficient comparative studies.
This study aimed at analyzing predictors for tumor-related death in spinal cord astrocytomas and evaluating the impact of therapeutic effects on overall survival rate (OSR) and neurologic function based on explicit treatment indication via pathological lesional grades.
Methods
Study design and subjects
This is a single-center retrospective study. Overall, 74 subjects underwent surgical treatment for spinal cord astrocytomas between 1977 and 2019. Among the 74 patients, this study focused on the 67 cases that were treated after 1990, at which time motor-evoked potential (MEP) intraoperative neurophysiological monitoring was introduced. Extensive data, including demographic information, medical history, symptomology, imaging findings, and surgery, were collected for each participant. Tumor size was defined as the range of spinal vertebrae according to intramedullary lesional spread using the sagittal plane of magnetic resonance imaging (MRI). To obtain an adequate number of subjects with this rare tumor, the current study included subjects who were participants in our previously published studies [5, 18]. Tumors were histologically categorized using the 2016 World Health Organization (WHO) classification from grade I to IV [19]. Neurologic status was evaluated using the modified McCormick scale (MMS) [20].
Therapeutic indication
GTR, subtotal resection (STR), and biopsy were defined as resection of ≥90%, ≥50% and <90%, and <50% of tumor volumes, respectively [21]. If the tumor was identified as low-grade glioma (WHO grades I and II) in prompt pathological diagnosis during the surgery, GTR was performed. When cases ended with STR or biopsy, postoperative radiation therapy was performed based on patients’ consents. In patients whose diagnosis was grade III or IV gliomas, the surgical resection was limited to biopsy or STR, and additional adjuvant therapy was postoperatively performed. None of the cases underwent duroplasty.
During the surgical resection, we temporarily suspended the surgery when MEPs were attenuated; if the potentials decreased in almost all the monitored muscles, we evacuated the whole tumor, even at the partial resection state.
If the pathological results showed high-grade malignancy (WHO grades III and IV) at the thoracic level, cordotomy was performed from 2003 to prevent rostral tumor progression. Cordotomy was conducted at the upper thoracic level to prevent neurologic deficits in the upper extremities [18].
Statistical analyses
Means ± standard deviations were used to describe continuous variables, and percentages were used to summarize categorical variables in the analyses of predictors for tumor-related death, which was defined as death caused by tumor enlargement or dissemination. Age at surgery, sex, symptom duration, and tumor location, and size were compared between the groups using unpaired t-test for continuous variables and chi-square test for categorical variables. In the survival rate analysis, survival curves were drawn using Kaplan–Meier methods. Potentially significant survival differences were assessed using the log-rank test. Paired t-test was used to evaluate the effect size using the MMS pre- and postoperatively. All statistical analyses were performed using SPSS version 26.0 (SPSS Inc., Chicago, IL). A P-value of <0.05 was considered statistically significant.
Results
Participants
Table 1 summarizes the demographics of 67 patients, which included 38 men (56.7%) and 29 women (43.3%) aged 40.8 ± 18.6 years on average (range: 3–84). The average symptom duration was 14.0 ± 19.1 months (range: 1.0–123.2). The tumor locations were the cervical spinal level in 28 patients (41.8%) and the thoracic level in 39 (58.2%). The tumor range was 3.6 ± 2.5 spinal vertebrae in sagittal MRI (range: 1–18). WHO classification showed that 24 cases (35.8%) were diagnosed as grade I, 16 (23.9%) as grade II, 14 (20.9%) as grade III, and 13 (19.4%) as grade IV. The number of patients who had tumor-related death was 34 (50.7%). There were four patients with regrowth of the residual tumor after partial resection who died because of paralysis progression and subsequent respiratory failure. The other 33 patients (49.3%) were alive during the follow-up period or died due to causes not related to the tumor. The average follow-up duration was 59.9 ± 54.1 months (range: 0.5–210.0), including cases of mortality.
Regarding clinical predictors of tumor-related death, age (p = 0.14), sex (p = 0.40), symptom duration prior to surgery (p = 0.47), and tumor location (p = 0.18) and size (p = 0.98) were not significant prognostic factors (Table 2). Differences in the OSR between the cervical and thoracic spinal levels were not statistically significant (p = 0.70). However, OSR presented worse outcomes as the WHO grade increased (p < 0.01) (Fig. 1).

