
Abstract
This prospective study aimed to evaluate the diagnostic utilities of neutrophil CD64 expression for the identification of early-onset clinical infection and pneumonia in term infants and to define the optimal cutoff value so that it may act as a reference with which future studies can be compared. Term newborns in whom infection was suspected when they were <72 h of age were recruited into the study. C-reactive protein (CRP) and expression of CD64 on neutrophils were measured at 0 h (at the time of sepsis evaluation) and 24 h. The sensitivity, specificity, positive predictive value, and negative predictive value (NPV) of CRP, CD64, and the combination of these two markers for predicting neonatal sepsis were determined. A total of 338 infants with suspected clinical sepsis were investigated, 115 of whom were found to be clinically infected. CRP and CD64 in infected infants were both significantly elevated at 0 and 24 h compared with noninfected infants (p < 0.001). The calculated optimal cutoff value for CD64 was 6136 antibody-phycoerythrin molecules bound/cell. CD64 has a very high sensitivity (96%) and NPV (97%) at 24 h. The addition of CRP only marginally enhanced the sensitivity and NPV (97 and 98%, respectively). In conclusion, neutrophil CD64 is a very sensitive diagnostic marker for the identification of early-onset clinical infection and pneumonia in term newborns. The results strongly suggest that measurement of neutrophil CD64 may allow neonatal clinicians to discontinue antibiotic treatment at 24 h in infants who are clinically stable and whose CD64 expressions are below the optimal cutoff level.
Similar content being viewed by others


Main
Early-onset (<72 h of age) neonatal infection is associated with a high morbidity and mortality (1). Immature immunologic defenses in newborn infants, including low circulating levels of immunoglobulins, decrease in absolute number of T lymphocytes and neutrophils, and functionally impaired cytotoxic activity in leukocytes (2–4), are important risk factors that predispose these infants to life-threatening sepsis. Early clinical signs and symptoms of neonatal infection and pneumonia are often inconspicuous and can easily be confused with other noninfective causes, such as transient tachypnea of the newborns, meconium aspiration syndrome, congenital heart diseases, and hypoxic-ischemic encephalopathy (5). Thus, there is always a possibility that the attending neonatologists may overlook or miss subtle cases of early infection. In view of the potentially serious outcome associated with delayed treatment and the difficulty in distinguishing infected from noninfected cases, it has become common practice to prescribe broad-spectrum antibiotics for suspected infection that presents with nonspecific clinical features and maternal risk factors (5–7). Furthermore, as negative microbiologic culture results do not always suggest the absence of bacterial sepsis, continuation of antimicrobial therapy for presumptive infection frequently leads to unnecessary and prolonged treatment and increases in duration of hospitalization and promotes the emergence of multiresistant organisms in the neonatal unit. Thus, a good indicator of infection or a set of reliable infection markers would be clinically desirable for differentiating infected from noninfected patients.
CD64, a neutrophil surface antigen, was purposefully chosen as a potential marker for identifying early-onset clinical infection and pneumonia in term infants. Three major classes of Fcγ-receptors (FcγR)—FcγRI (CD64), FcγRII (CD32), and FcγRIII (CD16)—have been characterized on neutrophils and monocytes in humans (8–10). CD64, a high-affinity receptor, is usually expressed at a low concentration on the surface of nonactivated neutrophils in preterm and term infants (11). Upon antigenic challenge by microbial products, its expression will be substantially up-regulated (11–13). Our previous study on late-onset infection in preterm infants suggested that the expression of CD64 peaked 24 h after the onset of clinical manifestations, and the levels remained elevated above the baseline even after 48 h (12). These favorable properties render CD64 a potentially useful indicator for revealing the early stage of immune response to bacterial infection and as a diagnostic marker of neonatal sepsis.
This prospective study aimed 1) to determine the diagnostic utilities [sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV)] of CD64, both individually and in combination with conventional biochemical markers such as C-reactive protein (CRP), for diagnosing early-onset clinical infection and pneumonia in term newborns and 2) to define the optimal cutoff value for neutrophil CD64 using the receiver operating characteristics (ROC) curve so that it may be used as a reference with which future studies can be compared.
