
Abstract
Objective
To find variations in Chinese obesogenic environmental priorities from 2000 to 2011, predict spatiotemporal distribution of obesity prevalence aged 7–17 years in 31 provinces, and provide foundations for policy-makers to reduce obesity in children and adolescents.
Methods
Based on data examination of provincial obesity prevalence aged 7–17 years from three rounds of China Health and Nutrition Surveys (in 9 [2000], 9 [2006], and 12 [2011] provinces) and corresponding years’ environments in 31 provinces from China Statistical Yearbooks and other sources, 12 predictors were selected. We used 30 surveyed provinces in three rounds as training samples to fit three analytic models with partial least-square regressions and prioritized predictors by variable importance projection to find variations. And fitted a spatiotemporal prediction model with Bayesian analysis to infer in space–time.
Results
Variations of obesogenic environmental priorities were found at different times. A Bayesian spatiotemporal prediction model with deviance information criterion of 155.60 and statistically significant (P < 0.05) parameter estimates of intercept (−717.0400, 95% confidence intervals [CI]: −1186.0300, −248.0480), year (0.3584, CI: 0.1245, 0.5924), square of food industry level (0.0003, CI: 0.0002, 0.0004), and log (healthcare) (5.3742, CI: 2.5138, 8.2347) was optimized. Totally inferred average obesity prevalence among children and adolescents were 2.23%, 5.11%, 10.77%, 12.20%, 13.99%, and 17.58% in 31 provinces in China in 2000, 2006, 2011, 2015, 2020, and 2030, respectively. Obesity in north and east of China clusters on predicted maps.
Conclusions
Obesity prevalence in children and adolescents in China is rapidly increasing, growing at 0.3584% annually from 2000 to 2011. From longitudinal observation, prevalence was significantly influenced by food industry (“Amplifier”) and healthcare service (“Balancer”). Targeted interventions in north and east of China are pressing. Further researches on the mechanisms underlying the influence of food industry, healthcare service, and so on in children and adolescents are needed.
Similar content being viewed by others
Introduction
The prevalence of obesity in children and adolescents has increased substantially over the past three or four decades in developed and developing countries [1, 2], including China [3,4,5,6,7,8]. This implies greater reductions in quality of life, greater risk of social isolation, and greater economic disease burden [3, 9]. However, since it is predictable, preventable, controllable, and reversible [10], the need for preventive action is increasingly being recognized.
Obesity is partly determined by genetic susceptibility, but obesogenic environments are necessary for its phenotypic expression [11]. In industrialized societies, the imbalance between health literacy and rapid food industry, marketing media, and transportation modernization, promotes higher energy-density intakes and sedentary behaviors [12, 13]. Given the complexity of obesity in children and adolescents, policy-decision processes should be more systematic, evidence-based, locally relevant, and stakeholder-informed, for more cohesive and comprehensive actions; but are often nonsystematic in practice. In recent years, Analysis Grid for Environments Linked to Obesity (ANGELO) framework was used in Europe by policy-makers at the national level to prioritize strategies for effective food and nutrition initiatives [3, 14]. Swinburn et al. suggested this 2 × 4-grid analysis framework to dissect the environments into two levels, micro and macro, using four dimensions: physical, economic, political, and sociocultural. In this framework, environmental factors influencing food intake and physical activities were characterized as “obesogenic” or “leptogenic” (promoting leanness) [15]. Research on obesogenic environments can help systematically and locally to determine and identify priority areas for population-based prevention of childhood obesity [3]. We need to develop systematic and integrated approaches to facilitate complementary and coordinated actions by various concerned parties, including governments, international organizations, civil society, and corporations [11, 12].
With rapid industrialization, urbanization, and unbalanced economic development, in the background of complex terrain, distributions of obesity prevalence throughout China are heterogeneous in time–space. Wang et al. found regional differences in the prevalence of obesity among 7–18-year-old Chinese children in 2014 [8]. Contrariwise, obesity was shown as closely related to geographic and natural environments [16], economic activity, dietary patterns, food production, transportation, social culture, policies, and regulations [17, 18]. Often, these factors are internally consistent within each of the Chinese provinces. Fighting obesity requires detailed global, national, provincial, and community-level pictures of the problem, especially its severity, size, distribution, and the underlying determinants. Few systematic studies have focused on the relationships between macro-environmental factors and obesity prevalence in Chinese children and adolescents at the provincial level. There are perhaps some difficulties, including lack of complete data and suitable methods. Geographic information system (GIS) is increasingly used in thematic mapping and spatiotemporal epidemiology analysis of obesity and other public health problems [19, 20].
