
Abstract
The potential for functional and metabolic recovery in neonatal hearts after the development of ischemic contracture remains controversial and undefined. This study documents postischemic recovery of metabolism and function in the in vivo neonatal heart after the development of onset and peak ischemic contracture. In piglets on cardiopulmonary bypass, hearts were reperfused after the development of either onset (TICo) or peak (TICp) ischemic contracture. Systolic (developed and systolic function, contractility) and diastolic (diastolic function, relaxation) performance was assessed throughout reperfusion. Biopsies were obtained at end-ischemia or end-reperfusion to assess metabolism. By end-ischemia, the metabolic profiles of both TICo and TICp hearts confirmed energy-store depletion and purine degradation that was quantitatively greater in TICp hearts. Hearts reperfused at TICo had consistent moderate impairment of developed function, contractility, diastolic function, and relaxation, whereas hearts reperfused at TICp had much more profound functional impairment. Diastolic function showed the worst functional recovery. In contrast, systolic function was not significantly altered in either study group and, thus, did not reflect the actual extent of injury. In addition, TICo hearts either did not further deplete or partially regenerated energy stores during reperfusion, whereas TICp hearts had further energy-store depletion and lactate accumulation. In summary, neonatal hearts reperfused after TICo maintained or partially restored energy stores and had significant but incomplete functional recovery. In contrast, further metabolic deterioration and profound functional impairment occurred with reperfusion after TICp, potentially indicating ongoing mitochondrial injury and compromised oxidative phosphorylation.
Similar content being viewed by others

Main
Whether the neonatal heart is highly tolerant (1) or susceptible (2) to ischemic injury remains controversial. The TIC model has been used to assess myocardial susceptibility to ischemic injury since such landmark papers as those published by Hearse et al. (3) and Wechsler et al. (4). Ischemic contracture, a marker of ischemic injury (3, 4), was first recognized clinically when some heart surgery patients developed unrecoverable postischemic myocardial dysfunction (5, 6). In adult hearts, ischemic contracture has been shown to occur secondary to mitochondrial injury (7), altered cytosolic Ca2+ levels (8), and a critical loss of ATP at the myofibrils (3, 9) that results in a progressive inability to dissociate actin-myosin cross-bridges (6). Since its recognition and characterization, ischemic contracture has been used as a marker of ischemic tolerance (3, 4). Despite the original interest in the TIC model and its metabolic characterization, the functional consequences of and metabolic recovery from ischemic contracture have not been extensively investigated. Doubt has emerged regarding the relevance of TIC in immature hearts (10). As well, the potential for both metabolic and functional recovery with reperfusion after the development of ischemic contracture in neonates has not been fully elucidated. To address these issues, the present study compares and contrasts postischemic recovery of myocardial metabolism and function with reperfusion after the development of onset and peak ischemic contracture in the in vivo neonatal heart.
METHODS
Preparation.
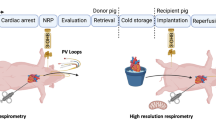
In preparation for placement on CPB (11), neonatal male Yorkshire pigs (3 d old, n = 32) were anesthetized with an intraperitoneal injection of sodium pentobarbital (65 mg/kg). Animals were then intubated and ventilated with medical air. One catheter was inserted into the right carotid artery and advanced to the aortic arch to monitor arterial blood pressure. A second catheter was inserted into the right jugular vein and advanced to the superior vena cava to monitor central venous pressure. These catheters were connected to pressure transducers (COBE, Lakewood, CO, U.S.A.) and a physiologic recorder (BIOPAC Systems, Inc., Goleta, CA, U.S.A.). Arterial blood samples were obtained and appropriate adjustments were made to ensure normal physiologic values for Po2 and Pco2 as well as bicarbonate and pH (ABL30 Acid-Base Analyzer, Radiometer, Copenhagen, Denmark). After sternotomy, systemic heparinization (heparin sulfate, 400 IU/kg), and aortic and right atrial cannulation, piglets were placed on normoxic (Pao2 = 15.8 ± 0.8 kPa), normothermic (38.3 ± 0.1°C) CPB using a Minimax membrane oxygenator (Medtronic, Anaheim, CA, U.S.A.) and a Sarns 9000 perfusion system (3M SARNS, Ann Arbor, MI, U.S.A.) that was primed with fresh blood. Supplemental sodium pentobarbital was administered via the perfusion circuit to ensure a surgical plane of anesthesia.
Experimental protocol.