METHODS
Patients
Newborn infants who had with 1) gestational age ≥37 wk, 2) postnatal age <72 h, 3) signs and symptoms suggestive of early-onset clinical infection or pneumonia and requiring full sepsis evaluation and antibiotic treatment, and 4) parental consent and were admitted to the neonatal unit at Prince of Wales Hospital, Hong Kong, were eligible for enrollment into the study. Patients who had lethal congenital or chromosomal abnormalities and those whose siblings have known immunodeficiencies were excluded. The use of maternal intrapartum antibiotics, however, did not preclude the infants from participating in the study. The recruitment of suspected infection episode was conducted prospectively over a 30-mo period.
Infection Screen
Term infants with clinical features suggestive of early-onset neonatal infection received a full sepsis workup. These signs and symptoms included 1) unstable temperature (<36.5°C or >37.5°C on two occasions within 12 h); 2) unexplained poor peripheral circulation with prolonged capillary refilling time >3 s; 3) respiratory distress as evidenced by tachypnea (respiratory rate >60 breaths/min), intercostal or substernal retractions, apnea, or central cyanosis; 4) increase in anterior fontanelle tension or convulsion; and 5) persistent vomiting, bloody stool, and abdominal distension. All infants were recruited at the time of evaluation for suspected clinical sepsis. In each suspected episode, a full sepsis screen was performed, which included surface (ears, nose, throat, and umbilicus), urine, stool (suspected cases of enterocolitis), blood, cerebrospinal fluid, and endotracheal aspirate specimens (infants on respirator) for microscopy and bacterial cultures. Chest radiograph was routinely performed, and an abdominal radiograph would be requested when infants presented with signs and symptoms suggestive of necrotizing enterocolitis (NEC) or intra-abdominal sepsis. Hematologic and biochemical investigations such as complete blood cell and platelet counts, blood gas, and serum glucose concentration were also performed. In addition to the routine serial CRP measurement, an EDTA blood specimen (0.2 mL) was obtained for neutrophil CD64 analysis by flow cytometry. The first sample was taken at the time of the initial sepsis evaluation (0 h), and an additional sample was obtained 24 h after the onset of presentation. The schedule of blood sampling coincided exactly with the unit policy for serial blood count and CRP measurements after a suspected infection episode had been identified. Parenteral antibiotics were commenced immediately after the infection screen and the first set of blood sample (0 h) had been obtained.
Classification of Infection Episodes
Three categories of “infection” episodes were defined prospectively in this study.
Group 1 (infected group).
The infected group consisted of infants who had been confirmed as septicemic from positive blood cultures when the same organism was isolated from both blood culture bottles. Other microbiologic-confirmed bacterial infections, including peritonitis, meningitis, and NEC (stage II or above in Bell's classification with or without positive blood culture), (14) were also included in this group. Clinical pneumonia was diagnosed on the basis of respiratory signs in combination with abnormal chest radiographic findings and absence of history such as thick meconium-stained liquor or antenatally diagnosed pleural effusion that could account for the abnormal radiographic appearances. As most infants did not require intubation and mechanical ventilation, bronchopulmonary lavage specimen was not routinely available for microbiologic analysis. The radiologic images were stored digitally in a computed radiographic system (Mobilette Plus; Siemens, Erlargen, Germany) so that the brightness and contrast of these images could be optimized to highlight the abnormal lesions. The digital technology greatly enhanced the chance of picking up subtle features. Extreme care was exercised in interpreting the radiographic findings. All chest radiographs were systematically reviewed by two independent investigators, a neonatologist (P.C.N.) and a pediatric radiologist (W.C.W.C.), who were blinded to the patient's identity, routine laboratory results, and results of the infection markers. During the review process, the investigators specifically looked for air space consolidation, pleural effusion, and peribronchial and perivascular interstitial infiltration. Any disagreement in opinion between the investigators was subjected to a further review, and the final interpretation of radiographic signs was based on a consensus of opinion.
Group 2 (noninfected group).
The noninfected group consisted of patients who met the initial screening criteria for suspected clinical infection but were subsequently found not to have positive bacterial cultures in blood, cerebrospinal fluid, and urine specimens; plus there was no radiologic evidence of pneumonia or NEC; and the infant continued to improve after antibiotic treatment was stopped. Positive surface culture alone was considered only as bacterial colonization, and such infants would not be classified as being infected.
Group 3 (control group).
A control group consisted of 21 well term infants with their blood samples taken within the first 72 h of life for CD64 and CRP measurements. The collection of the blood specimens coincided with other routine blood sampling procedures, such as serum bilirubin, hematocrit, electrolytes, or glucose measurements.