In this study, we collected obesity data for children and adolescents aged 7–17 years from three rounds of China Health and Nutrition Surveys (CHNS), and corresponding years’ environmental data at provincial level from China’s Statistical Yearbooks and other sources. After scanning these data, we selected 12 predictors and constructed analytic models with partial least-square regression (PLSR) and a predictive model with Bayesian analysis, which have been successfully used in medical fields to address small sample cases [21,22,23,24]. Furthermore, obesogenic environmental factors were prioritized for research and intervention, while thematic maps of obesity in 2000, 2006, 2011, 2015, 2020, and 2030 among children and adolescents in 31 Chinese provinces were inferred.
Materials and methods
Study design, samples, and key variables
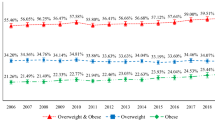
We used data from three rounds of CHNS; 9 provinces (Liaoning, Heilongjiang, Jiangsu, Shandong, Henan, Hubei, Hunan, Guangxi, and Guizhou) were surveyed in 2000 and again in 2006, then 12 provinces (with Beijing, Shanghai, and Chongqing, in addition to the previous nine provinces) in 2011. A multistage, stratified, random cluster sampling design was used throughout, to ensure a suitable representation of the population [25, 26]. Specialized and standardized trainings were adopted in advance and data on health, nutrition, and socioeconomic variables at the community, household, and individual levels were collected using questionnaires, dietary surveys, and physical measurements in September (autumn) every round. The institutional review boards of the University of North Carolina at Chapel Hill and the National Institute for Nutrition and Health at the Chinese Center for Disease Control and Prevention approved the survey protocols. All subjects completed written informed consent. Further details are provided in the published profile of this cohort study [25, 26]. We used the data of children and adolescents aged 7–17 with complete height and weight records to assess obesity prevalence at province level in the corresponding age range; those without height or weight data were excluded from analysis. The final sample included 4803 participants with 2249, 1138, and 1416 participants in 2000, 2006, and 2011 surveys, respectively. The proportions of male, urban, 7–11 years old, and total observed obesity prevalence were 53.13%, 23.83%, 41.80%, and 2.45% in 2000 (nine provinces); 52.99%, 26.54%, 49.21%, and 3.51% in 2006 (nine provinces); and 50.71%, 40.40%, 54.38%, and 9.11% in 2011 (12 provinces), respectively. Height was measured without shoes to the nearest 0.1 cm using portable Seca 206 wall-mounted metal tapes (Seca Ltd., Birmingham, UK), while weight was measured without shoes and in light clothing to the nearest 0.1 kg on calibrated Seca 880 beam scales. Body mass index (BMI), the key outcome variable, was defined according to the Body Mass Index Reference Norm for Screening Overweight and Obesity in Chinese Children and Adolescents (aged 7–18 years) [27] developed in 2004 by the Working Group on Obesity in China, organized by the International Life Science Institute Focal Point in China [27]. Relative to sex and age, the definition of obesity, BMI > 95th percentile, has been applied extensively in recent years in China [27].
The dimensionalities of obesogenic environmental factors were determined by interviewing experts and reviewing literatures. Relevant environmental data, at provincial levels, were found in China Statistical Yearbooks [28,29,30], China Health Statistics Yearbooks [31,32,33], China Education Yearbooks [34,35,36], China Light Industry Yearbooks [37, 38], China Food Industry Yearbooks [39], the Sixth National Population Census of the People’s Republic of China in 2010 [40], China Electric Power Yearbooks, and other sources, for the corresponding years. We collected data on food consumption, including grains, meat, poultry, vegetables, edible oil, sugar, and dietary behaviors (dining out). We used the provincial annual production of dairy and soft drinks as representative variables for the developmental level of modern food industry. We checked environmental hygiene indicators, such as modified water sources, tap water, and lavatories. We examined economic indicators, including provincial gross domestic product (GDP), GDP per capita, and average incomes. We considered some demographic indicators, including sex ratio, child dependency ratio, urban–rural ratio, and urban population density. Other indicators considered were media and marketing (television coverage), transportation capacity, use of washing machine, healthcare service, mother’s illiteracy rate, sports facilities, built environments (per capita public green space and paved road area, etc.), sedentary life, and school policy scores. From 45 variables of 13 dimensionalities collected and examined, 12 environmental predictors of 11 dimensionalities were selected and analyzed. We did not analyze the data of Hong Kong, Macao, and Taiwan.