After the initiation of CPB, a compliant fluid-filled latex balloon was inserted into the LV and connected to a pressure transducer. Heart rate as well as systolic pressure, diastolic pressure, and developed (systolic-diastolic) pressure were obtained directly from the original pressure trace (Fig. 1A). This pressure trace was differentiated with respect to time; contractility and relaxation were defined as the peak positive deflection (+dP/dtmax) and peak negative deflection (-dP/dtmax), respectively (Fig. 1B). Myocardial performance was assessed by incrementally injecting fluid into the compliant LV balloon to yield a volume-dependent relationship and to generate performance index-versus-volume curves. For all indices except relaxation (developed function, contractility, systolic function, diastolic function), performance was defined as the slope of the linear portion of the index-versus-volume curve (Fig. 1C). Because relaxation was consistent across this physiologic volume range, relaxation was defined as the mean -dP/dtmax value across this volume range. A sample performance index-versus-volume curve is shown from one individual TICo animal (Fig. 2). This varied-volume myocardial performance assessment technique is well accepted in larger animal models and assesses the ability of the heart to respond to a range of volumes, thereby applying the Frank-Starling law of the heart to provide more physiologically relevant information.

For each balloon volume, the original intraventricular pressure trace (A) yielded pressure values; the first derivative of this trace with respect to time (B) yielded peak maximum (+dP/dtmax) and peak minimum (-dP/dtmax) contractility and relaxation, respectively. For each function assessment, fluid was injected into the balloon to progressively increase the balloon volume, thus generating performance index-vs-volume curves (C). Myocardial function was defined as the slope of the linear portion of the index-vs-volume curve.

Sample developed pressure-vs-volume curves for one TICo heart. In addition to three baseline curves (•), pressure-volume curves are also shown for 15 (▪), 30 (▴), and 60 (▾) min of reperfusion. Although the entire volume range is shown, the slope values are calculated from the linear portion of the range between the dotted lines.
Preischemic baseline myocardial performance was obtained for all hearts. After confirming stability, global myocardial ischemia was initiated with placement of an AXC. Immediately after AXC, the LV balloon was filled to generate a pressure of 10 mm Hg. As the duration of ischemia increased, the pressure in the LV balloon gradually increased, and ischemic contracture onset was defined as a 2-mm Hg pressure increase, whereas peak ischemic contracture was defined as the pressure plateau. This is a standard technique to assess the development of ischemic contracture (2). The TICo or TICp was measured and recorded for each heart. Due to the potentially deleterious effect of LV biopsies on both coronary perfusion and myocardial function in a neonatal heart model, a biopsy was taken immediately after the development of onset or peak ischemic contracture (end-ischemia) in one subset of hearts (n = 16). This biopsy was used to assess the metabolic status at onset or peak ischemic contracture and, thus, determines the metabolic effects of ischemia alone. Postischemic functional recovery could not be assessed in these hearts. In all other hearts (n = 16), after reaching either onset or peak ischemic contracture, the fluid was withdrawn from the balloon, the AXC removed, and reperfusion initiated. Reperfusion was confirmed by distension of the main coronary arteries with arterial blood together with the return of normal arterialized color to the myocardium. One TICp heart was excluded from the study due to unsuccessful reperfusion as documented by the lack of coronary distension and an absent LV pressure waveform and confirmed by extremely high diffusible end-product levels (lactate, 157.5 μmol/g; hypoxanthine, 4.1 μmol/g) at end-reperfusion. In all other animals, postischemic myocardial function was assessed at 15, 30, and 60 min of reperfusion, and a biopsy was obtained at end-reperfusion to determine the combined metabolic effects of ischemia/reperfusion.
After obtaining the LV biopsy at either end-ischemia or end-reperfusion, CPB was terminated and animals were euthanized by pentobarbital overdose. All experimental procedures and protocols used in this investigation were reviewed and approved by the University of Toronto Animal Care and Use Committee and are in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals (National Institutes of Health publication No 85–23, revised 1985) and Canadian Council on Animal Care guidelines.
Myocardial metabolism.
Full-thickness freeze-clamp LV free-wall biopsies (12) were immediately immersed in liquid nitrogen, freeze-dried, and stored at −86°C for subsequent analysis. Adenine nucleotides (ATP, ADP, AMP) and nucleosides (hypoxanthine, xanthine, IMP, inosine), pyridine nucleotides (NAD, NADP), and CP were analyzed according to HPLC methods modified by Hull-Ryde et al. (13). Myocardial glycogen and lactate were determined by enzymatic analysis (14, 15). TAN (ATP + ADP + AMP) content was also calculated. Metabolites are expressed as μmol/g dry weight.
Data analysis.
In both study groups, each myocardial performance index was obtained at preischemia and at 15, 30, and 60 min of reperfusion. Analysis was via univariate repeated-measures ANOVA with Duncan's multiple range test post hoc. Group differences in ischemic time and metabolites at end-reperfusion were analyzed by t test. For statistical analyses, calculations were performed on the absolute data, and significance was accepted at p < 0.05. All values are expressed as mean ± SEM.