Measurement of Biochemical and Cell-Surface Markers
Blood samples collected from venipunctures were immersed in ice and immediately transported to the laboratory for processing. CRP was measured by a turbidity assay kit against control standards, as specified by the manufacturer (Behring Diagnostics Inc., Westwood, MA). Before each analysis of neutrophil CD64 expression, the QuantiBRITE PE beads (Becton Dickinson Immunocytometry Systems, San Jose, CA) conjugated with four predefined levels of phycoerythrin (PE) molecules were used to construct a standard linear regression curve. This quantitative method represents a substantial improvement over the measurement of relative fluorescence intensity, which may be affected by subtle, day-to-day operational and instrumental fluctuations. The technique provides an accurate and quantitative comparison of the cell-surface antigen expression in time serial analysis (15,16). Freshly collected EDTA blood was maintained at 4°C and stained within 15 min after arrival at the laboratory. The CD64-PE antibodies were of QuantiBRITE grade (≥95% 1:1 antibody:PE ratio) and the staining procedures were performed according to the manufacturer's recommendation. We incubated 0.05 mL of whole blood with 20 μL of CD64-PE/CD45-peridinin chlorophyll protein (Becton Dickinson Immunocytometry Systems; cat. no. 340768) in the dark, at room temperature for 60 min. The red cells were then lysed with 1 mL of 1 × FACS Lysing solution (Becton Dickinson Immunocytometry Systems) for an additional 60 min before cytometric analysis. Thirty thousand events were acquired for each sample, using the FACSCalibur machine and CellQuest software (Becton Dickinson Immunocytometry Systems). The three parts of differential populations (lymphocytes, monocytes, and granulocytes) were identified and gated by their CD45/side-scatter profile. The expressions (geometric mean) of CD64 on neutrophils were measured quantitatively. The antibody-PE binding sites per cell were computed by the QuantiQuest software (Becton Dickinson Immunocytometry Systems), using the linear regression curve of QuantiBRITE beads obtained in parallel with each sample analysis.
Statistical Analysis
The demographic data of the three groups and the levels of infection markers among the infected (group 1; 0 h), noninfected (group 2; 0 h), and control (Group 3) groups were compared using the Kruskal-Wallis test and χ2 test. The Mann Whitney U test was also used to assess the infection risk factors, clinical parameters, and levels of infection markers at 24 h between group 1 and group 2 infants. As there were no recommended diagnostic cutoff values for neutrophil CD64 in term newborns, a ROC curve was constructed for each sampling time point. The optimal cutoff value for CD64 was then determined on the graph by minimizing the number of misclassified episodes. As the diagnostic marker should ideally identify all genuinely infected infants (i.e. 100% sensitivity) and at the same time would not misclassify too many noninfected cases (i.e. high specificity), the optimal cutoff value, therefore, was chosen with the sensitivity approaching 100% and specificity >85% (12,17). However, if the diagnostic marker was unable to satisfy the above criteria, then the optimal cutoff value would be chosen so that both the sensitivity and specificity approached 80%. The calculated optimal cutoff value enables us to work out the diagnostic utilities: sensitivity, specificity, PPV, and NPV of the cell-surface antigen and combination of markers at the most appropriate sampling time for diagnosing early-onset clinical infection and pneumonia in term infants. A combination of tests was considered positive when any one of the selected markers exceeded its respective cutoff value. All statistical tests were performed by SPSS for Windows (Release 11.5; SPSS Inc., Chicago, IL). The level of significance was set at 5% in all comparisons.
Ethical Approval
The study was approved by the Research Ethics Committee of the Chinese University of Hong Kong. Written informed consent was obtained from the parents or guardians for all study patients.
RESULTS
A total of 359 term infants were studied, 115, 223, and 21 of whom belonged to the infected (group 1), noninfected (group 2), and control (group 3) groups, respectively. The demographic profile of the three study groups is summarized in Table 1. There were no significant differences among the groups in gestational age, birth weight, Apgar scores at 1 and 5 min, umbilical arterial cord blood pH, and other parameters listed in Table 1. None of the studied infants died from neonatal sepsis. The antenatal infection risk factors and the clinical presentation between group 1 and group 2 infants are summarized in Tables 2 and 3, respectively. Significantly more infected infants were delivered by spontaneous vaginal delivery (p < 0.01) and had pathogens isolated from high vaginal swabs of mothers (p < 0.005; Table 2). These pathogens included Streptococcus agalactiae (×18), Candida spp. (×5), Escherichia coli (×2), Streptococcus faecalis (×1), and Trichomonas vaginalis (×1). Poor tissue perfusion as evidenced by prolonged capillary refilling time >3 s was also significantly more prevalent in infected infants (p < 0.01; Table 3). Other clinical indices such as body temperature, blood pressure, and respiratory rate were unable to differentiate between infected and noninfected patients (Table 3).