Statistical analysis
In the form of descriptive statistical analysis, tables, and maps, we showed the distributions and variabilities of obesity prevalence and the environmental predictors in time and space at provincial level among children and adolescents aged 7–17 years.
Compared with principal component analysis, use of PLSR (originally proposed by the econometrician Herman Wold in the 1960s) is more flexible and extensive, especially in medicine [21, 22, 41, 42]. PLSR integrates linear regression, principal component analysis, and canonical correlation analysis to handle multiple colinear and small sample data, and is even applicable when the sample size is smaller than the number of independent variables with a stable regression. PLSR can use Variable Importance in Projection (VIP) for variable screening and priority ordering conveniently [43,44,45].
First, we examined correlations among independent variables (environmental factors) by dimensionality. Second, we used independent variables by dimensionality and the dependent variable (observed obesity prevalence among adolescents and children at province level) as training samples to test for linearity, independence, normality, and equal variance; and to perform the single factor linear regressions. Twelve independent variables (as environmental predictors) of 11 dimensionalities, which were eligible for the simple linear regression with statistical significance (P < 0.1), or supported by expert opinions or literatures, were selected. Third, using three rounds of survey as three cross-sectional datasets, we fitted three analytic models with PLSR separately: Y = β0 + β1X1 + β2X2 + … + βkXk + ε, in which the dependent variable Y was provincial obesity prevalence and the independent variables X1,X2,…Xk were the 12 environmental predictors we have just selected. We derived three groups of prioritizations of obesity environmental predictors by VIPs.
The analytic PLSR models can explain the observed samples well, but it cannot predict unobserved samples accurately because of overfitting. In addition, a PLSR model cannot give 95% CI of parameter estimates. Bayesian analysis provides robust predictions and inferences that are conditional on the data, without reliance on asymptotic approximation, while treating parameters as unknown random variables and making inferences based on the posterior distributions of the parameters. Moreover, small sample inference proceeds in the same manner as if one had a large sample. It can also estimate any function of parameters directly, without using the “plug-in” method and provide interpretable answers with 95% CI and a model assessment tool of deviance information criterion.
Fourth, based on analysis of the variations of obesogenic environmental priorities in three different rounds, we included all 30 provincial-level observations in three survey rounds as a training sample to optimize a space–time predictive model with fewer independent variables by Bayesian analysis. And predicted obesity prevalence for the provinces and for the years not surveyed, as well as a profile of obesity prevalence in 31 provinces in China in 2000, 2006, 2011, 2015, 2020, and 2030. The posterior distribution of the model parameters was estimated using Markov chain Monte Carlo simulations. By defaults in SAS, PROC GENMOD computes three convergence diagnostics: the lag1, lag5, lag10, and lag50 autocorrelations; Geweke diagnostic statistics; and effective sample sizes. We have 95% confidence to say that the intervals contain the overall parameter estimates with statistical significance.
Fifth, in the Sixth National Population Census of the People’s Republic of China in 2010, we took the children and adolescent proportions as weights, these were the corresponding populations in each of the 31 provinces accounting for the total corresponding population of 31 provinces of China. We calculated the total inferred average prevalence of obesity among the children and adolescents in the 31 provinces.
Sixth, we made six thematic maps of predicted obesity prevalence among children and adolescents in 31 provinces. We used SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and ArcGIS Desktop 10.3 (Environmental System Research Institute, ESRI) throughout the process.
Finally, we compared the inferred 2015 obesity prevalence with the newest CHNS 2015 round result on the children and adolescents’ obesity prevalence in 15 provinces of China (Shaanxi, Yunnan, and Zhejiang in addition to the 12 provinces surveyed in 2011).
Results
Distributions and variations for selected independent and dependent variables in 2000, 2006, and 2011
Table 1 shows the descriptive analysis (minimum, median, maximum, mean, and standard deviation) for selected variables and the number of provinces reported for.
Distribution and variations in observed obesity prevalence and environmental predictors by provinces in 2000, 2006, and 2011
Figure 1 is a group of maps showing the distribution and variations in the observed obesity prevalence and environmental predictors by provinces.