Overall survival rates according to pathological grade.
Outcomes of survival rate and neurologic function in low-grade astrocytomas
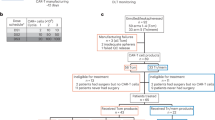
In patients diagnosed with low-grade astrocytomas during the surgery, 18 underwent GTR, while 16 and 6 underwent STR and biopsy, respectively. We only went as far as performing a biopsy in 6 patients because there was a significant reduction in the MEP readings in two patients intraoperatively; and the other four patients were operated on prior to the year 2000 when we lacked consensus on the management of the tumor. OSR was significantly improved when GTR was performed compared to STR or biopsy (p = 0.02) (Fig. 2A). Regarding neurologic assessment, patients who underwent GTR did not show a significant deterioration in MMS during the follow-up period (2.3 ± 0.8 to 2.6 ± 0.8; p = 0.36) (Fig. 2B). However, patients who underwent STR or biopsy presented significantly worse MMS (2.2 ± 0.7 to 3.3 ± 1.1; p < 0.01).

A Overall survival rates after surgical procedures. B Changes in the Modified McCormick Scale preoperatively and at the final follow-up in the group who underwent or did not undergo gross total resection. C Impact of radiation therapy on overall survival rates for subjects who were treated with STR or biopsy.
Of the 22 patients with STR or biopsy, 17 received additional radiation therapy. The average radiation dose was 47.1 ± 3.2 Gy (range: 40.0–50.0). However, this adjuvant therapy did not exert a beneficial effect on the OSR (p = 0.26) (Fig. 2C). Among the 22 patients, two showed tumor regrowth due to malignant transformation and were pathologically diagnosed with pilocytic astrocytoma with anaplastic features following the second surgery.
Outcomes of survival rate in high-grade astrocytomas
Overall, 27 patients had high-grade astrocytomas, and 18 and 9 patients underwent STR and biopsy, respectively. Of these patients, 19 underwent radiation therapy, with an average dose of 47.6 ± 3.3 Gy (range: 40.0–50.4). However, OSR did not show a significant increase in these patients (p = 0.98) (Fig. 3A).

Overall survival rates after radiation therapy (A), chemotherapy (B), and cordotomy (C).
Ten patients received chemotherapy postoperatively. Temozolomide was administered in all patients, and two patients additionally received bevacizumab after temozolomide. However, these chemotherapies did not show favorable life extension for patients with high-grade astrocytomas (p = 0.24) (Fig. 3B).
Ten patients who had lesions at the thoracic level underwent cordotomy after the biopsy. This procedure preserved the residual neurologic function for all ten patients. However, they did not have an improvement in life prognosis compared with those who did not undergo cordotomy (n = 5) (p = 0.43) (Fig. 3C). Eight of the ten patients died, and the causes of death were tumor dissemination to the brain or cervical spinal cord in four patients, lung metastasis in three, and intestinal obstruction in one.
Representative cases
Case 1
A 68-year-old woman visited our hospital because of muscle weakness in her lower extremities. MRI showed an intramedullary tumor from Th8 to Th10 (Fig. 4A, B). A surgical procedure was performed for this patient, and GTR was achieved. The pathological diagnosis was pilocytic astrocytoma (WHO grade I) (Fig. 4C, D). After 5 years from the surgery, there was no finding of tumor recurrence (Fig. 4E, F). The patient was in good condition and could walk using a cane.

A Preoperative T2-weighted MRI and (B) T1-weighted MRI with gadolinium enhancement presented intramedullary tumor at the thoracic spinal levels. C, D Pathological findings show densely fibrillary areas composed of bipolar cells with Rosenthal fibers (C), and GFAP-positive area (D). E T2-weighted MRI and (F) T1-weighted MRI with gadolinium enhancement shows no tumor recurrence 5 years after surgical resection.
Case 2
A 60-year-old man complained of gait disturbance and was referred to our hospital. MRI showed an intramedullary tumor at the spinal levels from C7 to Th3 (Fig. 5A, B). Although surgical treatment was performed, the border between the tumor and cord parenchyma was unclear, and MEPs were attenuated intraoperatively (Fig. 5C, D). The pathological diagnosis was diffuse astrocytoma (WHO grade II) (Fig. 5E, F). The surgery ended with STR, and the remnant tumor persisted at the rostral part (Fig. 5G). Adjuvant radiological therapy was performed; however, the tumor proliferated gradually over time. After 9 years from the surgery, the patient was alive and could walk using a cane (Fig. 5H).

