
Abstract
Intrauterine growth restriction (IUGR) may influence adrenocortical function, lipid metabolism and glucose tolerance in later life. Both cortisol (F) synthesis and metabolism contribute to serum F concentrations. 11β-hydroxysteroid dehydrogenase type 2 (11β-HSD2) enzyme converts F to biologically inactive cortisone (E). Decreased 11β-HSD2 activity has been suggested for a reason to IUGR and to its metabolic consequences. Our aim was to develop a specific liquid chromatography - tandem mass spectrometry (LC-MS/MS) method for analysing serum F and E concentrations, to determine the F/E ratios, and to correlate them with serum lipid concentrations, insulin resistance index (HOMA-IR), and catch-up growth in children born small for gestational age (SGA). The mean serum F and E concentrations, and F/E ratios did not differ between the SGA and their control children at 12 y age. The SGA children in the highest F/E ratio quartile had poorer gain in height between 0-12 y, and higher serum total and LDL cholesterol levels than those with lower F/E ratios. In logistic regression analysis, high LDL cholesterol, high HOMA-IR, and early pubertal stage associated with high F/E ratio in the SGA children. In conclusion, our LC-MS/MS method enables a reliable measurement of both F and E concentrations from a single serum sample. High serum F/E ratio may be associated with IUGR, its metabolic consequences, and poor catch-up growth in a subset of SGA children.
Similar content being viewed by others
Main
Intrauterine growth restriction (IUGR) is associated with increased prevalence of cardiovascular diseases in adulthood (1). The exact mechanisms are still unknown. However, altered activity of the hypothalamo-pituitary-adrenal (HPA) axis may be involved. Recent studies have shown that subjects with low birth weight may have increased plasma cortisol (F) concentrations, increased urinary glucocorticoid metabolite excretion or enhanced plasma F response to ACTH (2–6).
Both F secretion and metabolism contribute to serum F concentration. 11β-hydroxysteroid dehydrogenase type 2 (11β-HSD2) enzyme is responsible for the conversion of F to biologically inactive cortisone (E) (7). In the fetus, 11β-HSD2 is expressed mainly in the lungs, adrenals, colon and kidneys, and in adults in the mineralocorticoid targes tissues, kidneys and colon (7). In the placenta, 11β-HSD2 has a crucial role protecting fetus from deleterious effects of maternal glucocorticoids (8). 11β-HSD2 activity is reduced in excessive liquorice consumption and in apparent mineralocorticoid excess (AME) owing to mutations in the 11β-HSD2 gene. In these states F binds to the mineralocorticoid receptor causing hypokalemic alkalosis and hypertension (9,10).
Animal studies have shown that 11β-HSD2 inhibition by carbenoxolone in a pregnant rat causes fetal growth restriction and elevated blood pressure in the offspring in later life. If the pregnant rats were adrenalectomized, carbenoxolone had no effect on birth weight or blood pressure (11). Furthermore, if dexamethasone, a poor substrate for 11β-HSD2, is given to a pregnant rat, the offspring's birth weight is reduced and blood pressure elevated (12,13). In human, reduced placental 11β-HSD2 gene expression has been reported in IUGR and preeclamptic pregnancies (8,14). In addition, patients with AME invariably have IUGR (9,10). Accordingly, F metabolism seems to be an important factor regulating fetal growth.
Our aim was to develop a specific liquid chromatography - tandem mass spectrometry (LC-MS/MS) method for analysing serum F and E concentrations, to determine the F/E ratios, and to correlate them with serum lipid concentrations, insulin resistance index (HOMA-IR), and catch-up growth in children born small for gestational age (SGA) and in their control subjects born appropriate for gestational age (AGA).
METHODS
Definitions.
SGA was defined as birth weight or length or ponderal index >2 SD scores below the respective mean for the gestational age and sex (15). The ponderal index was calculated as (weight [g]/length3[cm]) × 100. AGA was defined as birth weight, birth length and ponderal index ≥−2 SD scores and ≤2 SD scores of the respective mean for the gestational age and sex. Full-term applied to babies born at or after week 37 and before the 42nd week of gestation (calculated from the beginning of the last menstruation). Body mass index was defined according to the formula weight(kg)/height2(m). Insulin resistance index HOMA-IR was calculated as (serum fasting insulin[mU/L] × blood glucose[mmol/L])/22.5 (16). Parent-specific expected height (PSEH) was calculated as determined by Pere et al. (17).