Distribution and variations in the observed obesity prevalence and environmental predictors by province in 2000, 2006, and 2011. Note: From A to L, 12 obesogenic environmental predictors are food industry level (in 10,000 tons), transport capability (in 100 million ton-km), edible oil per capita (g), provincial GDP (in 100 million yuan), modified water source ratio (%), school policy score (point), children dependency ratio (%), media (television coverage in %), washing machine (in units per 100 households), vegetables per capita (g), healthcare service (in doctors/1000 persons), and mother’s illiteracy rate (%)
Analytic model
We developed parameter estimates, prioritizations of environmental obesity factors (Table 2) and found two environmental factor types. Obesity-promoting factors include edible oil per capita, food industry level, modified water source ratio, provincial GDP, washing machines, media (television coverage), transportation capability, and healthcare service, while obesity-impeding factors include child dependency ratio, mother’s illiteracy rate, vegetables per capita, and school policy score. In 2006 and 2011 rounds, the dimensionalities and the direction of the impact of these two factor types on obesity remained consistent. However, in 2000, four predictors (edible oil per capita, washing machines, mother’s illiteracy rate, and school policy score) showed inverse directions of the impact on obesity compared with its following two rounds (2006 and 2011).
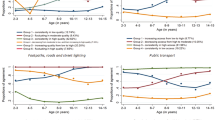
In the cross-sectional three rounds of data, we found variations in Chinese obesogenic environmental priorities at provincial level (Fig. 2). In descending order of VIPs, the most important four factors of children obesity, respectively, were transportation capability, school policy score, provincial GDP, and modified water source ratio in 2000; transportation capability, provincial GDP, food industry level, and vegetables per capita in 2006; and edible oil per capita, food industry level, modified water source ratio, and provincial GDP in 2011.

Variations of Chinese obesogenic environmental priorities at provincial level in 2000, 2006, and 2011
In the three different survey years, predictors of continuously increasing importance were edible oil per capita, children dependency ratio, food industry level, media, washing machines, mother’s illiteracy rate, healthcare service; the predictor of continuously decreasing importance was transportation capability. Predictors lacking a steady trend were provincial GDP, vegetables per capita, school policy score, and modified water source ratio.
Optimization of the Bayesian space–time predictive model and the spatiotemporal inference
Using all observed 30 provincial-level observations in the three rounds as a training sample, we fitted a Bayesian space–time predictive model with a deviance information criterion of 155.60 and with statistically significant parameter estimates (P<0.05) (Table 3). In the posterior distribution test results, no obvious internal correlations among samples and Markov chain Monte Carlo simulations converged rapidly. From longitudinal observation, the prevalence of obesity among children and adolescents increased by 0.3584% annually on average between 2000 and 2011, and was more influenced by the food industry level and healthcare service. The predictive model yielded spatiotemporal inferences on obesity prevalence distributions in the 31 provinces of China in 2000, 2006, 2011, 2015, 2020, and 2030; and inferences in 2015, 2020, and 2030 were based on the obesogenic environmental data of 2011.
Totally inferred average prevalence of obesity in the 31 provinces of China
The inferred total average obesity prevalence in all 31 provinces were 2.23%, 5.11%, 10.77%, 12.20%, 13.99%, and 17.58% in 2000, 2006, 2011, 2015, 2020, and 2030, respectively.
Thematic maps predicted
Obesity in children and adolescents showed a continuously increasing trend, and obesity in northern and eastern provinces of China was clustered in the predicted maps. In 2000, there were only three provinces with the highest obesity levels, from 5 to 10%. In 2006, three provinces had a level above 10% and one above 15%. In 2011, nine provinces had a level above 10% and four above 15%. In 2015, 14 provinces had a level above 10% and 4 above 15%. In 2020, 20 and 6 provinces would have a level above 10 and 15%, respectively. In 2030, all 31 provinces would have a level above 10% while 15 above 15% (Fig. 3).

Predicted thematic maps of obesity prevalence aged 7–17 in 2000, 2006, 2011, 2015, 2020, and 2030 in 31 provinces of China. Note: We did not analyze the data of Hong Kong, Macao, and Taiwan in this study
Comparison between predicted and newly observed results in CHNS 2015 round
Using the newly observed obesity prevalence among children and adolescents in CHNS 2015 round in 15 provinces, we compared them with their counterparts inferred and found that these two results were almost consistent across regional trends, in provinces on obesity prevalence near or above 10% and in clustering of obesity in the north (Beijing, Liaoning, Heilongjiang, and Shaanxi) and east (Shandong, Shanghai, and Jiangsu) of China (Supplementary Figure 1).
