
Abstract
Study design
Cross-sectional survey.
Objective
To assess quality of life (QOL) and the predictors of QOL in people with spinal cord injury (SCI).
Setting
Shanghai Yangzhi Rehabilitation Hospital, Mainland China.
Methods
Three hundred adult participants with SCI completed standardized self-report measures. The study assessed QOL, demographic and injury variables, psychological factors and community participation. Psychological factors included resilience, post-traumatic growth, post-traumatic stress disorder, anxiety and depression. Descriptive analyses were used to calculate the QOL, psychological outcomes, and community participation scores. The relationship between all the factors was examined using Pearson correlation analysis. Regression analyses were performed to determine the independent predictors of QOL.
Results
The mean range of items for four domains of QOL was from 3.0 to 3.2. Resilience and post-traumatic growth showed significant positive relationships with each domain of QOL (range of r from 0.26 to 0.53, p < 0.01). Post-traumatic stress disorder, anxiety, and depression showed negative relationships with each domain of QOL (range of r from −0.67 to −0.27, p < 0.01). Community participation showed weak significant relationships with three domains of QOL. Participants’ self-reported perception of environmental barriers and the five psychological outcomes were the most significant predictors of QOL. Community participation did not show any predictive effect.
Conclusions
The QOL of people with SCI in Mainland China needs improvement. Many factors influence QOL, especially psychological outcome variables. Promoting mental health in individuals with SCI is critical to improving overall QOL.
Similar content being viewed by others


Introduction
Spinal cord injury (SCI) is becoming a more common cause of long-term disability. It results in decreased quality of life (QOL) due to body activity and participation limitations [1]. SCI is a low-prevalence condition, but there are more than 1 million people in Mainland China currently living with a SCI. The number of people who sustained SCI is growing at a rate of ~120,000 new cases every year [2]. How to promote the QOL of this group has become an urgent task for the Department of Health in China.
QOL is defined by World Health Organization (WHO) as “an individual’s perception of their position in life, in the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards, and concerns” [3]. Clinicians can use QOL analysis to understand whether an individual with SCI is living well, and proper QOL assessment is vital for individuals with SCI, as it can contribute to developing better interventions and plans of care for these individuals. Previous studies have used the life satisfaction questionaire, the medical outcomes study short form (SF-36), and the World Health Organization Quality of Life Scale Brief Version (WHOQOL-BREF) questionnaire to assess the QOL of people with SCI [1, 4, 5]. The WHOQOL-BREF is a commonly utilized measure of QOL and is available in ~40 different languages [6, 7]. Its purpose is to provide a direct comparison between people with different health states and cultural settings. The official Chinese version of WHOQOL-BREF was developed and formally approved by the WHOQOL Group in 1999 and for this study we chose the WHOQOL-BREF to assess the QOL of people with SCI. Therefore, the first purpose of current study was to explore the QOL of people with SCI in Mainland China.
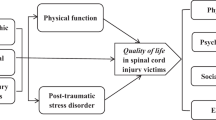
QOL is a complicated concept and can be affected by many factors. Several studies have confirmed that some socio-demographic and psychological factors are strongly correlated with QOL [1]. Researchers have observed strong correlations between environmental factors and QOL in people with SCI [8]. Environmental factors include general accessibility and opportunities for employment [8]. Community participation is considered an indicator of rehabilitation outcomes. Participation in the home and in leisure activities has been shown to have a positive effect on QOL [3]. Literature supports the finding that people with SCI can increase their overall wellbeing through satisfactory social participation [9]. The second purpose of this study was to assess the predictive quality of the factors that can affect QOL. Researchers have proposed that successful rehabilitation should incorporate physical, social, and psychological components [10]. We hypothesize that the psychological variables and community participation have significant impacts on QOL.