RESULTS
Myocardial metabolism at end-ischemia.
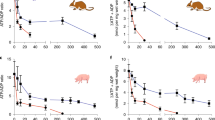
In the two study groups, the TICo and TICp were 30.5 ± 1.9 and 46.0 ± 4.0 min, respectively (p = 0.04). At end-ischemia, both study groups had reduced myocardial energy stores with quantitatively greater reductions at peak than onset ischemic contracture. Additionally, ischemia had a quantitatively different impact on the various metabolites. Specifically, both study groups had the least reductions in ATP (Fig. 3A; TICp, 46 ± 11%, TICo, 13 ± 6%) and greater reductions in CP (Fig. 3B; TICp, 58 ± 4%, TICo, 55 ± 9%) and glycogen (Fig. 3C; TICp, 78 ± 8%, TICo, 64 ± 7%). Interestingly, TAN levels decreased 17% in TICp hearts (22.0 ± 4.0 μmol/g) but remained at baseline levels in TICo hearts (27.0 ± 2.5 μmol/g).

In vivo neonatal myocardial energy stores after the development of onset (solid) or peak (hatch) ischemic contracture at end-ischemia (left) and end-reperfusion (right). Values are mean ± SEM (μmol/g dry weight). Values at end-ischemia are shown for ATP (A), CP (B), and glycogen (C). Values at end-reperfusion are shown for ATP (D), CP (E), and glycogen (F). Normal physiologic values (dotted line) and specific statistical differences at end-reperfusion between onset and peak groups are shown.
Myocardial metabolism at end-reperfusion.
By end-reperfusion, compared with the levels obtained at end-ischemia, myocardial energy levels were either unaltered or partially restored in the TICo group, whereas those in the TICp group were either unchanged or further reduced. Specifically, at end-reperfusion, the ATP level in the TICo hearts remained 23 ± 5% below baseline values but was still 4.1-fold higher than the 81 ± 10% reduction observed in TICp hearts (Fig. 3D). In contrast, CP levels in the TICo hearts recovered to baseline (Fig. 3E). This value was 10.3-fold greater than that seen in the TICp hearts in which CP actually declined further and was 90 ± 9% below baseline by end-reperfusion. At end-reperfusion, glycogen in the TICo group partially recovered to 25 ± 8% below baseline but remained 68 ± 21% below baseline in TICp hearts (Fig. 3F). Despite these differences, large variability in the TICp group prevented statistical significance. Overall, this profile indicates that TICo hearts had much higher myocardial energy stores than TICp hearts by end-reperfusion. In addition, the myocardial pyridine nucleotides at end-reperfusion were significantly higher in TICo hearts with 2.4-fold higher NAD (Fig. 4A;p = 0.01), which approached that seen at baseline, and 2-fold higher NADP (Fig. 4B;p = 0.02).

In vivo neonatal myocardial reducing equivalents at end-reperfusion after the development of onset (solid) or peak (hatch) ischemic contracture. Values are mean ± SEM (μmol/g dry weight). Values are shown for NAD (A) and NADP (B). Normal physiologic values (dotted line) and specific statistical differences between onset and peak groups are shown.
In contrast, glycolytic and purine degradation product levels at end-reperfusion were generally higher in the TICp than TICo hearts (Table 1). Specifically, lactate levels at end-reperfusion were 2.4-fold higher in TICp hearts (p = 0.0005), and both groups remained elevated from baseline (TICo, 60 ± 32%versus TICp, 276 ± 1%). In addition, ADP and AMP remained over 40% reduced from baseline in both groups with the TICp hearts having 36% lower ADP levels (p = 0.001) and 1.8-fold higher AMP levels. As a result, compared with baseline, TAN levels at end-reperfusion were reduced 30% in TICo and 76% in TICp hearts. Although the diffusible purine degradation products were generally higher in the TICp group, only the 1.7-fold higher hypoxanthine levels achieved statistical significance (p = 0.02), whereas the 2.4-fold higher IMP yielded a statistical trend (p = 0.08).
Postischemic myocardial function.