Discussion
In three rounds of surveys, priorities had changed. During the last 10 years, the influence of these seven factors (edible oil, children dependency ratio, food industry level, media, washing machines, mother’s illiteracy rate, and healthcare service) was continuously increasing. According to the predictive model fitted, we found the following quantitative relations. The prevalence of obesity among children and adolescents increased by 0.3584% annually on average from 2000 to 2011 and was more influenced by food industry level and healthcare service. Food industry level seems to be an “Amplifier” of childhood obesity, with “1” being the critical value, which actually means when the development level of the food industry reaches or exceeds the scale of 10,000 tons of milk products per year in a province the “Amplifier” can accelerate prevalence of obesity more quickly in the form of square of food industry level. Healthcare service level seems to be a “Balancer” of childhood obesity, with “1” being the critical value, which actually means when the number of doctors per 1000 persons is less than 1 or more than 1, healthcare service level shows a negative or positive effect on the nutritional status of the population in the form of a logarithmic relationship. From a qualitative perspective, whether healthcare practitioners focus on “disease treatment” or “nutrition and health integrity” may fundamentally determine the direction, nature, and future trends of the role of healthcare in the obesity epidemic. Hence, we can term it a “Balancer.” The inferred total average obesity prevalence in 31 provinces of China were 2.23%, 5.11%, 10.77%, 12.20%, 13.99%, and 17.58% in 2000, 2006, 2011, 2015, 2020, and 2030, respectively. Compared with the newly observed CHNS 2015 data in the 15 provinces, predictive results of 2015 were consistent with the observed results, in provinces with obesity rates near or above 10% and in the clustering trend of obesity in the north and east of China. We need to understand major contradictions timeously and identify modifiable determinants to control and reverse the epidemic of obesity.
The food industry level combined with media and transportation capacity forms a powerful engine to promote consumption of processed foods and snacks [15, 46, 47]. In this study, food industry level was a positive correlation factor in the three rounds with continuously increasing importance. Modern food industry provides abundant inexpensive food, increases the accessibility to food, and plays important roles in reducing protein energy malnutrition. However, with sustained economic growth, increased purchasing power, and decreased physical activity; the excessive oil, salt, and sugar in processed foods, snacks, and beverage contribute to obesity in children and adults [15, 46]. Food marketing and advert directed at children are extensive, widespread, and global; and are focused on fast food, processed food, snacks, and beverages. Evidences also imply that television marketing influences children’s food preference, requests, and purchase behaviors. The World Health Organization has provided suggestions in a framework for implementing a set of recommendations on the marketing of foods and nonalcoholic beverages to children (2012), to promote responsible marketing. In our study, media, transportation capability (which determines the access to foods especially during eras or in regions of food shortages), and healthcare service were positive correlation factors in the three rounds with continuously increasing importance [46].
However, healthcare service not only helps improve residents’ nutritional status but can also help to prevent obesity [48]. Efforts should be directed at setting nutritional guidelines to educate doctors on how to prevent diet-related chronic non-communicable diseases, and not just to treat the resulting diseases only.
We also found other positive correlations, such as provincial GDP, modified water sources, edible oil, and washing machine use. The studies by Popkin et al. found that when income increases, households from the lower-income strata tend to add more oil and sugar to diets that are already high in energy density [49]. Su et al., based on the 1997–2009 Chinese data on children and adolescents found that the percentage of energy intake from fat was positively related to overweight and obesity (odds ratio = 1.01; 95% CI 1.00, 1.02; P = 0.006) [50]. Another study found that by 2009, 57.0% of children and adolescents aged 7–17 years consumed over 30.0% of their energy from fat, which is the upper limit recommended in Chinese Dietary Reference Intakes [51]. In our study, the importance of edible oil in three rounds was continuously increasing.
We also found negative correlations between obesity in children and the provincial children dependency ratio, mother’s illiteracy rate, school policy score, and consumption of vegetables. Children dependency ratio reflects the allocation of resources, fertility rate, work participation rate, and change in the amount of housework undertaken [52, 53]. We believe that maintaining a moderately higher fertility rate might lower the obesity prevalence in children. Further research is needed. Mother’s illiteracy rate may affect the availability of food in households and mothers’ practices in feeding children [54]. We consider that the negative effect of mother’s illiteracy rate may be an indirect reflection of the phenomenon that mothers’ high employment rate promotes children’s obesity [55]. The school policy in our study showed a moderately antagonistic effect on child obesity. Children and adolescents are in the key period of knowledge learning, cognitive formation, and eating habits shaping. Education on nutrition, health, and activities will play a positive role, and may also have long-term effects on their offspring [3, 56, 57].
