
Abstract
Children born preterm and of very low birth weight have an increased incidence of learning difficulties, but little is known about the specific nature of their cognitive deficits and the underlying neuropathology. We hypothesized that their vulnerability to hypoxic, metabolic, and nutritional insults would lead to reduced hippocampal volumes and to deficits in memory because of the role of the hippocampus in this domain of cognition. Neuropsychological and magnetic resonance imaging methods were used to investigate this hypothesis in adolescents born preterm (≤30 wk gestation, n = 11) or full-term (n = 8). The preterm group had significantly smaller hippocampal volumes bilaterally, despite equivalent head size, and showed specific deficits in certain aspects of everyday memory, both on objective testing and as indicated by parental questionnaires. The preterm group also had a specific deficit in numeracy. The reduced hippocampal volumes and deficits in everyday memory have previously been unrecognized, but their prevalence in a group of neurologically normal children is striking.
Similar content being viewed by others
Main
There have been many reports of cognitive and learning difficulties in children born preterm at VLBW (1). Most studies have focused on assessment of intelligence and academic attainments, with few investigating the more selective impairments that may underlie these broader cognitive deficits (2–4). Although there have been reports of cerebral abnormalities in the preterm brain on the basis of autopsy and, more recently, neuroimaging studies (5–8), there have been few attempts to explore the association between such abnormalities and specific cognitive impairments.
The hippocampus is a structure known to be susceptible to damage in preterm infants; Fuller et al. (9) reported that 67% of their sample of preterm infant brains showed hippocampal abnormalities at autopsy. The hippocampus, both in animals and humans, is known to be selectively vulnerable to a wide variety of neurologic insults, including hypoxic-ischemic injury (10–12), hypoglycemia (13), undernutrition (14), and hypothyroidism (15). Because preterm infants, particularly those of VLBW, are liable to suffer from a variety of hypoxic, metabolic, and nutritional insults, a high incidence of hippocampal abnormality might be predicted in this population.
If some preterm babies were to suffer hippocampal pathologic injury, what implications might this have for the subsequent development of their cognitive function? Inasmuch as the hippocampus plays a special role in cognitive memory, both in animals and humans (16), abnormalities in this structure should be associated with memory impairments. Neuroimaging studies in a variety of adult populations, including the normal elderly (17, 18), the elderly with Alzheimer's disease (19), and patients with amnesia (20), have all demonstrated memory impairments in conjunction with decreases in hippocampal volume. Such studies in the pediatric population are few. Rose and Feldman (2) reported poorer performance by 11-y-old preterm children compared with a full-term group on a variety of memory tasks; this was related to the presence and severity of respiratory distress syndrome. They speculated that insult to the vulnerable hippocampus had occurred, but they had no supporting data. A recent report by Vargha-Khadem et al. (21) provided strong support for the view that the hippocampus is particularly important in subserving episodic memory, the memory for events experienced by an individual. They described a dissociation between episodic memory and semantic memory (memory for facts) in three children with severe bilateral hippocampal atrophy; all showed profound difficulties in episodic memory but relatively preserved semantic memory as shown by tests of intelligence, language, and academic attainment. Memory deficits were demonstrated on both laboratory-based tasks and, strikingly, measures of everyday memory function.
Therefore, given the expected high incidence of hippocampal abnormality in children born at VLBW, we hypothesized that they would have deficits in memory, particularly in episodic compared with semantic memory. To test this hypothesis, we investigated memory function and hippocampal abnormalities using neuropsychological assessment and magnetic resonance techniques in a group of adolescents who had been VLBW babies.
METHODS
Subjects
Subjects were selected from a large cohort of children, born preterm, who had taken part in a randomized feeding trial, between 1982 and 1985, at one of five centers in the United Kingdom (22). Eleven children from this cohort took part in the present study (eight boys and three girls). All were born at <30 wk gestation (median, 28 wks; range, 27–29 wks) and weighed <1500 g at birth (median, 998 g; range, 840-1490 g). None of the infants had recorded intraventricular hemorrhages. All babies had respiratory disease, with eight of the 11 requiring intubation within the first 30 min after birth. The median number of days ventilation for the group was 9 d (range, 7–40 d) and the median number of days in >30% oxygen was 35 d (range, 9–69 d). However, none had evidence of birth asphyxia: none had meconium staining in the liquor and none had an Apgar score of ≤4 at 5 min. Only one baby had a fetal heart rate that dipped below 100, but in this case, the scalp pH was >7.25 and 5-min Apgar score was 6. The children were all described as neurologically normal when examined by a pediatrician in a follow-up study at the age of 7.5–8 y. All attended mainstream schools at the time of the present assessment, and none had a statement of special educational needs, although five had received some learning support in the past.
The control group consisted of eight age-matched children (three boys and five girls) born full-term (median gestation, 39.5 wks; range, 38–41 wks), median birth weight was 3622 g (range, 2717–4754 g), and all had had a normal neonatal course.
At the time of assessment, both groups had a median age of 13 y, 6 mo. All 19 children were right-handed. All children and parents gave informed written consent, and the study was approved by the local hospital and regional ethics committees.