Throughout the study, heart rate was not significantly altered in either study group (p = 0.70), with values of 201 ± 8 beats/min at preischemia and 182 ± 6 beats/min throughout reperfusion. Absolute values, including baseline, are shown for all systolic performance parameters (Fig. 5). The overall ANOVA statistics for the systolic performance parameters indicate that for all but systolic function, the TICo and TICp groups exhibit significantly different functional recovery with ischemia/reperfusion [developed function (p < 0.0001), contractility (p < 0.0001), systolic function (p = 0.13)]. Specifically, developed function during reperfusion is shown in Figure 5A. In the TICo group, developed function was depressed 32 ± 8% (p = 0.0004) at 15 min and remained 36 ± 12% (p < 0.0001) depressed by 60 min of reperfusion. In contrast, there was significantly worse recovery of developed function after TICp. Specifically, developed function in the TICp group was depressed by 72 ± 7% (p < 0.0001) at 15 min and thereafter remained over 80% depressed (p < 0.0001). Contractility during reperfusion in the TICo and TICp groups is shown in Figure 5B. In the TICo group, contractility was depressed 36 ± 11% (p < 0.0001) at 15 min and did not improve during reperfusion. In contrast, contractility in the TICp group was reduced over 95% (p < 0.0001) throughout the reperfusion period. Systolic function is shown in Figure 5C. The overall ANOVA indicated that systolic function was not significantly altered after ischemia/reperfusion (p = 0.13) in either TICo or TICp hearts.

Postischemic systolic performance parameters with reperfusion after the development of onset (solid) or peak (hatch) ischemic contracture. Profiles are shown for developed function (A), contractility (B), and systolic function (C) at 15, 30, and 60 min of reperfusion. The overall ANOVA statistic and baseline preischemic mean (dotted line) are also shown. Values are mean ± SEM. Post hoc analysis yielded statistically significant differences from baseline; *p < 0.0001; †p < 0.0005; §p < 0.005.
Absolute values for all diastolic performance parameters are shown in Figure 6. The overall ANOVA statistics for the diastolic performance parameters indicate that the TICo and TICp groups had significantly different postischemic functional recovery [diastolic function (p < 0.0001), relaxation (p = 0.004)]. Specifically, diastolic function during reperfusion is shown in Figure 6A. For this parameter, an increase indicates impaired diastolic function. In the TICo group, diastolic function increased over 80% (p < 0.05) during initial reperfusion and was sustained at this level throughout reperfusion. Diastolic function in the TICp group increased by 3500–4500% (p < 0.0001) throughout the reperfusion period, thus confirming significantly worse diastolic function in TICp hearts than TICo hearts (p < 0.0001). Relaxation during reperfusion in the TICo and TICp groups is shown in Figure 6B. In the TICo group, relaxation was depressed 33 ± 9% (p < 0.0001) at 15 min and did not improve throughout reperfusion. In contrast, relaxation in the TICp group was reduced over 80% (p < 0.0001) throughout the reperfusion period.

Postischemic recovery of diastolic performance parameters with reperfusion after the development of onset (solid) or peak (hatch) ischemic contracture. Profiles are shown for diastolic function (A) and relaxation (B) at 15, 30, and 60 min of reperfusion. The overall ANOVA statistic and baseline preischemic mean (dotted line) are also shown. Values are mean ± SEM. Post hoc analysis yielded statistically significant differences from baseline; *p < 0.0001; †p < 0.0005, ‡p < 0.05 and from the TICo group; ¶p < 0.0001.
DISCUSSION
For the first time, this study quantifies metabolic and functional recovery in neonatal hearts with reperfusion after the development of onset and peak ischemic contracture. Neonatal hearts reperfused after ischemic contracture onset had no further reduction or even partially restored energy stores and slight to moderate reductions in both contractile and diastolic performance. This partial metabolic recovery in individual hearts was consistent with the extent of postischemic functional recovery. In contrast, hearts reperfused after peak ischemic contracture had further reduced energy stores and profound systolic and diastolic dysfunction. Thus, this study documents the extent of postischemic metabolic and functional recovery and definitively disproves the belief that there would be sufficient metabolic and functional recovery to support the circulation in neonatal hearts reperfused after peak ischemic contracture.