Wang et al. in 2017, analyzed obesity data from the Chinese National Survey on Students Constitution and Health among those aged 7–18 years and found regional differences in the prevalence of overweight and obesity. The occurrence of obesity in northern and eastern provinces of China shows obvious clustering. The spatial distribution trend found in our study was consistent with that of the authors [8].
In this study, the annual increase in the rate of obesity prevalence among Chinese children and adolescents ranged from 0.12 to 0.59% from 2000 to 2011. This was close to Wang et al.’s results of the students’ physical examination, in which the annual increase in the rate of obesity ranged from 0.10 to 0.58% among students aged 7–18 years from 1985 to 2014 [8].
Overall, the association between childhood and adolescent obesity and food industry level and healthcare service was statistically significant. We should create supportive environments for healthier food choice via continuous systematic research on how the imbalance is formed and how it can be reversed, and by education and the establishment of regulations on food labeling.
Although the data were limited, we adopted PLSR and Bayesian analysis, which was suitable for modeling with small size sample, and still fitted a stable space–time predictive model. Moreover, as the forecasts for 2015, 2020, and 2030 were based on 2011 environmental data, such predictions may be conservative or underestimated in the context of the overall social developments. In the future, more detailed data should be obtained through routine monitoring to verify the results of this study. Furthermore, “individual–community–province” hierarchical or random-effect models will be adopted in our next research, which can deal with the problem of temporal or spatiotemporal misalignment better and to explore the influencing mechanism and changing rules in obesogenic environments more precisely and clearly. The effects and mechanism of school policy, children dependency ratio, and parents’ educational situation on children obesity also need further explorations.
In summary, there have been obvious changes in obesogenic environmental priorities during the different rounds. Obesity prevalence in children and adolescents aged 7–17 years in China experienced a rapid increase, at about 0.3584% annually between 2000 and 2011. From longitudinal observation, the associations between food industry level (“Amplifier”), healthcare service (“Balancer”), and children and adolescents’ obesity prevalence were statistically significant. Targeted interventions in northern and eastern provinces of China are necessary and urgent. Further research on the mechanisms of how the levels of food industry, healthcare service, and other environmental factors influence the prevalence of obesity is needed. We need to understand the major contradictions timeously and identify modifiable determinants to control and reverse the epidemic of obesity and to achieve enduring health outcomes. Given the complexity of problems, concerted efforts are needed to promote innovation. There should be supply-side reforms in the food industry, healthcare, and educational systems (primary schools, middle schools, medical colleges, and food industry colleges) to support the new generations on how to understand food, nutrition, and activities; and how to produce, select, and consume healthier food.
References
Abarca-Gómez L, Abdeen ZA, Hamid ZA, Dika Z, Ivkovic V, Jelakovic A, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 2017;390:2627–42.
WHO. Consideration of the Evidence on Childhood Obesity for the Commission on Ending Childhood Obesity: Report of the Ad hoc Working Group on Science and Evidence for Ending Childhood Obesity. Geneva, Switzerland: World Health Organization Press; 2016.
WHO. Prioritizing Areas for Action in the Field of Population-based Prevention of ChildhoodObesity: a Set of Tools for Member States to Determine and Identify Priority Areas for Action. Geneva, Switzerland: World Health Organization Press. .
Wang H, Xue H, Du S, Zhang J, Wang Y, Zhang B. Time trends and factors in body mass index and obesity among children in China: 1997-2011. Int J Obes. 2017;41:964–70.
Zhang J, Wang H, Wang Y, Xue H, Wang Z, Du W, et al. Dietary patterns and their associations with childhood obesity in China. Br J Nutr. 2015;113:1978–84.
Jia Peng, Xue Hong, Zhang Ji, Wang Youfa. Time trend and demographic and geographic disparities in childhood obesity prevalence in China—evidence from twenty years of longitudinal data. Int J Environ Res Public Health. 2017;14:1–9.
NHFPC. Report on Chinese Residents’ Chronic Diseases and Nutrition. Beijing, China: People’s Medical Publishing House; 2015.
Wang S, Dong YH, Wang ZH, Zou ZY, Ma J. [Trends in overweight and obesity among Chinese children of 7-18 years old during 1985-2014]. Zhonghua yu Fang yi xue za zhi [Chin J Prev Med]. 2017;51:300–5.
Wang YC, Mcpherson K, Marsh T, Gortmaker SL, Brown M. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet. 2011;378:815–25.