Methods
Participants and procedures
The research proposal received ethical approval from the ethics committee of Tongji University and Shanghai Yangzhi Rehabilitation Hospital. Inclusion criteria for participants included: (a) SCI caused by traumatic injury, (b) aged between 18 and 65 years old, and (c) lived with the injury for at least 6 months.
Individuals with a head injury or communication disorder were ineligible. Shanghai Yangzhi Rehabilitation Hospital’s ‘halfway house’ project provided the participants. Project ‘halfway house’ is a government-supported program that provides rehabilitation training for free. Researchers asked those participants who agreed to participate in the study to complete the survey soon after admission to the rehabilitation hospital’s halfway house, in order to capture information on their perceptions before the rehabilitative activities began. There were 320 individuals invited to complete the questionnaire between March 2015 and December 2017. Excluding 20 invalid questionnaires, the final sample of the study was 300.
Measures
The participants provided demographic data (e.g., age, education, marital status, religion) and injury characteristics (e.g. cause of injury, length of time since their injury). Participants’ self-report about environmental barriers was assessed using a 5-point Likert scale, from 1 for unrestricted to 5 for extremely restricted.
Quality of life
The mainland Chinese version of the WHOQOL-BREF consists of 28 items; 26 standard items from the original WHOQOL-BREF supplemented by two items that are unique to China [11]. The original Chinese developers recommended these two culturally specific items “Does family friction affect your life?” and “How is your appetite?”, which are not included in any domain score to maintain the comparability with the standard WHOQOL-BREF. The two additional items were not used in this study [11]. The WHOQOL-BREF questionnaire in this study consists of only the original 26 items. Items 1 and 2 assess an individual’s overall perception of QOL and health, respectively. The remaining 24 items are grouped into four domains: physical (7 items), psychological (6 items), social relationships (3 items), and environment (8 items). Each item is rated on a 5-point Likert scale. The responses are scaled in a positive direction. The mean score of the items within each domain was used to calculate the raw score. Raw scores were then transformed to a 0–100 scale using a transformation formula [Formula = (raw scores−4)(100/16)]. A higher score reflects a better QOL. Cronbach’s α of QOL was 0.952 in this study.
Psychological outcomes
The researchers investigated five common psychological outcome variables. Positive psychological outcomes included measures of resilience and post-traumatic growth (PTG). Post-traumatic stress disorder (PTSD) symptoms, anxiety, and depression were chosen as the indicators of psychological morbidity for the current sample. The inventories used in this study were the same as those in our previous study [12].
Community participation
The Craig Handicap Assessment and Reporting Technique Short Form (CHART-SF) follows the WHO’s model of handicap dimensions [13]. It consists of 19 questions covering Physical Independence, Cognitive Independence, Mobility, Occupation, Social Integration, and Economic Self-Sufficiency. Each of the six subscale scores, ranges from 0 (complete handicap) to 100 (no handicap). The CHART-SF has demonstrated adequate reliability (test–retest reliability coefficient = 0.93) and validity (e.g., 0.83 correlation between subject and proxy reports) among individuals with SCI [13]. The cognitive independence domain was deleted because none of the participants had cognitive problems. Economic self-sufficiency was also deleted because most participants did not like to talk about their economic status to other people. Some people found it difficult to estimate the family income. Thus, four domains: physical independence, mobility, occupation, and social integration were assessed. Cronbach’s α of CHART-SF was 0.82 in this study.
Statistical analysis
SPSS version 22.0 was used for the analysis of data. All data were entered into the SPSS database by two people on different machines. The descriptive analysis included the means and standard deviations of the main variables. Pearson correlations were used to examine potential relationships within the data, primarily between the demographic and injury characteristics with the four domains of QOL. This analysis was to identify potential covariates. Then, Pearson’s correlation coefficients were calculated to determine the correlations of the five psychological variables and community participation with four domains of QOL. Secondly, hierarchical linear regressions were performed. We used the social demographic data, psychological outcomes and community participation as predictor variables and all four domains of QOL, excluding items 1 and 2, as outcome variables. Hierarchical multiple regression (HMR) analysis was used to determine incremental variance that can be accounted by each predictor set in the analysis. Only the factors that were found to be correlated with QOL were included in the regression. The ‘enter’ method was used for all steps. Cronbach’s alpha coefficients were calculated for all scales. All statistical tests were two-tailed with an alpha level of 0.05. A p-value < 0.05 was considered to be statistically significant.