Stone heart was first recognized clinically when some heart surgery patients (5, 6) had severely compromised postischemic heart function with reperfusion. This occurred due to an increase in diastolic stiffness (3, 5) that was initiated during ischemia and was exacerbated with reperfusion. In the current study, the greater impairment in diastolic function also confirms the importance of diastolic stiffness in the neonatal heart. Ischemic contracture occurs secondary to a critical loss of ATP at the myofibrils (3, 9), which results in a progressive inability to dissociate actin-myosin cross-bridges (6) and ultimately increases diastolic stiffness (3, 5). Since its recognition and characterization, ischemic contracture has been used as a useful marker of ischemic tolerance (3, 4), and the TIC model has been used as an index of susceptibility to global ischemic injury (3, 5). By use of this model, ischemic damage can be estimated by determining both TICo and TICp. Ischemic contracture onset marks the beginning of rigor complex formation, is characterized by combined reversible and irreversible injury, and is supported by the moderate functional recovery documented in this study. In contrast, peak contracture represents maximal rigor complex formation with extensive irreversible injury and was confirmed by the profoundly impaired postischemic functional recovery observed in all TICp hearts. Both initial (3) and subsequent research (7, 9, 16, 17) on adult TIC focused extensively on the metabolic correlates of onset and peak contracture. Whereas early studies correlated ischemic contracture with ATP depletion in both adults (7, 9, 18) and newborns (18), more recent studies in adult hearts have identified the cessation of anaerobic glycolysis as the metabolic event that defines the onset of ischemic contracture (17, 19). Despite these metabolic studies, postischemic functional recovery after ischemic contracture in the neonatal heart has not been extensively examined. In particular, some researchers contend that immature hearts will exhibit substantial functional recovery even with reperfusion after TICp. In contrast, the current study shows that neonatal hearts reperfused at TICp had negligible postischemic recovery of most performance indices in addition to severe metabolic compromise.
Traditionally, studies of postischemic functional recovery have used fixed durations of ischemia and, thus, could not provide a direct link between the metabolic events identified in TIC studies and postischemic functional recovery. For example, one study examined ischemic contracture in neonatal hearts but documented TIC in one set of hearts and functional recovery in another set of hearts exposed to fixed durations of ischemia (10). As a result, this study did not examine postischemic functional recovery after the development of ischemic contracture. In fact, because TIC is normally distributed for both adult (16) and newborn (10) hearts, extrapolation of fixed duration data to ischemic contracture should be viewed with caution. The current study confirmed this concern because TICp in some hearts occurred after a shorter duration of ischemia than TICo in other hearts. Thus, the potential for functional recovery after ischemic contracture can only be evaluated in individual hearts reperfused after the development of ischemic contracture. The current study measured TICo or TICp and then evaluated functional recovery in the same heart, thus permitting a direct evaluation of functional recovery after the development of onset or peak ischemic contracture.
Myocardial Metabolism
Metabolism during ischemia.
At end-ischemia, the metabolic profiles for both the TICo and TICp hearts are consistent with impaired oxidative phosphorylation. Specifically, at end-ischemia, TICo hearts had modestly depleted energy stores, whereas TICp hearts had much more extensive energy and purine nucleotide depletion. Additionally, the inhibition of glycolysis and the concomitant cessation of glycolytic ATP production have been identified as the metabolic events that define ischemic contracture onset (17, 19). Because myocardial glycogen is the only glycolytic substrate available during global ischemia, only a significant reduction in glycogen between onset and peak ischemic contracture would indicate ongoing glycolysis. In this experiment, the similar glycogen levels in TICo and TICp hearts at end-ischemia, despite more profound ATP depletion in TICp hearts, confirms that the cessation of glycolysis also marks ischemic contracture onset in neonatal hearts.
Metabolism during reperfusion.
The extent of metabolite depletion during ischemia and the ability to regenerate metabolites during reperfusion both contribute to the myocardial metabolite levels at end-reperfusion. Onset and peak hearts had very different metabolic profiles by end-reperfusion. Specifically, at end-reperfusion, the TICo hearts fully restored CP and partially restored glycogen but had no further significant reduction in ATP and moderately reduced TAN. This could imply that despite the inability to restore ATP to baseline levels, hearts reperfused at TICo regained sufficient mitochondrial function to satisfy their immediate cellular energy requirements. In contrast, even by end-reperfusion, the TICp hearts did not improve their end-ischemic glycogen levels and had additional moderate CP and ATP reductions with profoundly reduced TAN, consistent with profoundly impaired oxidative phosphorylation and extensive mitochondrial injury. In addition, the elevated diffusible purine nucleoside and lactate levels in TICp hearts suggest that tissue end-product removal was impaired.
The oxidative intermediate profile (NAD, NADP) provides information about cellular reducing equivalents and can also be used to assess metabolic recovery from ischemic contracture. Cytosolic NAD indicates the relative rates of glycolysis and oxidative phosphorylation (20) and is, thus, a marker of cellular energy levels. In TICo hearts, NAD either returned to baseline levels or remained slightly depressed, indicating a modest effect on mitochondrial function. In contrast, the significantly reduced NAD in TICp compared with TICo hearts confirms that mitochondrial function and, thus, oxidative phosphorylation in the TICp hearts were profoundly impaired. Although the supply of reducing equivalents is independent from energy production, NADPH provides a means to shunt reducing equivalents to defend against oxidative stress, thus further compromising cellular energy levels (21). The significantly lower NADP levels in TICp hearts indicate that not only is the supply of reducing equivalents for energy production impaired but also the ability to defend against oxidative injury (22) is likely impaired, potentially further compromising postischemic performance in these neonatal hearts.