Blackburn GL, Waltman BA. Expanding the limits of treatment-new strategic initiatives. J Am Diet Assoc. 2005;105:S131–S135.
Loos RJF, Rankinen T. Gene-diet interactions on body weight changes. J Am Diet Assoc. 2005;105:S29–S34.
Gortmaker SL, Swinburn BA, Levy D, Carter R, Mabry PL, Finegood DT, et al. Changing the future of obesity: science, policy, and action. Lancet. 2011;378:838–47.
Carmona RH. Improving health literacy: preventing obesity with education. J Am Diet Assoc. 2005;105:S9–S10.
Robertson A, Tirado C, Lobstein T, Jermini M, Knai C, Jensen JH, et al.. Food and Health in Europe: a New Basis for Action. Copenhagen, Denmark: WHO Regional Office for Europe; 2004.
Swinburn B. Dissecting obesogenic environments: the development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev Med. 1999;29:563–70.
Von HP, Benson R. Obesity and the natural environment across US counties. Am J Public Health. 2014;104:1287–93.
Amine E, Belhadj M, Deurenbergyap M, Forrester T, Baba N, Djazayery A. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint FAO/WHO Expert Consultation. Geneva, Switzerland: World Health Organization Press; 2003.
Jeor STS. The complexities of obesity. J Am Diet Assoc. 2005;105:S11–S12.
Jia P, Cheng X, Xue H, Wang Y. Applications of geographic information systems (GIS) data and methods in obesity‐related research. Obes Rev. 2017;18:1–12.
Wilson A, Kingham S, Campbell M, Beere P. Using GIS to assess the impact of childhood environments on obesity. CMAJ. 2015;6:706–12.
Krishnan A, Williams LJ, Mcintosh AR, Abdi H. Partial least squares (PLS) methods for neuroimaging: a tutorial and review. Neuroimage. 2011;56:455–75.
Mehmood T. Mining for genotype-phenotype relations in Saccharomyces using partial least squares. BMC Bioinforma. 2011;12:318–30.
Li J, Jin M, Zheng X. Spatiotemporal variability of remotely sensed PM2.5 concentrations in China from 1998 to 2014 based on a Bayesian hierarchy model. Int J Environ Res Public Health. 2016;13:772–88.
Li J, Wang N, Wang J, Li H. Spatiotemporal evolution of the remotely sensed global continental PM2.5 concentration from 2000-14 based on Bayesian statistics. Environ Pollut. 2018;238:471–81.
Zhang B, Wang HJ, Ww DU. [Progress of cohort study and its inspiration to China health and nutrition survey]. Zhonghua yu Fang yi xue za zhi [Chin J Prev Med]. 2011;45:295–8.
Popkin BM, Du S, Zhai F, Zhang B. Cohort profile: the China Health and Nutrition Survey—monitoring and understanding socio-economic and health change in China, 1989–2011. Int J Epidemiol. 2010;39:1435–40.
Group of China Obesity Task Force. Body mass index reference norm for screening overweight and obesity in Chinese children and adolescents. Chin J Epidemiol. 2004;25:97–102.
National Bureau of Statistics of China. China Statistical Yearbook 2000 (In Chinese). Beijing, China: China Statistics Press; 2001.
National Bureau of Statistics of China. China Statistical Yearbook 2006 (In Chinese). Beijing, China: China Statistics Press; 2007.
National Bureau of Statistics of China. China Statistical Yearbook 2011 (In Chinese). Beijing, China: China Statistics Press; 2012.
Ministry of Health of China. China Health Statistics Yearbook 2000 (In Chinese). Beijing, China: People’s Medical Publishing House; 2001.
Ministry of Health of China. China Health Statistics Yearbook 2006 (In Chinese). Beijing, China: People’s Medical Publishing House; 2007.
Ministry of Health of China. China Health Statistics Yearbook 2011 (In Chinese). Beijing, China: People’s Medical Publishing House; 2012.
Ministry of Education of the People’s Republic of China. China Education Yearbook 2000 (In Chinese). Beijing, China: People’s Education Press; 2001.
Ministry of Education of the People’s Republic of China. China Education Yearbook 2006 (In Chinese). Beijing, China: People’s Education Press; 2007.
Ministry of Education of the People’s Republic of China. China Education Yearbook 2011 (in Chinese). Beijing, China: People’s Education Press; 2012.
National Light Industry Bureau. China Light Industry Yearbook 2000 (in Chinese). Beijing, China: China Light Industry Press; 2001.