Subjects.
The study population consisted of all full-term children who were born SGA at Kuopio University Hospital, Finland, during a 22-mo period between 1984 and 1986; 73 SGA children (70 singletons and 3 twins) were included in the study. Five 12-y-old children born SGA could not be reached, one child was excluded because of a metabolic disease (Salla disease), one child was excluded by age (12.8 y) and 11 were unwilling to participate in the study. Thus 18 (24.7%) subjects of the original SGA children were excluded from the study. Each SGA child had, as the control subject, the next born full-term AGA child matched for sex. At the age of 12 y, 55 SGA children (20 boys and 35 girls) and 55 AGA control subjects participated in this study. The mean age in both the study and the control group was 12.2 (SD 0.2) years. The study protocol was approved by the Research Ethics Committee of Kuopio University Hospital. Informed written consent was obtained from the child and the parents.
Perinatal data.
Perinatal data (e.g., birth weight, length, head circumference and duration of gestation) were obtained from hospital records. The birth measures were converted to SD scores by plotting them on the growth charts and adjusting the birth measures for duration of gestation and gender (15). The mean birth weights and lengths for the SGA and AGA groups were 2452 g (−2.44 SD score) versus. 3455 g (-0.24 SD score), p < 0.001, and 46.2 cm (−2.27 SD score) versus. 50.4 cm (-0.08 SD score), p < 0.001, respectively. The mean (SD) gestational age was 39.0 (1.4) weeks in the SGA group and 39.7 (1.5) weeks in the AGA group. A detailed description of the perinatal characteristics was reported previously (18). The mean birth measures of the children who dropped out of the study did not differ from those of the participating SGA children.
Anthropometric measures and pubertal development.
At the ages of 5 and 12 y, height was measured with a calibrated Harpenden stadiometer (Holtain, Ltd, Crymych, UK) and recorded to the nearest 0.1 cm, and weight was recorded to the nearest 0.1 kg. Height was converted to SD scores and weight to percentages in relation to the mean weight-for-height by using the current Finnish reference values for height and weight-for-height (Pegasos V 3.9.2, Pediatric Research Foundation, Helsinki, Finland). The anthropometric data at 5 y age were previously reported (18), and those at 12 y age are presented in Table 1. A complete physical examination was performed on all children. Pubertal development was assessed according to the Tanner staging scale (19,20). For the statistical analyses, pubertal stage was defined by breast scores for girls and genital scores for boys (scores 1–5). Pubertal development did not differ between the SGA and AGA children at 12 y age (p = 0.917, the marginal homogeneity test). PSEH could not be calculated for four SGA children, because one child had been adopted as a newborn, and heights for three fathers were not known.
Blood sampling and laboratory analyses.
Blood samples were taken in the morning, between 9:00 and 10:00 am, after an overnight fast. An i.v. cannula was placed in the antecubital vein for blood sampling, and blood samples were drawn through the cannula, after the child had rested for one hour in recumbent position. The serum specimens were immediately frozen and stored at −70°C until analyzed.
F and E assays.
Serum F and E concentrations were measured by LC-MS/MS. Before analysis, 25 μL of 1 μM deuterated F as internal standard (IS) (9,12,12-D3-cortisol, Cambridge Isotope Laboratories, Andover, MA) in 40% (vol/vol) methanol was added to 100 μL of serum before solid phase extraction (SPE, Bakerbond C18, 500 mg, 3 mL, Phillipsburg, NJ). The columns were pretreated with methanol followed by water. After sample application the columns were washed first with water and then with 20% (vol/vol) acetone. Steroids were eluted with ethyl acetate. After evaporation the residues were dissolved in 100 μL of 40% (vol/vol) methanol. Calibrators containing 10-1000 nmol/L of F (USP Hydrocortisone, H-3160, Sigma Chemical Co., St. Louis, MO) and E (C-2755, Sigma Chemical Co.) were prepared in 40% (vol/vol) methanol. Five μL of sample extracts and calibrators were analysed on an LC-MS/MS system equipped with an API 2000 triple quadrupole mass spectrometer (PE Sciex, Foster City, CA). Peripherals included an Agilent series 1100 HPLC system with a quaternary pump (Waldbronn, Germany). Separation was performed on a Purospher Star RP-18 column (2 × 55 mm; Merck, Darmstadt, Germany). The mobile phase was a linear gradient consisting of methanol and water, at a flow rate of 300 μL/min. The gradient was: 0 min, 40% methanol; 3 min, 90% methanol; and 3.5-10 min 40% methanol. The column was directly connected to the electrospray ionisation probe. F and E were detected in the negative mode with the following transitions: F, m/z 361.2 to m/z 331.2, E m/z 359.1 to m/z 328.8 and IS, m/z 364.2 to m/z 334.2. Data were acquired and processed with the Analyst Software (Ver. 1.3; Sciex). The mass calibration and resolution adjustments (at 0.7 atomic mass units at full width and half height) on both the resolving quadrupoles were optimised using a polypropylene glycol solution with an infusion pump.