Myocardial Function
Systolic performance.
This study found that both TICo and TICp hearts had impaired developed function and contractility, which were quantitatively worse in hearts reperfused at TICp. Interestingly, systolic function was not significantly impaired in either study group. Developed function and contractility depend on many common factors such as troponin C Ca2+ affinity (23, 24) and myofilament Ca2+ sensitivity (25, 26–28), which regulate the cross-bridges (29). The consistent 35% impairment of both developed function and contractility in the TICo hearts throughout reperfusion is in keeping with the fact that they depend on these common mechanisms. However, contractility also depends extensively on the myosin ATPase activity (30) and SR Ca2+ handling (28), both of which are highly dependent on ATP supply and are adversely affected by acidosis. Within the TICo group, ATP was only minimally reduced, thus indicating that these mechanisms were likely not significantly impaired. This resulted in similar recovery of developed function and contractility, consistent with the observed metabolic recovery in TICo hearts.
In contrast, the TICp hearts had profoundly reduced ATP levels and severe lactate accumulation at end-reperfusion, likely indicating compromised mitochondrial function, impaired cellular perfusion, and tissue acidosis that would contribute to the quantitatively worse recovery of developed pressure and contractility. In addition to impairment of other cellular mechanisms, these hearts likely had severely impaired myosin ATPase activity that would have contributed to the quantitatively greater impairment of contractility than developed function (95 versus 80%) in these TICp hearts. The minimal recovery of TICp hearts in the current study suggests that neonatal hearts reperfused after the development of peak ischemic contracture exhibit extensive irreversible injury and yield a level of function that would be incapable of supporting the circulation.
In contrast, systolic function did not appear to be significantly impaired during reperfusion after the development of either onset or peak ischemic contracture. In fact, systolic function in the TICp hearts actually increased by end-reperfusion. This may mistakenly be interpreted as sustained or even improved systolic function. However, systolic function is the slope of the systolic pressure-versus-volume relationship and, thus, represents the length-dependent aspect of myofilament deactivation at the end of the contractile phase. The TICo hearts maintained systolic function during ischemia/reperfusion, suggesting that the systolic pressure-versus-volume relationship was unaltered. In contrast, systolic function appeared to increase slightly in TICp hearts. Because stiffness is the change in pressure for a given change in volume, these systolic data more likely suggest that, even during contraction, the TICp hearts are stiffer during reperfusion. This was confirmed by the diastolic function data.
Diastolic performance.
This study also found that both TICo and TICp hearts had impaired diastolic function and relaxation that were quantitatively worse in hearts reperfused at TICp. This diastolic injury indicates increased myocardial stiffness, was evident very early during reperfusion, and did not worsen or improve. This myocardial stiffness occurs secondary to greater actin-myosin cross-bridge interactions that are determined largely by the cytosolic Ca2+ levels and regulated by SR and SL Ca2+-ATPases. Interestingly, SR and SL Ca2+-ATPase activity depends on sufficient ATP supply but can also be impaired by acidosis. In the TICo group, the consistently impaired diastolic function throughout reperfusion indicates that Ca2+ influx likely occurred with the initiation of reperfusion but was not progressive. This suggests that mitochondrial function supplied sufficient ATP to maintain SR and SL Ca2+-ATPase function and, thus, maintained relatively stable cytosolic Ca2+ levels throughout reperfusion. In contrast, all TICp hearts had significantly elevated lactate at end-reperfusion, likely with concomitant acidosis, and profound ATP depletion that would severely impair cytosolic Ca2+ transport, increase cytosolic Ca2+ levels, and ultimately yield the diastolic injury observed in these hearts. In addition, some individual TICp hearts had progressively worsening diastolic function, indicating progressively impaired ATP-dependent cytosolic Ca2+ regulation during reperfusion.
Relaxation, the change in -dP/dtmax for a given change in volume, is dependent on the rate of cytosolic Ca2+ decline, which is determined directly by the rate of Ca2+ transport via the SR and SL Ca2+-ATPases. Both TICo and TICp hearts had significantly impaired relaxation, suggesting that oxidative phosphorylation was insufficient to supply adequate ATP for optimal Ca2+-ATPase function. The quantitatively worse relaxation in the TICp hearts, 80% impairment versus only 33% in TICo, is consistent with the profoundly impaired oxidative phosphorylation and extensively reduced myocardial energy stores observed in TICp hearts at end-reperfusion.