A Preoperative T2-weighted MRI and (B) T1-weighted MRI with gadolinium enhancement present intramedullary tumor at the cervicothoracic spinal levels. C, D Operative findings. The tumor was exposed on myelotomy via the posterior median sulcus and adhered to the cord parenchyma (C). The tumor was debulked using a Cavitron Ultrasonic Surgical Aspirator (Integra Life Sciences Corp., Plainsboro, NJ, USA) (D). E, F Pathological findings show moderately increased cellularity with mild nuclear atypia (E) and present a broad GFAP-positive area (F). G Postoperative T2-weighted MRI. The tumor remained at the rostral part (an arrow). H T2-weighted MRI 9 y postoperatively. The remnant tumor proliferated.
Discussion
This study presented the clinical outcomes of the treatment of intramedullary astrocytomas. In patients with low-grade astrocytomas, GTR resulted in a significantly better survival rate and prevention of neurologic deterioration during the follow-up period. However, in non-GTR, radiation therapy did not contribute to life extension, and neurologic dysfunction progressed compared to the preoperative status. Regarding high-grade astrocytomas, none of the treatments showed efficacy for increasing the survival rate, although adjuvant therapy and cordotomy were performed. Thus, GTR should be performed for low-grade astrocytomas, while further therapeutic development is necessary for high-grade lesions.
As shown in our results, total resection of low-grade astrocytomas led to a favorable survival rate. Consistently, Zhang et al. reported a positive correlation of high resection volume with better survival rate in patients with low-grade spinal cord astrocytomas [21]. This trend was corroborated even when focusing on children with low-grade gliomas; the five-year progression-free survival rate was 88% in patients who underwent GTR but decreased to 34% in those who received other therapies [12]. Regarding postoperative neurologic function, in our study, patients who underwent GTR did not show significant functional deterioration and retained their neurologic status. However, in their study targeting children, Scheinemann et al. reported that 52% of patients with low-grade glioma showed neurologic sequelae postoperatively [12]. Since radical surgical resection potentially results in functional deterioration in return for survival improvement, a careful and safe surgical technique is still required to prevent postoperative neurologic dysfunction.
In contrast to the favorable outcomes for low-grade astrocytomas after GTR, survival prognosis was not significantly improved unless total resection was performed. Similar results were observed in other studies, which demonstrated that partial resection was related to a worse prognosis [12, 21,22,23,24]. Furthermore, our study demonstrated that neurologic function became worse at the final follow-up in the group that did not undergo GTR. The cause for this neurologic deterioration could be an intraoperative excessive invasion, which was identified by a decrease or disappearance of MEP waveforms, resulting in surgical cessation and insufficient resection volume. Another possibility was exacerbated compression from the inner side of the spinal cord by a proliferation of remnant tumors during the observation period. The postoperative neurological function is directly linked to the survival rate [25, 26]; therefore, GTR should be the aim in all cases for improving patient prognosis.
When ended to partial resection at initial surgery; however, one solution could be performing two-stage surgery to accomplish GTR [27, 28]. According to previous studies, myelotomy and partial resection were performed at the initial surgery, and this procedure led to extrusion of remnant intramedullary astrocytomas, owing to intraparenchymal pressure. After a few weeks, the second surgery was performed, and the extruded tumor was better defined from the adjacent spinal cord, which allowed complete tumorectomy without neurologic deficits. Because this approach was recommended especially for low-grade astrocytomas [27], the surgeon has an option to perform two-stage surgery to achieve GTR without neurologic injury and obtaining informed consent on this procedure from the patient before surgery would be better.
