
Abstract
Objective
To evaluate the utility of a standardized physical exam score (PE-NEC) in predicting need for surgery or death in neonates with necrotizing enterocolitis (NEC).
Methods
This prospective, multicenter, observational study was conducted from 3/1/14 to 2/29/16 with three regional perinatal centers in upstate New York. Infants with NEC Bell’s Stage ≥ 2 had physical exams and laboratory data recorded at 12–24 h intervals for 48 h following diagnosis. PE-NEC score was comprised of seven components: bowel sounds, capillary refill time, abdominal wall erythema, girth, discoloration, induration, and tenderness. Surgical timing was determined by surgeons blinded to the PE-NEC score. Optimal sensitivity and specificity of PE-NEC score for surgery/death (primary outcome) was determined by receiver operating characteristic curve analysis.
Results
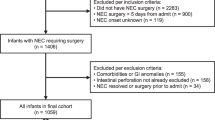
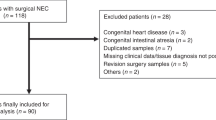
Of 100 infants with NEC, 5 had pneumoperitoneum at diagnosis and were excluded yielding 95 for analyses. Of those, 35 infants experienced the primary outcome: 3 died from NEC prior to surgery and 32 had surgery (30 laparotomies, 2 drains). The PE-NEC score was found to be sensitive and specific for need for surgery/death (AUC = 0.89, 95% CI 0.82–0.97); a score of ≥3 had a sensitivity of 0.88 (95% CI 0.72–0.97), specificity of 0.81 (95% CI 0.69–0.90). All components of the PE-NEC score were more likely to be present among infants with surgical NEC or who died.
Conclusion
PE-NEC score is sensitive and specific in predicting need for surgery in infants with NEC and should be validated as a clinical decision-making tool.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Mizrahi A, Barlow O, Berdon W, Blanc WA, Silverman WA. Necrotizing enterocolitis in premature infants. J Pediatr. 1965;66:697–705.
Neu J. Necrotizing enterocolitis: The search for a unifying pathogenic theory leading to prevention. Pediatr Clin North Am. 1996;43:409.
Uauy RD, Fanaroff AA, Korones SB, Phillips EA, Phillips JB, Wright LL. Necrotizing enterocolitis in very low birth weight infants: biodemographic and clinical correlates. National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr. 1991;119:630–8.
Stevenson DK, Wright LL, Lemons JA, Oh W, Korones SB, Papile LA, et al. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1993 through December 1994. Am J Obstet Gynecol. 1998;179:1632–9.
Flake AW. Necrotizing enterocolitis in preterm infants--is laparotomy necessary? N Engl J Med. 2006;354:2275–6.
Kosloske AM. Epidemiology of necrotizing enterocolitis. Acta Paediatr Suppl. 1994;396:2–7.
Kosloske AM. Indications for operation in necrotizing enterocolitis revisited. J Pediatr Surgery. 1994;29:663–6.
LaGamma EF, Ostertag SG, Birenbaum H. Failure of delayed oral feedings to prevent necrotizing enterocolitis. Results of study in very-low-birth-weight neonates. Am J Dis Child. 1985;139:385–9.
Lemons JA1, Bauer CR, Oh W, Korones SB, Papile LA, Stoll BJ, et al. Very low birth weight outcomes of the National Institute of Child health and human development neonatal research network, January 1995 through December 1996. NICHD Neonatal Research Network. Pediatr. 2001;107:E1.
Tepas JJ, Sharma R, Leaphart CL, Celso BG, Pieper P, Esquivia-Lee V. Timing of surgical intervention in necrotizing enterocolitis can be determined by trajectory of metabolic derangement. J Pediatr Surg. 2010;45:310–4.
Kliegman RM, Walker WA, Yolken RH. Necrotizing enterocolitis: research agenda for a disease of unknown etiology and pathogenesis. Pediatr Res. 1993;34:701.
Kliegman RM, Walsh MC. Neonatal necrotizing enterocolitis: pathogenesis, classification, and spectrum of disease. Curr Probl Pediatr. 1987;17:243–88.
Wu S, Caplan M, Lin H. Necrotizing enterocolitis: old problem with new hope. Pediatr Neonatol. 2012;53:158–63.
Gephart SM, Spitzer AR, Effken JA, Dodd E, Halpern M, McGrath JM. Discrimination of GutCheckNEC: a clinical risk index for necrotizing enterocolitis. J Perinatol. 2014;34:468–75.
Fox JR, Thacker LR, Hendricks-Munoz KD. Early detection tool of intestinal dysfunction: impact on necrotizing enterocolitis severity. Am J Perinatol. 2015;32:927–32.
Ji J, Ling X, Zhao Y, Hu Z, Zheng X, Xu Z, et al. A data-driven algorithm integrating clinical and laboratory features for the diagnosis and prognosis of necrotizing enterocolitis. PLoS ONE. 2014;9:e89860.
Shah NP, Steyerberg EW, Kent DM. Big data and predictive analysis. Recalibrating Expect JAMA. 2018;320:27–28.
Robinson JR, Rellinger EJ, Hatch LD, Weitkamp J-H, Speck KE, Danko M. Surgical necrotizing enterocolitis. Semin Perinatol. 2017;41:70–9.
Kim WY, Kim WS, Kim IO, Kwon TH, Chang W, Lee EK. Sonographic evaluation of neonates with early-stage necrotizing enterocolitis. Pediatr Radiol. 2005;35:1056–61.
Dilli D, Suna Oguz S, Erol R, Ozkan-Ulu H, Dumanli H, Dilmen U. Does abdominal sonography provide additional information over abdominal plain radiography for diagnosis of necrotizing enterocolitis in neonates? Pediatr Surg Int. 2011;27:321–7.
Hashem RH, Mansi YA, Almasah NS, Abdelghaffar S. Doppler ultrasound assessment of the splanchnic circulation in preterms with neonatal sepsis at risk for necrotizing enterocolitis. J Ultrasound. 2017;20:59–67.
Cuna AC, Reddy N, Robinson AL, Chan SS. Bowel ultrasound for predicting surgical management of necrotizing enterocolitis: a systematic review and meta-analysis. Pediatr Radiol. 2018;48:658–66.
Henry MCW, Moss RL. Neonatal necrotizing enterocolitis. Sem Ped Surgery. 2008;17:98–109.
Gordon PV, Swanson JR, Spitzer A. The complete blood cell count in a refined cohort of preterm NEC: the importance of gestational age and day of diagnosis when using the CBC to estimate mortality. J Perinatol. 2016;36:121–5.
Acknowledgements
We thank the faculties at Albany Medical Center, the University of Rochester and the University at Buffalo for their help in standardized documentation of physical examinations and Holly Wadkins, Caitlin Fallone, and Ann Marie Scorsone for assistance with data extraction.
Funding
Supported in part by the Clinical and Translational Science Award UL1 TR000445.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Khalak, R., D’Angio, C., Mathew, B. et al. Physical examination score predicts need for surgery in neonates with necrotizing enterocolitis. J Perinatol 38, 1644–1650 (2018). https://doi.org/10.1038/s41372-018-0245-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-018-0245-1
This article is cited by
-
Surgical prediction of neonatal necrotizing enterocolitis based on radiomics and clinical information
Abdominal Radiology (2024)
-
Early versus delayed enteral nutrition for neonatal hypoxic-ischemic encephalopathy undergoing therapeutic hypothermia: a randomized controlled trial
Italian Journal of Pediatrics (2022)
-
Camera-based heart rate estimation for hospitalized newborns in the presence of motion artifacts
BioMedical Engineering OnLine (2021)