Metabolism versus Function
Within the TICo group as well as between the TICo and TICp groups, the metabolic profiles are consistent with the observed differences in functional recovery. For example, one TICo heart exhibited 115% recovery of developed function, whereas another TICo heart had only 49% recovery. These two hearts had the same lactate and glycogen levels, but the heart with better recovery had 49% higher ATP, 194% higher CP, 96% higher NADP, and 38% higher NAD. This confirms that both high-energy phosphate and reducing equivalent levels are associated with function recovery in the neonatal heart. These profiles are also consistent with the clinical (31) and experimental (32) observation that depletion of myocardial energy stores predisposes neonatal hearts to impaired postischemic functional recovery.
Summary
This study identified that neonatal hearts subjected to ischemic contracture onset had reduced metabolites during ischemia but had no further reduction or partially restored energy stores during reperfusion and slight to moderate reductions in overall myocardial function. In contrast, reperfusion after peak ischemic contracture further reduced ATP and CP and resulted in profoundly impaired myocardial function. Surprisingly, systolic function did not reflect these metabolic and functional responses and, therefore, is not a useful marker of injury in the neonatal heart. On the basis of all other functional indices examined, reperfusion after ischemic contracture onset would yield cardiac outputs sufficient to support the circulation, whereas reperfusion after peak ischemic contracture in the in vivo neonatal heart would be incompatible with life.
Abbreviations
- AXC:
-
aortic cross-clamp
- CP:
-
creatine phosphate
- CPB:
-
cardiopulmonary bypass
- +dP/dtmax:
-
contractility
- -dP/dtmax:
-
relaxation
- IMP:
-
inosine monophosphate
- LV:
-
left ventricle
- Pao2:
-
partial pressure of oxygen
- SL:
-
sarcolemma
- SR:
-
sarcoplasmic reticulum
- TAN:
-
total adenine nucleotides
- TIC:
-
time to ischemic contracture
- TICo:
-
time to ischemic contracture onset
- TICp:
-
time to peak ischemic contracture
References
Bove EL, Stammers AH 1986 Recovery of left ventricular function after hypothermic global ischemia. J Thorac Cardiovasc Surg 91: 115–122.
Wittnich C, Peniston C, Ianuzzo D, Abel JG, Salerno TA 1987 Relative vulnerability of neonatal and adult hearts to ischemic injury. Circulation 76:V156–V160.
Hearse DJ, Garlick PB, Humphrey SM 1977 Ischemic contracture of the myocardium: mechanisms and prevention. Am J Cardiol 39: 986–993.
Peyton RB, van Trigt P, Pellom GL, Jones RN, Sink JD, Wechsler AS 1982 Improved tolerance to ischemia in hypertrophied myocardium by pre-ischemic enhancement of adenine triphosphate. J Thorac Cardiovasc Surg 84: 11–15.
Cooley DA, Reul GJ, Wukasch DC 1972 Ischemic contracture of the heart: “stone heart. Am J Cardiol 29: 575–577.
Katz AM, Tada M 1972 The “stone heart. Am J Cardiol 29: 578–580.
Sink JD, Currie WD, Pellom GL, Hill RC, Chitwood WR, Wechsler AS 1980 Correlation of mitochondrial function and ischemic contracture. J Thorac Cardiovasc Surg 79: 570–578.
Nayler WG 1981 The role of calcium in the ischemic myocardium. Am J Pathol 102: 262–270.
Koretsune Y, Marban E 1990 Mechanism of ischemic contracture in ferret hearts: relative roles of [Ca2+]i elevation and ATP depletion. Am J Physiol 258:H9–H16.
Quantz M, Tchervenkov C, Chiu RCJ 1992 Unique responses of immature hearts to ischemia: functional recovery versus initiation of contracture. J Thorac Cardiovasc Surg 103: 927–935.
Ihnken K, Morita K, Buckberg GD, Ihnken O, Winkelmann B, Sherman M 1997 Prevention of reoxygenation injury in hypoxemic immature hearts by priming the extracorporeal circuit with antioxidants. Cardiovasc Surg 5: 608–619.
Belanger MP, Torrance SM, Panos A, Wittnich C 1992 Multiple in vivo full-thickness myocardial biopsies by freeze-clamping. J Invest Surg 5: 143–147.
Hull-Ryde EA, Lewis WR, Veronee CD, Lowe JE 1986 Simple step gradient elution of the major high-energy compounds and their catabolites in cardiac muscle using high-performance-liquid-chromatography. J Chromatog 377: 165–174.
Passonneau JV, Lowry OH 1993 Enzymatic Analysis. A Practical Guide. Humana Press Inc, Totowa, NJ, 105–110.
Lowry OH, Passonneau JV 1972 Flexible System of Enzymatic Analysis. Academic Press, New York, 120–218.