For high-grade malignant astrocytomas, determining and performing the optimal treatment is still a challenge. These tumors tend to infiltrate the spinal cord tissue; therefore, GTR is rarely possible [11, 29, 30]. Therefore, in patients who had lesions at the thoracic spinal levels, we have adopted cordotomy for malignant astrocytomas [18]. Although 2 of the 10 patients who underwent cordotomy survived, there was no significant improvement in prognosis compared with that in those who did not undergo cordotomy (Fig. 3C). The possible cause of the negative outcome was the dissemination that occurred during biopsy as primary surgery. Even after the biopsy, subarachnoid seeding of the tumor could progress by the time cordotomy was performed. The residual tumor had the potential to metastasize, and in fact, several patients in the present study developed lung metastasis. Although there was no case in our series, malignant astrocytoma was reported to trigger metastasis to the liver and spleen [31]. To overcome these issues, spinal cord resection (cordectomy) might be another surgical procedure as reported in previous studies [17, 32, 33]. While the beneficial result was reported with long-term survival of >10 years in a pediatric patient [17], several studies presented tumor-related death even after cordectomy [32, 33]. In either surgical technique, further study with a larger sample size will be necessary to validate the effectiveness of these procedures for survival prognosis.
We found no evidence to support the efficacy of radiation therapy for either low- or high-grade malignant groups in the present study. Several previous studies similarly did not show a beneficial effect of radiation therapy on the survival rate [30, 34], although others showed an improvement for low-[35] and high-grade astrocytomas [1, 4]. This discrepancy might be attributed to the selection bias of subjects who received radiation therapy because we did not conduct this adjuvant treatment for all patients but mainly for those who underwent biopsy or STR only. Depending on the amount of excision, and timing, and dose of radiation, the survival rate may be increased, but the number of patients is currently small, and statistically powerful evidence cannot be provided.
Regarding chemotherapy, temozolomide was demonstrated to increase the survival rate of subjects with intracranial glioblastoma [36]. Since these reports, this drug has been used to treat both high- and low-grade malignant gliomas in the spinal cord [37, 38]. Although this treatment for spinal tumors probably contributes to better outcomes, including longer survival times, the published findings are all case series or reports with limited numbers of subjects. In our study, all ten subjects who underwent chemotherapy for high-grade astrocytomas received temozolomide, but the drug did not show a positive impact on the survival rate. In fact, recent systematic reviews focusing on spinal cord glioblastomas did not reveal a statistically significant survival benefit of temozolomide treatment [39]. Fakhreddine et al. also reported that temozolomide did not improve the OSR in patients with WHO grade II to IV [40]. In another study, bevacizumab was administered to six subjects with spinal cord glioblastoma after treatment with irradiation and temozolomide and showed a moderate beneficial effect on survival with tolerable toxicity [41]. Taken together, further studies are necessary to confirm the impact of temozolomide and bevacizumab
Although the WHO classification is a gold standard for evaluating the prognosis and deciding the therapeutic strategy, this histological classification is not trivial and involves interobserver variability [42]. Moreover, the clinical behavior of each tumor can vary based on the specific histological entity. From this perspective, additional markers are crucial for the objective classification of astrocytomas and administration of customized therapy. With the development of molecular neuro-oncology, recent studies have focused on molecular diagnosis as clinically relevant tissue-based biomarkers. In the present study, owing to the retrospective and long-observational design, we did not evaluate the molecular diagnostics and have introduced several typical markers for the astrocytomas based on our literature review. A representative marker is a duplication/fusion of the BRAF gene in pilocytic astrocytomas (grade I), and it helps in distinguishing this tumor from diffuse astrocytomas [43]. Including our two cases, malignant transformation of pilocytic astrocytomas with anaplastic features is rare; however, Olar et al. reported that ATRX protein loss and deregulation of the PI3K/AKT pathway is common in patients with this tumor [44]. A small subset of the tumor has H3-K27M mutations or FGFR1 duplication [45, 46]. With regard to diffuse (grade II), anaplastic (grade III) astrocytomas, and secondary glioblastomas (grade IV), IDH1 mutation and MGMT promoter methylation are frequently detected [42, 47]. IDH1 mutation is linked to a better prognosis [48]. Primary glioblastoma presents EGFR amplification and PTEN mutation; however, it lacks IDH1 mutation [49]. MGMT methylation is also occasionally found in the primary glioblastoma, and hypermethylation of this gene is associated with a favorable response to chemotherapy [50]. Most of the markers have been identified using brain samples; therefore, further analyses are necessary for the assessment of molecular diagnostics in astrocytomas that occur in the spinal cord.