Serum lipid, insulin, and blood glucose measurements.
Serum lipid concentrations in these SGA and AGA children were measured by standard methods and reported previously (18). Serum insulin concentrations were determined by RIA (Phadeseph Insulin RIA, Pharmacia & Upjohn Diagnostics AB, Uppsala, Sweden) and blood glucose levels by a glucose oxidase method (Enzyme electrode, Nova Biomedical, Waltham, MA).
Data analysis.
Data were analysed using the statistical program SPSS for Windows, release 10.0 (SPSS Inc., Chicago, IL). All continuous variables were examined for normality with the Kolmogorov-Smirnov test. Nonnormally distributed variables were log transformed before testing with parametric tests. Correlation coefficients were examined by Pearson's or Spearman's correlation tests. The Wilcoxon matched pairs signed rank test or paired sample t test was used in comparing the means between the SGA and AGA group. The Mann-Whitney test was used in comparing nonnormally distributed variables between the subgroups of the SGA or AGA population, whereas the independent-samples t test was used for variables with normal distributions. The repeated measures ANOVA was used in analysing catch-up growth in the SGA children. The factors associating with high F/E ratios were analysed by the logistic regression analysis. A significance level of p < 0.05 was used for all analyses.
RESULTS
Serum F and E LC-MS/MS assays.
The between-assay CV calculated from 11 replicates for serum samples containing 511 nmol/L of F and 29 nmol/L of E were 4.6 and 8.3%, respectively. The detection limit of the assay was 2 nmol/L of F and 3 nmol/L of E based on a signal-to-noise ratio of 3. F concentrations from the same serum samples had been analysed previously by DPC Immulite 2000, chemiluminescent enzyme immunoassay, EIA (Diagnostic Products Corporation, Los Angeles, CA) (21). The EIA-measured F concentrations correlated well with the LC-MS/MS-measured ones in both the SGA and AGA groups (r = 0.934, p < 0.001; r = 0.904, p < 0.001, respectively). The LC-MS/MS-measured F concentrations were on average 23% lower than the EIA-measured ones in both the SGA and AGA groups.
Serum F and E concentrations, and F/E ratios in the SGA and AGA children.
The mean serum F and E concentrations, and F/E ratios did not differ between the SGA and AGA children (Table 2). However, the SGA children in the highest F quartile (n = 14) had higher F concentrations than the AGA children in their highest F quartile (n = 14) (379.9 versus. 305.7 nmol/L, p = 0.043), and these SGA children also tended to have higher E concentrations than the AGA children with high F levels (114.6 versus. 96.9 mM, p = 0.060), while the F/E ratios were similar (3.35 versus. 3.23, p = 0.652). Furthermore, the SGA boys had significantly higher serum F concentrations than the SGA girls did, whereas the F/E ratios did not differ significantly (Table 2).
The relationship between F/E ratios and anthropometric measures in the SGA children.
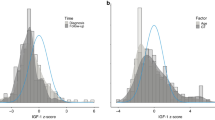
The F/E ratios did not correlate with birth measures, but they correlated inversely with height SD scores at 5 y (r = -0.274, p = 0.043) and 12 y age (r = -0.302, p = 0.025). Gain in height between 0 and 5 y, adjusted by PSEH, tended to be poorer in the SGA children in the highest F/E ratio quartile than in those in the other quartiles. Furthermore, gain in height between 0 and 12 y, adjusted by PSEH and pubertal development, was significantly poorer in the SGA children with high F/E ratios than in those with lower F/E ratios (Fig. 1). The PSEH did not differ significantly between the low and high F/E ratio groups (–0.13 and –0.39 SD scores, respectively, p = 0.100).