The clinical diagnosis of infected and noninfected infants is summarized in Table 4. Figure 1 shows the flow cytometric profile of CD64 expression on neutrophils of a typical infected infant and a noninfected infant. Table 5 compares the serum CRP concentration and neutrophil CD64 expression at 0 and 24 h after the onset of clinical manifestations between the groups. CD64 and CRP in infected infants were significantly elevated at both 0 and 24 h compared with noninfected infants (p < 0.001) and control subjects (p < 0.001). There was no significant difference in CD64 expressions and serum CRP concentrations between noninfected infants and control subjects. In episodes of confirmed infection, both CD64 and CRP demonstrated their highest levels 24 h after the onset of infection (Fig. 2, Table 5).

Flow cytometric analysis of CD64 expression on neutrophils. The solid histogram represents a significant increase in CD64 expression in a typical infected term infant, whereas the open histogram represents the CD64 expression in a noninfected infant. The mean fluorescence intensity values were expressed quantitatively as antibody-PE molecules bound/cell.

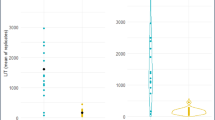
(A and B) Levels of CRP and neutrophil CD64 expression during the first 24 h of suspected clinical infection. Each figure compares the range of an infection marker between the infected and noninfected infants. The bold line and upper and lower boundaries of the shaded area represent the 50th, 75th, and 25th percentiles, respectively, of the infected infants. The thick and thin dotted lines and the upper and the lower boundaries represent the 50th, 75th, and 25th percentiles, respectively, of the noninfected infants.
The ROC curves of CD64 and CRP at 0 and 24 h are shown in Fig. 3. The areas under the curves for CD64 and CRP were 0.88–0.94 and 0.77–0.79, respectively. Table 6 summarizes the diagnostic utilities of CD64 and CRP at various cutoff values during the initial sepsis evaluation (0 h) and 24 h afterward. The assessment of individual markers indicated that CD64 has the highest overall sensitivity and NPV at both time points for the prediction of early-onset clinical infection and pneumonia. We chose the calculated cutoff value of 6136 antibody-PE molecules bound/cell to be the optimal point, as it would permit a very high sensitivity (96%) and NPV (97%), and simultaneously be able to maintain an acceptable specificity >80% (81%) at 24 h (Table 6). In contrast, the cutoff value of CRP ≥10 mg/L currently adopted in the neonatal unit provided only a sensitivity and specificity of 49–60% and 83–91%, respectively (Table 6). In addition, a comparison of the diagnostic utilities of CD64 and CRP in combination versus individual markers suggested that the use of multiple markers was associated with only a marginal improvement of sensitivity and NPV (97 and 98%, respectively; Table 7).

The ROC curves of CRP and neutrophil CD64 expression at 0 h (A) and 24 h (B).