China Light Industry Association. China Light Industry Yearbook 2006 (in Chinese). Beijing, China: China Light Industry Yearbook Press; 2007.
Zhi Liu, China Food Industry Yearbook Editorial Board. China Food Industry Yearbook 2011-3 (In Chinese). Beijing, China: Zhonghua Book Company; 2014.
National Bureau of Statistics of China. Chinese census data for 2010 (In Chinese). Beijing, China: China Statistics Press; 2012.
Abdi H, Williams LJ. Partial least squares methods: partial least squares correlation and partial least square regression. Methods Mol Biol. 2013;930:549–79.
Zhao N, Wu ZS, Zhang Q, Shi XY, Ma Q, Qiao YJ. Optimization of parameter selection for partial least squares model development. Sci Rep. 2015;5:1–10. https://doi.org/10.1038/srep11647.
Chin WW, Marcolin BL, Newsted PR. A partial least squares latent variable modeling approach for measuring interaction effects: results from a Monte Carlo simulation study and voice mail emotion/adoption study. Inf Syst Res. 1997;14:189–217.
Rosipal R. Overview and recent advances in partial least squares. International Conference on Subspace, Latent Structure and Feature Selection 2005; 3940: 34-51.
GregoriaMateos-Aparicio. Partial least squares (PLS) methods: origins, evolution, and application to social sciences. Commun Stat. 2011;40:2305–17.
Swinburn BA, Sacks G, Hall KD, Mcpherson K, Finegood DT, Moodie ML, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378:804–14.
Ludwig DS, Nestle M. Can the food industry play a constructive role in the obesity epidemic? JAMA. 2008;300:1808–11.
National Collaborating Centre for Primary Care. Obesity: The Prevention, Identification, Assessment and Management of Overweight and Obesity in Adults and Children. Natl Inst Health & Clin Excell. 2006;10:117–23.
Popkin BM, Adair LS, Wen NS. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70:3–21.
Su C, Zhang B, Wang YF, Jia XF, Xue H, Wang HJ. Epidemics of overweight and obesity among growing childhood in China between 1997 and 2009: impact of family income, dietary intake, and physical activity dynamics. Chin Med J (Engl). 2015; 128: 1879–86.
Su C, Wang HJ, Wang ZH, Zhang JG, Ww DU, Zhang J et al. [Current status and trends of both dietary fat and cholesterol intake among Chinese children and adolescents aged 7 to 17 years old in 9 provinces of China, from 1991 to 2009]. Chin J Epidemiol. 2012; 33: 1208–12.
Huffman WE, Huffman SK, Rickertsen K, Tegene A. Over-nutrition and changing health status in high income countries. Forum for Health Economics & Policy, 2010.
Saleh K. World bank study: a health sector in transition to universal coverage in Ghana. World Bank Other Operational Studies, 2012.
Nazarov ZE, Rendall MS. Differences by mother’s education in the effect of childcare on child obesity. Econ Lett. 2014;124:286–9.
Babu SC, Gajanan SN, Hallam JA. Nutrition Economics: Principles and Policy Applications. London, UK: Elsevier Academic Press; 2016.
WHO. Population-based Approaches to Childhood Obesity Prevention. Geneva, Switzerland: World Health Organization Press; 2012.
Garde A, Lobstein T, Armstrong T, Irwin R, Randby S, Sacks G, et al. A Framework for Implementing the Set of Recommendations on the Marketing of Foods and Non-alcoholic Beverages to Children. Geneva, Switzerland: World Health Organization Press; 2012.
Acknowledgements
This study used data from the CHNS. We thank the National Institute for Nutrition and Health, Chinese Center for Disease Control and Prevention; the Carolina Population Center, University of North Carolina at Chapel Hill; and the US National Institutes of Health (R01-HD30880, DK056350, R24-HD050924, and R01-HD38700) for financial support for the CHNS data collection and management.
Authors contributions
CG and BZ contributed to the initial design of the study. HW, GF, and JL directed the analysis. All authors contributed to the explanation of analysis results. CG wrote the first draft of the paper. All authors have contributed in revising the paper and approving the final version.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Guo, C., Wang, H., Feng, G. et al. Spatiotemporal predictions of obesity prevalence in Chinese children and adolescents: based on analyses of obesogenic environmental variability and Bayesian model. Int J Obes 43, 1380–1390 (2019). https://doi.org/10.1038/s41366-018-0301-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-018-0301-0