Height SD score (SDs) development in the SGA children with high and low F/E ratios (the highest and the other quartiles, respectively). The p-values show the statistical difference in height SDs gains from 0 to 5* and from 0 to 12** years of age between the subgroups.
The relationship between F/E ratios and serum lipid concentrations.
In the SGA children, the F/E ratios correlated positively with serum total and LDL cholesterol levels (r = 0.313, p = 0.020; r = 0.401, p = 0.002, respectively). The SGA children in the highest F/E ratio quartile had significantly higher serum total and LDL cholesterol levels than those in the lower F/E ratio quartiles (5.07 versus. 4.42 mM, p = 0.018; 3.28 versus. 2.71 mM, p = 0.007, respectively). However, in the AGA children no significant correlations were found between the F/E ratios and serum total or LDL cholesterol concentrations (r = 0.037, p = 0.788; r = 0.042, p = 0.760, respectively). Neither did the serum total nor LDL cholesterol concentrations differ significantly between the high and low F/E ratio subgroups (4.58 versus. 4.25 mM, p = 0.150; 2.83 versus. 2.55 mM, p = 0.150, respectively) in the AGA group. Furthermore, the SGA children in the highest F quartile had higher total and LDL cholesterol concentrations than the SGA children in the lower F quartiles (5.15 mM versus. 4.39 mM, p = 0.005; 3.24 mM versus. 2.72 mM, p = 0.015, respectively).
The factors associating with high F/E ratios.
In the multiple logistic regression analyses, the F/E ratio variable was dichotomised in the SGA and AGA groups; as the cut-off point we used the levels of the 75th percentile in the SGA and AGA groups, respectively. All the factors included in the analyses are shown in Table 3. According to the multiple logistic regression analysis, high LDL cholesterol, high HOMA-IR, and early pubertal stage were significantly associated with high F/E ratios in the SGA children. An increase of 1.0 mM in LDL cholesterol increased by 3.6-fold the risk of high F/E ratio, and an increase of 1.0 unit in HOMA-IR increased the risk by 3.3-fold (Table 3). Logistic regression analysis was performed with an identical model in the AGA group; none of the covariates reached statistical significance (Table 4).
DISCUSSION
We found no significant differences in serum F and E concentrations or F/E ratios between the SGA and AGA groups, but high concentrations of serum F were more common in the SGA than in the AGA children if the highest F quartiles in each group were compared. High serum total and LDL cholesterol levels associated with both high F/E ratios and high serum F levels in the SGA group. In logistic regression analysis, high F/E ratios associated with high LDL cholesterol and HOMA-IR. In addition, the SGA children with the highest F/E ratios had the poorest catch-up growth.
The strengths of the present study are the well-characterized population based study group of the SGA children and their matched controls, and the specific LC-MS/MS assay for serum F and E concentrations. Our present F levels were about 23% lower than those measured by an EIA assay (21), which is most probably due to the lack of interferences and cross-reactions often detected in immunoassays. Our F/E ratios were also somewhat lower than those derived from immunologic assays by Dötsch and coworkers (22).
In adult populations, Phillips and coworkers found an inverse relation between birth weight and plasma F concentrations (2,3). In these subjects increased plasma F levels associated with elevated blood pressure, increased concentration of triglycerides, and insulin resistance (2,3). According to Reynolds et al. plasma F response to ACTH and urinary F metabolite excretion were increased in men with low birth weight (5). In children, increased urinary F metabolite excretion was found in subjects with low birth weight (4), while in another population no differences were found in the circadian serum F concentrations between short SGA and short AGA children (23). Consequently, increased activity of the HPA axis seems to be associated with IUGR.
Plasma F and E concentrations, and their ratios have been used previously as an indirect measurement of 11β-HSD2 activity (22,24). Dötsch et al. reported that during the first year of life the F/E ratio increases, but stays quite stable later in childhood and adolescence (22). Decreased 11β-HSD2 activity has been suggested for a factor linking IUGR and its metabolic consequences (13,24). Houang and coworkers studied serum F and E concentrations by RIA in a 1-13-y-old IUGR study population without catch-up growth and in a small control group. They found that 20% of their IUGR children had high F/E ratios suggesting a possible partial 11β-HSD2 defect. These IUGR children had significantly higher total cholesterol concentrations, systolic blood pressure, and a tendency toward higher fasting insulin levels than the IUGR children with low F/E ratios and the control children (24). Furthermore, both high F/E ratios (24) and high F levels have been associated with poor catch-up growth (25).