DISCUSSION
Our findings suggested that neutrophil CD64 expression was substantially up-regulated in term infants with early-onset clinical infection and pneumonia (Table 5). CD64 was capable of differentiating infected from noninfected conditions such as hypoxic-ischemic encephalopathy, meconium aspiration syndrome, and transient tachypnea of the newborns, presenting with similar clinical signs and symptoms. As the diagnostic utilities (sensitivity, specificity, PPV, and NPV) ultimately determine the usefulness of a clinical test, the one with a high sensitivity and NPV (approaching 100%) would be most desirable in this situation because all genuinely infected cases are required to be identified and treated (18). The test should also have an acceptable specificity (>80%) so that misclassification of noninfected cases and unnecessary use of antibiotics could be kept to a minimum. Hence, we have presented different cutoff values of CD64 from the ROC curve for assessment (Table 6). The cutoff value of 6136 antibody-PE molecules bound/cell was considered optimal, as it exhibited a very high sensitivity (96%) and a moderate specificity (81%). Using this value, CD64 correctly identified all septicemic cases [Streptococcus agalactiae (×3) and Staphylococcus aureus (×1)] and the severe case of NEC. However, 5 infants with clinical pneumonia were missed, and 43 noninfected patients were incorrectly classified into the infected group. Combining the use of CD64 (≥6136 antibody-PE molecules bound/cell) with CRP (≥10 mg/L) would improve the sensitivity to 97% but substantially lower the specificity (71%; Table 7). Two of the 5 clinical pneumonia cases missed by the CD64 assessment would have been positively identified by CRP, but an additional 22 noninfected infants would have been misclassified and would have inadvertently received a prolonged course of antibiotics. Although the number of clinical pneumonia cases seemed to be high, this figure represented <1% of all liveborn infants within the study period. The use of an advanced digital computed radiographic system could also have enhanced the diagnostic value of chest radiograph compared with the predigital era. Similar to preterm infants, the increase in expression of the surface antigen on neutrophils was sustained for at least 24 h after the initial presentation of symptoms and even after antimicrobial treatment (12). This phenomenon has also been observed in a small number of septic patients (n = 3) monitored serially in a recent study (13). This intrinsic property greatly broadens the diagnostic window for identifying neonatal sepsis in the early phase and allows blood specimens to be collected within normal working hours for laboratory assay.
To our knowledge, only three studies, including our previous study in preterm infants (12), had investigated the expression of CD64 in neonatal sepsis (11,13). In accordance with the results of the current study, all suggested that neutrophil CD64 from both infected term and preterm infants were significantly up-regulated compared with noninfected infants and healthy newborns (11–13). The diagnostic utilities between this and our previous study (12) are also very similar, suggesting that CD64 is a very sensitive and moderately specific marker for both early- and late-onset infection in neonates. Layseca-Espinosa et al. (13), however, found that a single determination of CD64 was associated with a high specificity (96.8%) and a very low sensitivity (25.8%). Several plausible explanations could account for the disparity of this observation. First, as the results of the current and our previous studies (12) indicated that the peak CD64 expression occurred at ∼24 h after the initial sepsis evaluation, the use of the second blood sample (i.e. the 24-h sample) or serial measurements for calculating the diagnostic utilities, therefore, should be more representative. Second and more important, Layseca-Espinosa et al. (13) defined the cutoff value arbitrarily as the arithmetic mean +3 SD of the expression values observed in control healthy newborns and did not use the ROC curve for determination of the optimal cutoff point. The disadvantage of using such a stringent cutoff criterion would almost certainly render the test highly specific but relatively insensitive. Third, the sample size of the latter study (13) was comparatively small (n = 48, excluding healthy control subjects). Fourth, the semiquantitative analysis gave only a “relative” rather than an absolute measurement, and the latter results might not be comparable among different laboratories. The current study with a much larger sample size and with quantitative measurement of neutrophil CD64 expression should more accurately reflect the diagnostic utilities of the test. In addition, the optimal cutoff value used in this study was slightly different from the one used for the late-onset infection in preterm infants (CD64 expression ≥4000 antibody-PE molecules bound/cell) (12). Although Fjaertoft et al. (11) suggested that there were no significant differences in neutrophil CD64 expression during bacterial infections among adults (n = 6), children (n = 14), and preterm (n = 9) and term newborn infants (n = 3), the number of subjects studied were small. We speculate that differences in gestational age, postnatal age at which the tests were performed, and the types of infection such as septicemia versus clinical pneumonia may influence the maturity of the complex activation system of neutrophil and the level of CD64 expression in different categories of infants. Thus, our finding further emphasizes the importance of establishing an optimal cutoff value for each group of patients.