This study has several limitations, including its retrospective nature. First, the sample size was relatively small and was insufficient to validate our results regarding the predictors and survival rate, and thus, the level of evidence is low and the results should be interpreted cautiously. It is crucial to continue registering subjects for future studies with larger sample sizes. Second, we examined consecutive subjects who presented to us over 30 years of practice; the diagnosis, pathological assessment, therapeutic principles, surgical procedures, intraoperative monitoring, and imaging modality have changed over this long period. These diversities could have substantially influenced the clinical outcomes. Finally, several surgeons performed the surgery in this series, raising the possibility that surgical outcomes may have been affected by differences in the surgeons’ experience and techniques.
Conclusions
For low-grade intramedullary astrocytomas, GTR provided beneficial effects for survival rate and prevention of neurologic deterioration. If the tumor remained, the neurologic function was impaired, and the prognosis for life expectancy was reduced. Regarding high-grade astrocytomas, neither cordotomy for thoracic spinal levels, chemotherapy nor radiotherapy improved the survival rate. However, caution is warranted while interpreting these results owing to the low evidence level. Further research on a larger sample is required to establish the effective treatment for malignant astrocytomas.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Minehan KJ, Brown PD, Scheithauer BW, Krauss WE, Wright MP. Prognosis and treatment of spinal cord astrocytoma. Int J Radiat Oncol Biol Phys. 2009;73:727–33.
Ardeshiri A, Chen B, Hutter BO, Oezkan N, Wanke I, Sure U, et al. Intramedullary spinal cord astrocytomas: the influence of localization and tumor extension on resectability and functional outcome. Acta Neurochirurg. 2013;155:1203–7.
Corradini S, Hadi I, Hankel V, Ertl L, Ganswindt U, Belka C, et al. Radiotherapy of spinal cord gliomas: a retrospective mono-institutional analysis. Strahlenther Onkol. 2016;192:139–45.
Adams H, Avendano J, Raza SM, Gokaslan ZL, Jallo GI, Quinones-Hinojosa A. Prognostic factors and survival in primary malignant astrocytomas of the spinal cord: a population-based analysis from 1973 to 2007. Spine. 2012;37:E727–735.
Nakamura M, Chiba K, Ishii K, Ogawa Y, Takaishi H, Matsumoto M, et al. Surgical outcomes of spinal cord astrocytomas. Spinal Cord. 2006;44:740–5.
Xiao R, Abdullah KG, Miller JA, Lubelski D, Steinmetz MP, Shin JH, et al. Molecular and clinical prognostic factors for favorable outcome following surgical resection of adult intramedullary spinal cord astrocytomas. Clin Neurol Neurosurg. 2016;144:82–7.
Babu R, Karikari IO, Owens TR, Bagley CA. Spinal cord astrocytomas: a modern 20-year experience at a single institution. Spine. 2014;39:533–40.
Liu A, Sankey EW, Bettegowda C, Burger PC, Jallo GI, Groves ML. Poor prognosis despite aggressive treatment in adults with intramedullary spinal cord glioblastoma. J Clin Neurosci. 2015;22:1628–31.
Seki T, Hida K, Yano S, Aoyama T, Koyanagi I, Houkin K. Surgical outcomes of high-grade spinal cord gliomas. Asian Spine J. 2015;9:935–41.
Raco A, Piccirilli M, Landi A, Lenzi J, Delfini R, Cantore G. High-grade intramedullary astrocytomas: 30 years’ experience at the Neurosurgery Department of the University of Rome “Sapienza”. J Neurosurg Spine. 2010;12:144–53.
McGirt MJ, Goldstein IM, Chaichana KL, Tobias ME, Kothbauer KF, Jallo GI. Extent of surgical resection of malignant astrocytomas of the spinal cord: outcome analysis of 35 patients. Neurosurgery. 2008;63:55–60.
Scheinemann K, Bartels U, Huang A, Hawkins C, Kulkarni AV, Bouffet E, et al. Survival and functional outcome of childhood spinal cord low-grade gliomas. Clinical article. J Neurosurg Pediatr. 2009;4:254–61.
Jiang Y, Lv L, Yin S, Zhou P, Jiang S. Primary spinal pilocytic astrocytoma: clinical study with long-term follow-up in 16 patients and a literature review. Neurosurg Rev. 2020;43:719–27.
Wong AP, Dahdaleh NS, Fessler RG, Melkonian SC, Lin Y, Smith ZA, et al. Risk factors and long-term survival in adult patients with primary malignant spinal cord astrocytomas. J Neurooncol. 2013;115:493–503.