Results
Participant characteristics
The mean age at the time of the study was 45.69 years (SD, 12.87; range, 18–65) and the mean age at injury was 33.80(14.28, range, 3–64). The demographic and injury characteristics of the study population (N = 300) are presented in Table 1.
Descriptive statistics
Means and standard deviations for measures of the variable are presented in Table 2. The means of overall QOL and general health were 3.0 and 2.7, respectively. The means of the different items were as follows: physical health 3.0, psychological health 3.2, social relationships 3.2, and environmental health 3.1. The means of transformed scores for the four domains were as follows: physical 50.3, psychological 55.2, social 54.2, and environmental 51.5. As for the four variables of community participation, there were great differences. The means from high to low were physical independence 81.9, social integration 70.8, mobility 47.9, and occupation 33.1.
Correlation analysis
Correlations between demographic and injury characteristics and the four QOL domains are shown in Table 3. Significantly negative correlations were observed between: age at the time of the study and the physical domain (r = −0.26, p < 0.01); age at injury and the physical domain (r = −0.31, p < 0.01); age at injury and the psychological domain (−0.25, p < 0.01); and age at injury and the environmental (−0.17, p < 0.01). Significantly positive correlations were observed between: duration since injury and the psychological domain (r = 0.15, p < 0.01); level of lesion and physical domain (r = 0.21, p < 0.01); and gender and social domain (r = 0.16, p < 0.01). Participants’ report of environmental barriers was negatively associated with the four domains of QOL.
Table 3 tabulates the correlations between psychological variables and QOL scores in different domains. The results indicate that positive psychological variables (resilience and PTG) were moderately positively correlated with the psychological domains. The positive psychological variables (resilience and PTG) and the physical, social, and environmental QOL domains had weak positive correlations. As expected, the three negative psychological variables (PTSD, anxiety, and depression) were moderately negatively correlated with the physical and psychological domains. Weak negative correlations were found between three of the negative psychological variables (PTSD, anxiety, and depression) and the social and environmental QOL domains.
Correlations between four factors of community participation and the four domains of QOL were observed (see Table 3). Significant weak correlations were observed between the community participation and the QOL domains (r = 0.15–0.35).
HMR analysis
HMR analysis was performed to identify the relative contribution of the independent variables to the four domains of QOL (see Table 4). The four domains of QOL were regressed separately as dependent variables. All variables related to the four domains of QOL were entered into the model. Those considered as the same category were entered as a block at each step. Five demographic and injury variables were entered on the first step as the control variables. Compared with community participation, psychological variables were more likely to be antecedents. Five psychological variables were then entered on the second step. Four factors of community participation were finally entered in the equation.
Overall, different combinations of predictors accounted for 52.9% of the variance in physical health, 57% of the variance in psychological health, 33% of the variance in social health, and 29.2% of the variance in environmental health. In the model of physical health, five significant predictors were found. They consisted of two control variables (age at injury and self-report of environmental barriers), three psychological variables (resilience, PTSD, and anxiety). In the model of psychological health, six significant predictors were screened. They were the extent of environmental barriers and all five psychological variables. In the social health model, four significant predictors were confirmed: gender, resilience, PTG, and anxiety. In the model of environmental health, only the report of environmental barriers (β = −0.38, p < 0.05) and resilience (β = 0.25, p < 0.05) were significant predictors. Compared with psychological outcomes variables, community participation had a less predictive effect on the QOL domains. Including community participation results into the regression model in the second step did not allow any significant predictions to be made regarding the QOL domains. We speculate that this finding might be related to the cultural sensitivity of CHART S-F in the Chinese context.