In the present study no differences were found in serum F concentrations and F/E ratios between the SGA and AGA children, but in comparing the highest F quartiles in the study and the control group, the SGA children had significantly higher F levels than the AGA ones. Interestingly, the F/E ratios did not differ between the highest F quartiles in the SGA and the AGA group. Thus, our findings were consistent with those of Houang and coworkers (24) in respect of the relationship between serum lipid concentrations and high F/E ratios. However, in our SGA children both high serum F concentration and F/E ratio associated with high total and LDL cholesterol concentration and HOMA-IR index, whereas only high F/E ratio associated with poor catch-up growth.
In conclusion, our LC-MS/MS method enables a rapid and reliable measurement of both F and E concentrations from a single small serum sample. High serum F/E ratio may be associated with IUGR, its metabolic consequences, and poor catch-up growth at least in a subset of SGA children.
Abbreviations
- IUGR:
-
intrauterine growth restriction
- F:
-
cortisol
- E:
-
cortisone
- 11β-HSD2:
-
11β-hydroxysteroid dehydrogenase type 2
- LC-MS/MS:
-
liquid chromatography – tandem mass spectrometry
- HOMA-IR:
-
insulin resistance index
- SGA:
-
small for gestational age
- AGA:
-
appropriate for gestational age
- HPA:
-
hypothalamo-pituitary-adrenal
- PSEH:
-
parent-specific expected height
References
Barker DJ, Gluckman PD, Godfrey KM, Harding JE, Owens JA, Robinson JS 1993 Fetal nutrition and cardiovascular disease in adult life. Lancet 341: 938–941
Phillips DI, Barker DJ, Fall CH, Seckl JR, Whorwood CB, Wood PJ, Walker BR 1998 Elevated plasma cortisol concentrations: a link between low birth weight and the insulin resistance syndrome?. J Clin Endocrinol Metab 83: 757–760
Phillips DI, Walker BR, Reynolds RM, Flanagan DE, Wood PJ, Osmond C, Barker DJ, Whorwood CB 2000 Low birth weight predicts elevated plasma cortisol concentrations in adults from 3 populations. Hypertension 35: 1301–1306
Clark PM, Hindmarsh PC, Shiell AW, Law CM, Honour JW, Barker DJ 1996 Size at birth and adrenocortical function in childhood. Clin Endocrinol 45: 721–726
Reynolds RM, Walker BR, Syddall HE, Andrew R, Wood PJ, Whorwood CB, Phillips DI 2001 Altered control of cortisol secretion in adult men with low birth weight and cardiovascular risk factors. J Clin Endocrinol Metab 86: 245–250
Levitt NS, Lambert EV, Woods D, Hales CN, Andrew R, Seckl JR 2000 Impaired glucose tolerance and elevated blood pressure in low birth weight, nonobese, young South African adults: early programming of cortisol axis. J Clin Endocrinol Metab 85: 4611–4618
Stewart PM, Whorwood CB, Mason JI 1995 Type 2 11β-hydroxysteroid dehydrogenase in foetal and adult life. J Steroid Biochem Mol Biol 55: 465–471
McTernan CL, Draper N, Nicholson H, Chalder SM, Driver P, Hewison M, Kilby MD, Stewart PM 2001 Reduced placental 11β-hydroxysteroid dehydrogenase type 2 mRNA levels in human pregnancies complicated by intrauterine growth restriction: an analysis of possible mechanisms. J Clin Endocrinol Metab 86: 4979–4983
Dave-Sharma S, Wilson RC, Harbison MD, Newfield R, Azar MR, Krozowski S, Funder JW, Shackleton L, Bradlow HL, Wei JQ, Hertecant J, Moran A, Neiberger RE, Balfe JW, Fattah A, Daneman D, Akkurt HI, De Santis C, New MI 1998 Examination of genotype and phenotype relationships in 14 patients with apparent mineralocorticoid excess. J Clin Endocrinol Metab 83: 2244–2254
Kitanaka S, Tanae A, Hibi I 1996 Apparent mineralocorticoid excess due to 11β-hydroxysteroid dehydrogenase deficiency: a possible cause of intrauterine growth retardation. Clin Endocrinol (Oxf) 44: 353–359