Innocenzi G, Salvati M, Cervoni L, Delfini R, Cantore G. Prognostic factors in intramedullary astrocytomas. Clin Neurol Neurosurg. 1997;99:1–5.
Minehan KJ, Shaw EG, Scheithauer BW, Davis DL, Onofrio BM. Spinal cord astrocytoma: pathological and treatment considerations. J Neurosurg. 1995;83:590–5.
Crowley RW, Burke RM, Lopes MB, Hamilton DK, Jane JA Sr. Long-term cure of high-grade spinal cord glioma in a pediatric patient who underwent cordectomy. J Neurosurg Spine. 2015;23:635–41.
Nakamura M, Tsuji O, Fujiyoshi K, Watanabe K, Tsuji T, Ishii K, et al. Cordotomy for patients with thoracic malignant astrocytoma. J Neurosurg Spine. 2010;13:418–23.
Louis DN. WHO classification and grading of tumours of the central nervous system. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. (eds). WHO Classification of Tumours of the Central Nervous. 4th ed. International Agency for Research on Cancer, Lyon,2016;201;pp12–13.
McCormick PC, Stein BM. Intramedullary tumors in adults. Neurosurg Clin N Am. 1990;1:609–30.
Zhang YW, Chai RC, Cao R, Jiang WJ, Liu WH, Xu YL, et al. Clinicopathological characteristics and survival of spinal cord astrocytomas. Cancer Med. 2020;9:6996–7006.
Zou Y, Sun J, Zhou Y, Bai HX, Huang X, Babu R, et al. Prognostic factors and treatment of spinal astrocytomas: a multi-institutional cohort analysis. Spine. 2018;43:E565–573.
Luksik AS, Garzon-Muvdi T, Yang W, Huang J, Jallo GI. Pediatric spinal cord astrocytomas: a retrospective study of 348 patients from the SEER database. J Neurosurg Pediatr. 2017;19:711–9.
Khalid S, Kelly R, Carlton A, Wu R, Peta A, Melville P, et al. Adult intradural intramedullary astrocytomas: a multicenter analysis. J Spine Surg. 2019;5:19–30.
Lee HK, Chang EL, Fuller GN, Aldape KD, Atkinson GJ, Levy LB, et al. The prognostic value of neurologic function in astrocytic spinal cord glioma. Neuro-Oncology. 2003;5:208–13.
Seki T, Hida K, Yano S, Aoyama T, Koyanagi I, Sasamori T, et al. Clinical factors for prognosis and treatment guidance of spinal cord astrocytoma. Asian Spine J. 2016;10:748–54.
Hida K, Iwasaki Y, Seki T, Yano S. two-stage operation for resection of spinal cord astrocytomas: technical case report of three cases. Neurosurgery. 2006;58:E373–373.
Benzel EC, Mirfarkhraee M, Hadden T, Fowler M. Holocord astrocytoma: a two-staged operative approach. Spine. 1987;12:746–9.
Yanamadala V, Koffie RM, Shankar GM, Kumar JI, Buchlak QD, Puthenpura V, et al. Spinal cord glioblastoma: 25 years of experience from a single institution. J Clin Neurosci. 2016;27:138–41.
Przybylski GJ, Albright AL, Martinez AJ. Spinal cord astrocytomas: long-term results comparing treatments in children. Childs Nerv Syst. 1997;13:375–82.
Santi M, Mena H, Wong K, Koeller K, Olsen C, Rushing EJ. Spinal cord malignant astrocytomas. Clinicopathologic features in 36 cases. Cancer. 2003;98:554–61.
Marchan EM, Sekula RF Jr, Jannetta PJ, Quigley MR. Long-term survival enhanced by cordectomy in a patient with a spinal glioblastoma multiforme and paraplegia. Case report. J Neurosurg Spine. 2007;7:656–9.
Kyoshima K, Ito K, Tanabe A, Iwashita T, Goto T, Sato A, et al. Malignant astrocytoma of the conus medullaris treated by spinal cordectomy. J Clin Neurosci. 2002;9:211–6.
Lam S, Lin Y, Melkonian S. Analysis of risk factors and survival in pediatric high-grade spinal cord astrocytoma: a population-based study. Pediatr Neurosurg. 2012;48:299–305.