Discussion
This study used the same cohort as our previous study [12]. That study focused on the prevalence of the five psychological outcomes (resilience, PTG, PTSD, anxiety, and depression) and relationships between them [12]. In this study, we mainly examined QOL of people with SCI and the predictors for QOL.
In comparison to previous studies, people with SCI in our sample had a higher QOL than those with SCI who survived the Tang-shan earthquake [14] and a Taiwanese sample of people with SCI [15]. However, they reported a lower QOL than the healthy population in Mainland China [10], and people with SCI in some developed countries and in one African country [3, 16]. These comparisons are limited to studies that used the WHOQOL-BREF. Several possible reasons could explain this difference in different samples.
Firstly, most individuals with SCI come from low-income and low-education groups in China. They are house-bound, unemployed, and living in poverty. In this sample, 83% of participants had a lower education level than high school. Only 10% of participants were in paid employment. Secondly, medical care for individuals with SCI focuses on emergency life-saving measures and ongoing physical problems. As a result, people’s psychological health and subsequent rehabilitation are neglected. We theorize these reasons lead to the low QOL of this group [12]. Additionally, three cross-cultural comparative studies of WHOQOL-BREF showed that under the same background, higher life satisfaction scores were found in Western countries [17,18,19]. The lower QOL scores from the Chinese background (both mainland China and Taiwan) cannot exclude the effect of cultural differences.
Consistent with the previous study, our findings indicated gender and age at injury correlated with QOL [20]. This means that female or younger individuals had better QOL scores. Weak correlation was observed between duration since injury and the psychological domain of QOL. Through further analysis, we found participants who were within their second or third year post injury had lower scores in psychological, social, and environmental domains than the other three groups of duration since injury. We posit that individuals with SCI are more likely to require both psychological and social rehabilitation at this stage. Reported environmental barriers was negatively related with various QOL domains and was a significant predictor of negative outcomes in the physical, psychological, and environmental QOL domains in the regression analysis. This finding is in agreement with a prior study which indicated that the negative trauma-related self-appraisals were related to poor QOL scores [21].
As we hypothesized, two positive psychological variables were positively correlated with four QOL domains. The regression analyses revealed that resilience was a statistically positive predictor of all domains of QOL. PTG had positive predictive effects on the psychological and social health QOL domains. This confirmed the adaptive value of resilience and PTG for people with SCI as seen in previous studies [22, 23]. The findings provide new evidence suggesting that focusing on positive psychological interventions may greatly change the physical, psychological, and social well-being of individuals with SCI.
PTSD, anxiety, and depression were observed to be strongly negative correlations with the four domains of QOL. They also had a strong correlation with the QOL domains in the regression analysis. Anxiety was a significantly negative predictor of physical health, psychological health, and social domains. PTSD had significantly predictive effects on physical and psychological domains of QOL. Depression just showed a significantly predictive effect on the psychological health. It seems that early screening and intervention for anxiety and PTSD are essential measures to improve the QOL of individual with SCI.
A meta-analysis study concluded that societal participation had a robust and consistent relationship with QOL [24]. The findings showed community participation of individuals with SCI was not satisfactory. Only the score of physical independence was similar to that of developed countries (81.98 vs. 78.92). However, the scores of mobility (47.87 vs. 87.30), occupation (30.06 vs. 66.26), and social integration (70.77 vs. 89.91) were significantly lower than those of developed countries [25]. We theorize that the low availability of barrier-free facilities and lack of adequate rehabilitation training are the key factors that hinder integration into society and employment for the people with SCI. Correlation analyses highlighted a significant relationship between community participation and QOL. Contrary to our expectations, the regression model did not highlight a significantly predictive effect of community participation factors on QOL. We speculate that this finding might be related to the cultural sensitivity of CHART S-F. We used the Chinese translation of this scale, but took no further steps to culturally adjust the questions. Therefore, participants from a Chinese cultural background may have different understandings of community participation than those living in Western cultures. This may have skewed the results.