Jones RN, Attarian DE, Currie WD, Olsen CO, Hill RC, Sink JD, Wechsler AS 1981 Metabolic deterioration during global ischemia as a function of time in the intact normal dog heart. J Thorac Cardiovasc Surg 81: 264–273.
Kingsley PB, Sako EY, Yang MQ, Zimmer SD, Ugurbil K, Foker JE, From AHL 1991 Ischemic contracture begins when anaerobic glycolysis stops: a 31P-NMR study of isolated rat hearts. Am J Physiol 261:H469–H478.
Jarmakani JM, Nagatomo T, Langer GA 1978 The effect of calcium and high-energy phosphate compounds on myocardial contracture in the newborn and adult rabbit. J Mol Cell Cardiol 10: 1017–1029.
Vanoverschelde JLJ, Janier MF, Bakke JE, Marshall DR, Bergmann SR 1994 Rate of glycolysis during ischemia determines extent of ischemic injury and functional recovery after reperfusion. Am J Physiol 267:H1785–H1794.
Lee AC, Xu X, Colombini M 1996 The role of pyridine dinucleotides in regulating the permeability of the mitochondrial outer membrane. J Biol Chem 271: 26724–26731.
Kehrer JP, Lund LG 1994 Cellular reducing equivalents and oxidative stress. Free Radic Biol Med 17: 65–75.
Bolli R 1991 Oxygen-derived free radicals and myocardial reperfusion injury: an overview. Cardiovasc Drugs Ther 5: 249–269.
Endoh M 1998 Changes in intracellular Ca2+ mobilization and Ca2+ sensitization as mechanisms of action of physiological interventions and inotropic agents in intact myocardial cells. Jap Heart J 39: 1–44.
Fuchs F, Wang YP 1997 Length-dependence of actin-myosin interaction in skinned cardiac muscle fibres in rigor. J Mol Cell Cardiol 29: 3267–3274.
Babu A, Sonnenblick EH, Gulati J 1988 Molecular basis for the influence of muscle length on myocardial performance. Science 240: 74–76.
Allen DG, Kentish JC 1985 The cellular basis of the length-tension relation in cardiac muscle. J Mol Cell Cardiol 17: 821–840.
Lakatta EG 1987 Starling's law of the heart is explained by an intimate interaction of muscle length and myofilament calcium activation. J Am Coll Cardiol 10: 1157–1164.
Pieske B, Schlotthauer K, Schattman J, Beyersdorf F, Martin J, Just H, Hasenfuss G 1997 Ca2+-dependent and Ca2+-independent regulation of contractility in isolated human myocardium. Basic Res Cardiol 92: 75–86.
Winegard S 1984 Regulation of cardiac contractile proteins. Circ Res 55: 566–574.
Roos KP 1997 Mechanics and force production. In: Langer GA (ed) The Myocardium. Academic Press, San Diego, CA, 235–323.
Hammon JW, Graham TP, Boucek RJ, Parrish MD, Merrill WH, Bender HW 1987 Myocardial adenosine triphosphate content as a measure of metabolic and functional myocardial protection in children undergoing cardiac operation. Ann Thorac Surg 44: 467–470.
Wittnich C, Maitland A, Vincente W, Salerno T 1991 Not all neonatal hearts are equally protected from ischemic damage during hypothermia. Ann Thorac Surg 52: 1000–1004.
Acknowledgements
The authors thank Dr. P. St. Louis, Ph.D. (clinical chemist), Department of Clinical Biochemistry, The Hospital for Sick Children (Toronto) and C.E. Carlyle for their technical assistance, and M. Libin for his contributions. This work was made possible by 3M SARNS generous loan of the Sarns 9000 perfusion system, and we acknowledge Bach Simpson Ltd. and Ethicon Ltd. for their contributions.
Author information
Authors and Affiliations
Additional information
Supported by Grant No. T2454 from the Heart and Stroke Foundation of Ontario. S.M.T. was supported by a Research Fellowship from the Ontario Ministry of Health.
Rights and permissions
About this article
Cite this article
Torrance, S., Belanger, M., Wallen, W. et al. Metabolic and Functional Response of Neonatal Pig Hearts to the Development of Ischemic Contracture: Is Recovery Possible?. Pediatr Res 48, 191–199 (2000). https://doi.org/10.1203/00006450-200008000-00012
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-200008000-00012
This article is cited by
-
Myocardial histology and outcome after cardiopulmonary bypass of neonatal piglets
Journal of Cardiothoracic Surgery (2015)
-
Myocardial contractile function in survived neonatal piglets after cardiopulmonary bypass
Journal of Cardiothoracic Surgery (2010)
-
Recovery of the Chronically Hypoxic Young Rabbit Heart Reperfused Following No-Flow Ischemia
Pediatric Cardiology (2006)