A major intrinsic difficulty of assessing diagnostic markers for early-onset clinical sepsis in neonates is the problem of misclassification of suspected infection episodes. As the incidence of septicemia in early-onset neonatal infection is low (5,6), the classification of clinical sepsis in this setting depends mainly on clinical features and abnormal radiologic findings. We sought to minimize some of the problems by 1) prospectively standardizing the definition of infection, 2) effectively blinding the independent assessors from the results of the diagnostic markers and concealing the identity of the patient during the classification process, 3) using the latest digital technology in enhancing the radiographic film quality, and 4) having a relatively large sample size in the study. Furthermore, unlike most previous studies (5,6,13), we purposefully classified the suspected infected episodes into just two groups, the “infected” and the “noninfected” groups, to simulate the therapeutic decision-making process in clinical practice. The absence of buffer groups, such as “possible infection group” (5), “suspected infection group” (6), or “clinical sepsis group” (13), may theoretically increase the probability of misclassification of cases. However, our findings indicated that CD64 remained a sensitive marker for identification of early- and late-onset neonatal sepsis. It was possible that neonatal sepsis might occur in the absence of septicemia, meningitis, NEC, and pneumonia and thus affected the diagnostic utilities of the tests. In the current study, six infants who were classified as being noninfected but ran a severe clinical course and had negative blood culture and radiographic finding were subsequently found to have both increased CD64 expression and raised serum CRP concentrations (Table 4). All received a full course of antibiotics. The clinical and biochemical evidence suggested that these infants were most likely to be infected rather than false-positive cases. Including these cases to the infected group would improve the specificity and PPV of CD64 to 83 and 75%, respectively.
Recent reports suggested that the expression of other cell surface antigens such as CD11b on neutrophils (5,6), CD45RO and CD25 on lymphocytes (19–21), and CD69 on NK cells (22) were potential valuable markers for predicting neonatal sepsis. However, not all have been validated to be suitable for clinical use. CD11b has been found to be a sensitive diagnostic marker for early-onset clinical infection (5,6), but our previous study was unable to confirm its diagnostic value for late-onset sepsis in preterm infants (12). We have in this series shown that CD64 is a sensitive infection marker for both early- and late-onset neonatal infection, in term and preterm infants. The advantages of using CD64 as a diagnostic marker are that 1) the flow cytometric analysis can be performed with minimal blood volume (50 μL of whole blood); 2) the result is available within 4 h after the specimen reaches the laboratory; 3) the measurement is “quantitative” and thus enables comparison of results among different centers; 4) unlike cytokines, which are usually assayed in batches (18), the measurement of cell surface antigens is performed on an ad hoc basis; 5) the persistent expression of CD64 for at least 24 h gives the marker a wide diagnostic window; and 6) the very favorable diagnostic utilities render CD64 one of the best infection markers for the identification of early- and late-onset neonatal sepsis.
CONCLUSION
In conclusion, our findings strongly suggest that measurement of neutrophil CD64 may allow neonatal clinicians to discontinue antimicrobial treatment at 24 h, without waiting for the definitive microbiologic culture results, in infants who are clinically stable and whose CD64 expressions are below the predefined cutoff value.
Abbreviations
- CRP:
-
C-reactive protein
- FcγR:
-
Fcγ-receptor
- NEC:
-
necrotizing enterocolitis
- NPV:
-
negative predictive value
- PE:
-
phycoerythrin
- PPV:
-
positive predictive value
- ROC:
-
receiver operating characteristics
References
Klein JO, Marcy SM 1995 In: Bacterial sepsis and meningitis. Remington JS, Klein JO (eds) Infectious Diseases of the Fetus and Newborn Infant. WB Saunders, Philadelphia, pp 835–890
Anderson DC 1992 Neonatal neutrophil dysfunction. J Lab Clin Med 120: 816–817
Rowen JL, Smith CW, Edwards MS 1995 Group B streptococci elicit leukotriene B4 and interleukin-8 from human monocytes: neonates exhibit a diminished response. J Infect Dis 172: 420–426