Kim MS, Chung CK, Choe G, Kim IH, Kim HJ. Intramedullary spinal cord astrocytoma in adults: postoperative outcome. J Neurooncol. 2001;52:85–94.
Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;352:997–1003.
Chamberlain MC. Temozolomide for recurrent low-grade spinal cord gliomas in adults. Cancer. 2008;113:1019–24.
Kim WH, Yoon SH, Kim CY, Kim KJ, Lee MM, Choe G, et al. Temozolomide for malignant primary spinal cord glioma: an experience of six cases and a literature review. J Neurooncol. 2011;101:247–54.
Hernandez-Duran S, Bregy A, Shah AH, Hanft S, Komotar RJ, Manzano GR. Primary spinal cord glioblastoma multiforme treated with temozolomide. J Clin Neurosci. 2015;22:1877–82.
Fakhreddine MH, Mahajan A, Penas-Prado M, Weinberg J, McCutcheon IE, Puduvalli V, et al. Treatment, prognostic factors, and outcomes in spinal cord astrocytomas. Neuro-Oncology. 2013;15:406–12.
Chamberlain MC, Johnston SK. Recurrent spinal cord glioblastoma: salvage therapy with bevacizumab. J Neurooncol. 2011;102:427–32.
Riemenschneider MJ, Jeuken JW, Wesseling P, Reifenberger G. Molecular diagnostics of gliomas: state of the art. Acta Neuropathol. 2010;120:567–84.
Collins VP, Jones DT, Giannini C. Pilocytic astrocytoma: pathology, molecular mechanisms and markers. Acta Neuropathol. 2015;129:775–88.
Olar A, Tran D, Mehta VP, Reinhardt A, Manekia JH, Garnovskaya M, et al. ATRX protein loss and deregulation of PI3K/AKT pathway is frequent in pilocytic astrocytoma with anaplastic features. Clin Neuropathol. 2019;38:59–73.
Ballester LY, Penas-Prado M, Leeds NE, Huse JT, Fuller GN. FGFR1 tyrosine kinase domain duplication in pilocytic astrocytoma with anaplasia. Cold Spring Harb Mol Case Stud. 2018;4:a002378.
Rodriguez FJ, Brosnan-Cashman JA, Allen SJ, Vizcaino MA, Giannini C, Camelo-Piragua S, et al. Alternative lengthening of telomeres, ATRX loss and H3-K27M mutations in histologically defined pilocytic astrocytoma with anaplasia. Brain Pathol. 2019;29:126–40.
Yan H, Parsons DW, Jin G, McLendon R, Rasheed BA, Yuan W, et al. IDH1 and IDH2 mutations in gliomas. N Engl J Med. 2009;360:765–73.
Parsons DW, Jones S, Zhang X, Lin JC, Leary RJ, Angenendt P, et al. An integrated genomic analysis of human glioblastoma multiforme. Science. 2008;321:1807–12.
Ohgaki H, Kleihues P. Genetic pathways to primary and secondary glioblastoma. Am J Pathol. 2007;170:1445–53.
Herrlinger U, Rieger J, Koch D, Loeser S, Blaschke B, Kortmann RD. et al. Phase II trial of lomustine plus temozolomide chemotherapy in addition to radiotherapy in newly diagnosed glioblastoma: UKT-03. J Clin Oncol. 2006;24:4412–7.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
N.N. and M.N. designed the research; N.N. analyzed the data and wrote the paper; O.T., H.O., M.M., M.N., and K.W. performed data collection; O.T., K.I., M.M., M.N. and K.W. supervised the study; all authors reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study received ethical approval from the institutional review board (20110142). We certify that all applicable institutional regulations concerning the ethical use of human volunteers were followed during the course of this research.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nagoshi, N., Tsuji, O., Suzuki, S. et al. Clinical outcomes and a therapeutic indication of intramedullary spinal cord astrocytoma. Spinal Cord 60, 216–222 (2022). https://doi.org/10.1038/s41393-021-00676-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-021-00676-8
This article is cited by
-
Does the degree of preoperative gait disturbance remain after tumor resection in patients with intradural extramedullary spinal cord tumors?
Spinal Cord (2023)
-
Predictors of survival and time to progression following operative management of intramedullary spinal cord astrocytomas
Journal of Neuro-Oncology (2022)