Lindsay RS, Lindsay RM, Edwards CR, Seckl JR 1995 Inhibition of 11β-hydroxysteroid dehydrogenase in pregnant rats and the programming of blood pressure in the offspring. Hypertension 27: 1200–1204
Benediktsson R, Lindsay RS, Noble J, Seckl JR, Edwards CR 1993 Glucocorticoid exposure in utero: a new model for adult hypertension. Lancet 341: 339–341
Seckl JR, Cleasby M, Nyirenda MJ 2000 Glucocorticoids, 11β-hydroxysteroid dehydrogenase, and fetal programming. Kidney Int 57: 1412–1417
Schoof E, Girstl M, Frobenius W, Kirschbaum M, Dörr HG, Rascher W, Dötsch J 2001 Decreased gene expression of 11β-hydroxysteroid dehydrogenase type 2 and 15-hydroxyprostaglandin dehydrogenase in human placenta of patients with preeclampsia. J Clin Endocrinol Metab 86: 1313–1317
Pihkala J, Hakala T, Voutilainen P, Raivio K 1989 New Finnish fetal growth charts (in Finnish). Duodecim 105: 1540–1546
Uwaifo GI, Fallon EM, Chin J, Elberg J, Parikh SJ, Yanovski JA 2002 Indices of insulin action, disposal, and secretion derived from fasting samples and clamps in normal glucose-tolerant black and white children. Diabetes Care 25: 2081–2087
Pere A, Perheentupa J, Peter M, Voutilainen R 1995 Follow up of growth and steroids in premature adrenarche. Eur J Pediatr 154: 346–352
Tenhola S, Martikainen A, Rahiala E, Herrgård E, Halonen P, Voutilainen R 2000 Serum lipid concentrations and growth characteristics in 12-year-old children born small for gestational age. Pediatr Res 48: 623–628
Marshall WA, Tanner JM 1969 Variations in pattern of pubertal changes in girls. Arch Dis Child 44: 291–303
Marshall WA, Tanner JM 1970 Variations in pattern of pubertal changes in boys. Arch Dis Child 45: 13–23
Tenhola S, Martikainen A, Rahiala E, Parviainen M, Halonen P, Voutilainen R 2002 Increased adrenocortical and adrenomedullary hormonal activity in 12-year-old children born small for gestational age. J Pediatr 141: 477–482
Dötsch J, Hohenberger I, Peter M, Sippell W, Dörr HG 2000 Evidence for change of 11β-hydroxysteroid dehydrogenase activity during infancy and childhood. Pediatr Res 48: 697–700
Dahlgren J, Boguszewski M, Rosberg S, Albertsson-Wikland K 1998 Adrenal steroid hormones in short children born small for gestational age. Clin Endocrinol (Oxf) 49: 353–361
Houang M, Morineau G, Le Bouc Y, Fiet J, Gourmelen M 1999 The cortisol-cortisone shuttle in children born with intrauterine growth retardation. Pediatr Res 46: 189–193
Cianfarani S, Geremia C, Scott CD, Germani D 2002 Growth, IGF system and cortisol in children with intrauterine growth retardation: is catch-up growth affected by reprogramming of the hypothalamic-pituitary-adrenal axis?. Pediatr Res 51: 94–99
Acknowledgements
This study was supported by Kuopio University Hospital, Maud Kuistila Foundation, Sigrid Juselius Foundation, Pediatric Research Foundation, and Academy of Finland.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tenhola, S., Turpeinen, U., Halonen, P. et al. Association of Serum Lipid Concentrations, Insulin Resistance Index and Catch-Up Growth with Serum Cortisol/Cortisone Ratio by Liquid Chromatography Tandem Mass Spectrometry in Children Born Small for Gestational Age. Pediatr Res 58, 467–471 (2005). https://doi.org/10.1203/01.pdr.0000176908.93031.97
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.pdr.0000176908.93031.97
This article is cited by
-
Catch-up growth in body mass index is associated neither with reduced insulin sensitivity nor with altered lipid profile in children born small for gestational age
Journal of Endocrinological Investigation (2008)