Community participation of individuals with SCI in China is poor. In recent years, the Chinese government has adopted a series of measures to promote community participation of individuals with SCI, which include improving accessibility and providing vocational training.
Limitations of this study must be noted. Firstly, recruitment of the sample was from only one rehabilitation center of Shanghai. Shanghai is the most developed city in China and has the best medical and rehabilitation conditions. People with SCI living in other cities may have worse QOL than the current sample because of their less satisfactory medical conditions. Applying the results to a larger population will require caution due to representativeness issues in the study group. Secondly, we limited the scope to exploring the effects of the sociodemographic and injury factors, psychological variables, and community participation on QOL. Future studies should consider comprehensive data collection including environmental and personal factors to enhance the explanation of QOL after SCI.
Conclusion
The QOL of people with SCI in Mainland China needs improvement. Many factors were related to the four QOL domains. Only the self-reported environmental barriers and the five psychological variables were found to affect one or more domains of QOL. Therefore, promoting mental health in individuals with SCI is critical to improving overall QOL. Community participation had no effect on any domains of QOL. Perhaps people have a different understanding of community participation in the Chinese cultural background. A community participation scale which is appropriate to the Chinese cultural setting should be developed in the future study.
Data archiving
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Post M, Noreau L. Quality of life after spinal cord injury. J Neurol Phys Ther. 2005;29:139–46.
Feng Y, Zhang H, Li Y. Treatment of spinal cord Injury. J Chin Neurosurg Res. 2008;7:279–80.
Geyh S, Ballert C, Sinnott A, Charlifue S, Catz A, D’Andrea Greve JM, et al. Quality of life after spinal cord injury: a comparison across six countries. Spinal Cord. 2013;51:322–6.
Glennie RA, Batke J, Fallah N, Cheng CL, Rivers CS, Noonan VK, et al. Rural and urban living in persons with spinal cord injury and comparing environmental barriers, their health, and quality-of-life outcomes. J Neurotrauma. 2017;34:2877–82.
Barker RN, Kendall MD, Amsters DI, Pershouse KJ, Haines TP, Kuipers P. The relationship between quality of life and disability across the lifespan for people with spinal cord injury. Spinal Cord. 2009;47:149–55.
Skevington SM. Advancing cross-cultural research on quality of life: Observations drawn from the WHOQOL development. Qual Life Res. 2002;11:135–44.
Organization. WH. WHOQOL-BREF: introduction, administration, scoring and generic version of the assessment. http://www.whoint/mental_health/media/en/76pdf. 1996.
Tate D, Martin F. Review of cross-cultural issues related to quality of life after spinal cord injury. Top Spinal Cord Inj Rehabil. 2014;20:181–90.
Barclay L, McDonald R, Lentin P. Social and community participation following spinal cord injury: a critical review. Int J Rehabil Res. 2015;38:1–19.
Byrnes MBJ, Ray P, Mclenna R, Ker J. Patientfocused goal planning process and outcome after spinal cord injury rehabilitation: quantitative and qualitative audit. Clin Rehabil. 2012;26:1141–9.
Fang J. Measurement and application of quality of life. Peking. Peking University Medical Press; 2000.
Wang Y, Xie H, Zhao X. Psychological morbidities and positive psychological outcomes in people with traumatic spinal cord injury in Mainland China. Spinal Cord. 2018;56:704–11.
Hall KM, Dijker M, Whiteneck G, Brooks CA, Stuart Krause J. TheCraig Handicap Assessment and Reporting Technique (CHART): metric properties and scoring. Top Spinal Cord Inj Rehabil. 1998;4:16–30.
Chang F, Wang Y, Jang Y. Factors associated with quality of life among people with spinal cord injury: application of the International Classification of Functioning, Disability and Health model. Arch Phys Med Rehabil. 2012;93:2264–70.