Holt PG 1995 Postnatal maturation of immune competence during infancy and childhood. Pediatr Allergy Immunol 6: 59–70
Nupponen I, Andersson S, Järvenpää AL, Kautiainen H, Repo H 2001 Neutrophil CD11b expression and circulating interleukin-8 as diagnostic markers for early-onset neonatal sepsis. Pediatrics 108: E12–E17
Weirich E, Rabin RL, Maldonado Y, Benitz W, Modler S, Herzenberg LA, Herzenberg LA 1998 Neutrophil CD11b expression as a diagnostic marker for early-onset neonatal infection. J Pediatr 132: 445–451
Remington JS, Klein JO 1995 Current concepts of infections of the fetus and newborn infant. In: Remington JS, Klein JO (eds) Infectious Disease of the Fetus and Newborn Infants. Philadelphia, PA, WB Saunders, pp 1–19
van de Winkel JG, Anderson CL 1991 Biology of human immunoglobulin G Fc receptors. J Leukoc Biol 49: 511–524
de Haas M, Vossebeld PJ, Von dem Borne AE, Roos D 1995 Fc gamma receptors of phagocytes. J Lab Clin Med 126: 330–341
Rascu A, Repp R, Westerdaal NA, Kalden JR, Van de Winkel JG 1997 Clinical relevance of Fc gamma receptor polymorphisms. Ann NY Acad Sci 815: 282–295
Fjaertoft G, Håkansson L, Ewald U, Foucard T, Venge P 1999 Neutrophils from term and preterm newborn infants express the high affinity Fcγ-receptor I (CD64) during bacterial infections. Pediatr Res 45: 871–876
Ng PC, Li K, Wong RP, Chui KM, Wong E, Fok TF 2002 Neutrophil CD64 expression: a sensitive diagnostic marker for late-onset nosocomial infection in very low birth weight infants. Pediatr Res 51: 296–303
Layseca-Espinosa E, Pérez-González LF, Torres-Montes A, Baranda L, de La Fuente H, Rosenstein Y, González-Amaro R 2002 Expression of CD64 as a potential marker of neonatal sepsis. Pediatr Allergy Immunol 13: 319–327
Walsh MC, Kliegman RM, Fanaroff AA 1988 Necrotizing enterocolitis: a practitioner's prospective. Pediatr Rev 9: 219–226
Iyer SB, Hultin LE, Zawadzki JA, Davis KA, Giorgi JV 1998 Quantitation of CD38 expression using QuantiBRITE beads. Cytometry 33: 206–212
Gratama JW, D'hautcourt JL, Mandy F, Rothe G, Barnett D, Janossy G, Papa S, Schmitz G, Lenkei R 1998 Flow cytometric quantitation of immunofluorescence intensity: problems and perspectives. European Working Group on Clinical Cell Analysis. Cytometry 33: 166–178
Ng PC, Cheng SH, Chui KM, Fok TF, Wong MY, Wong W, Wong RP, Cheung KL 1997 Diagnosis of late onset neonatal sepsis with cytokines, adhesion molecule, and C-reactive protein in preterm very low birthweight infants. Arch Dis Child Fetal Neonatal Ed 77: F221–F227
Ng PC 2004 Diagnostic markers of infection in neonates. Arch Dis Child Fetal Neonatal Ed 89: F229–F235
Brüning T, Daiminger A, Enders G 1997 Diagnostic value of CD45RO expression on circulating T lymphocytes of fetuses and newborn infants with pre-, peri- or early post-natal infections. Clin Exp Immunol 107: 306–311
Hodge S, Hodge G, Flower R, Han P 1998 Surface activation markers of T lymphocytes: role in the detection of infection in neonates. Clin Exp Immunol 113: 33–38
Michie C, Harvey D 1994 Can expression of CD45RO, a T-cell surface molecule, be used to detect congenital infection?. Lancet 343: 1259–1260
Hodge G, Hodge S, Han P, Haslam R 2004 Multiple leucocyte activation markers to detect neonatal infection. Clin Exp Immunol 135: 125–129
Author information
Authors and Affiliations
Additional information
The work described in this paper was supported by a Direct Grant for Research (Project code: 2041069) from the Research Grants Council of Hong Kong.
Rights and permissions
About this article
Cite this article
Ng, P., Li, G., Chui, K. et al. Neutrophil CD64 Is a Sensitive Diagnostic Marker for Early-Onset Neonatal Infection. Pediatr Res 56, 796–803 (2004). https://doi.org/10.1203/01.PDR.0000142586.47798.5E
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.PDR.0000142586.47798.5E
This article is cited by
-
Diagnostics for neonatal sepsis: current approaches and future directions
Pediatric Research (2017)
-
Meta-analysis of diagnostic accuracy of neutrophil CD64 for neonatal sepsis
Italian Journal of Pediatrics (2016)
-
Monocyte HLA-DR expression and neutrophil CD64 expression as biomarkers of infection in critically ill neonates and infants
Pediatric Research (2015)
-
Expression of CD64 on neutrophils can be used to predict the severity of bloodstream infection before broad range 16S rRNA PCR
Folia Microbiologica (2015)
-
Diagnostic and prognostic value of sCD14-ST—presepsin for patients admitted to hospital intensive care unit (ICU)
Wiener klinische Wochenschrift (2015)