Badenhorst M, Brown JC, Lambert MI, Van Mechelen W, Verhagen E. Quality of life among individuals with rugby-related spinal cord injuries in South Africa: a descriptive cross-sectional study. BMJ Open. 2018;8:e020890–e.
de Franca ISX, Coura AS, de Franca EG, Basilio NNV, Souto RQ. Quality of life of adults with spinal cord injury: a study using the WHOQOL-bref. Rev Esc Enferm Usp. 2011;45:1361–8.
Ide M, Fugl-Meyer AR. Life satisfaction in persons with spinal cord injury: a comparative investigation between Sweden and Japan. Spinal Cord. 2001;39:387–93.
Songhuai L, Olver L, Jianjun L, Kennedy P, Genlin L, Duff J, et al. A comparative review of life satisfaction, quality of life and mood between Chinese and British people with tetraplegia. Spinal Cord. 2009;47:82–6.
Hampton NZ, Marshall A. Culture, gender, self-efficacy, and life satisfaction: a comparison between Americans and Chinese people with spinal cord injuries. J Rehabil. 2000;66:21–8.
Rivers CS, Fallah N, Noonan VK, Whitehurst DG, Schwartz CE, Finkelstein JA, et al. Health conditions: effect on function, health-related quality of life, and life satisfaction after traumatic spinal cord injury. A Prospective Observational Registry Cohort Study. Arch Phys Med Rehabil. 2018;99:443–51.
Schonenberg M, Reimitz M, Jusyte A, Maier D, Badke A, Hautzinger M. Depression, posttraumatic stress, and risk factors following spinal cord injury. Int J Behav Med. 2014;21:169–76.
Wang Y, Xie H, Zhao X. Psychological morbidities and positive psychological outcomes in people with traumatic spinal cord injury in Mainland China. Spinal Cord. 2018;56:704–11.
Tansey TN, Bezyak J, Kaya C, Ditchman N, Catalano D. Resilience and quality of life: an investigation of Kumpfer’s resilience model with persons with spinal cord injuries. Rehabil Couns Bull. 2017;60:163–74.
Dijkers M. Quality of life after spinal cord injury: a metaanalysis of the effects of disablement components. Spinal Cord. 1997;35:829–40.
Kennedy P, Lude P, Taylor N. Quality of life, social participation, appraisals and coping post spinal cord injury: a review of four community samples. Spinal Cord. 2006;44:95–105.
Acknowledgements
We thank all persons who participated in this study and the Shanghai Sunshine Hospital.
Funding
This work was supported by the project of the Shanghai Disabled Person’s Federation (K2016027) and the Outstanding Clinical Discipline Project of Shanghai Pudong (PWYgy2018-10).
Author contributions
YBW was responsible for designing the study, conducting the study, analyzing the data, writing the article, and submitting the article. XDZ were responsible for designing the study, conducting the study, analyzing the data, and writing the paper. HXX was responsible for collecting the data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, Y., Zhao, X. & Xie, H. Quality of life and its predictors in people with traumatic spinal cord injury in mainland China. Spinal Cord 57, 739–746 (2019). https://doi.org/10.1038/s41393-019-0279-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-019-0279-z
This article is cited by
-
Sex, age, role and geographic differences in traumatic spinal fractures caused by motor vehicle collisions: a multicentre retrospective study
Scientific Reports (2023)
-
Sexuality After Spinal Cord Injury. Which Factors Influence Sexual Activity and Satisfaction?
Sexuality and Disability (2022)
-
Self-care in spinal cord injuries inventory (SC-SCII) and self-care self-efficacy scale in spinal cord injuries (SCSES-SCI): development and psychometric properties
Spinal Cord (2021)
-
Long non-coding RNA Mirt2 relieves lipopolysaccharide-induced injury in PC12 cells by suppressing miR-429
Journal of Physiology and Biochemistry (2019)