Neuropsychological protocol
An initial 2-h neuropsychological assessment was conducted at the child's home or school, with a second taking place on the same day that the magnetic resonance studies were performed at Great Ormond Street Hospital for Children.
Intelligence.
To establish whether any deficits in memory were independent of reduced intelligence, the WISC-III (23) was administered in full, allowing index scores to be calculated (Verbal Comprehension, Perceptual Organization, Freedom from Distractibility, Processing Speed), in addition to VIQ and PIQ.
Everyday memory.
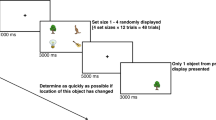
This was the main focus of interest and was measured in two ways. 1) The RBMT (24) had proved sensitive to the everyday memory deficits shown by the amnesic children reported by Vargha-Khadem et al. (21). This test uses activities closer to real life than the usual laboratory-based tasks, while providing an objective measure of everyday memory. A Standardized Profile Score is obtained by assigning a value of 0, 1 or 2 to each of the 12 subtests. 2) A parental questionnaire (25) was used to assess the frequency of different types of everyday memory problems encountered by the child; parents rated each of 28 items from A (has not occurred in the past 3 mo) to I (occurs once a day). Scores of 1 to 9 were assigned to ratings A to I, and these were summed for each child.
Verbal and nonverbal recall.
A series of memory tests commonly used in the laboratory to measure the acquisition and retention of experimental material was given:1) The Wechsler Memory Scale—Form I (26) was administered in the standard way, but with age corrections for children younger than the age of 18 (27). Measures of immediate and delayed recall were obtained for a) logical memory: two prose passages were read for immediate and unalerted recall after a 90-min delay;b) paired-associate learning: 10 pairs of words, six semantically related (e.g. up-down) and four unrelated (e.g. cabbage-pen), were read three times for immediate recall after each presentation and delayed recall after a 90-min delay; and c) visual reproduction: reproduction of geometric designs was obtained immediately after presentation and after a 40-min delay. 2) The CAVLT-2 (28) measures various aspects of verbal memory and learning: immediate memory, level of learning, interference effects, delayed recall, and recognition. A list of 16 words was read to the child five times with free recall after each presentation; to determine the effects of interference, a second 16-word list was read once for immediate recall followed by recall of the original list. 3) The Design Learning subtest of the Adult Memory and Information Processing Battery (29) was administered as a visual analog of the CAVLT-2. A pattern, formed by joining dots in a matrix, was presented for five learning trials; measures analogous to those of the CAVLT-2 were obtained. 4) The Rey-Osterrieth Complex Figure (30), a complicated geometric design, was copied and then recalled after 40 min. 5) Three subtests of the WISC-III (Information, Vocabulary, and Comprehension) were used to assess semantic memory and word knowledge.
Attainment measures.
Tests of attainment in the areas of literacy and numeracy provided additional measures of semantic memory as well as information about the child's level of function in the academic environment:1) All three subtests (Basic Reading, Spelling, and Reading Comprehension) of the WORD test (31) were administered to assess literacy skills. 2) Both subtests (Mathematics Reasoning and Numerical Operations) of the WOND test (32) were given.
The WORD and WOND manuals list the subtest scores that a child with any given WISC-III IQ would be expected to obtain, allowing the comparison of expected and observed values and the statistical evaluation of differences between them.
Magnetic resonance protocol
MRI and MRS studies were performed on a 1.5-tesla Siemens system. Structural MRI investigations included 1) magnetization prepared rapid acquisition gradient echo (33) 3-D volume acquisition with repetition time of 10 ms; echo time, 4 ms; inversion time, 200 ms; flip angle, 12°; matrix size, 256 × 256; field of view, 250 mm; partition thickness, 1.25 mm; 128 sagittal partitions in the third dimension, and acquisition time, 8.3 min; and 2) coronal and axial turbo spin-echo T2-weighted scans with repetition time of 4600 ms; echo time, 90 ms; and acquisition time, 4.3 min for each orientation. The images were reviewed by an experienced pediatric neuroradiologist, blind to the group membership of the children, who recorded the presence of focal, central, or generalized atrophy and abnormalities in the basal ganglia and the hippocampi.
In addition to visual inspection of the structural MRI scans, two quantitative techniques, volumetry and T2 relaxometry, were used for the assessment of hippocampal abnormalities. To measure volumes, the 3-D data sets were reformatted into 1-mm-thick contiguous slices in a tilted coronal plane that was perpendicular to the long axis of the hippocampus. Cross-sectional areas were measured along the entire length of the hippocampi, using every third slice as described previously (34). The volumes were calculated by summing the cross-sectional areas and multiplying by the distance between the measured slices (i.e. 3 mm). Intracranial volumes were measured from the unreformatted sagittal 3-D MRI data sets (34). The hippocampal volumes were then corrected for intracranial volume (34) and are presented here in this corrected form. The volume measurements were made blind to group membership.
T2 relaxometry provides a quantitative way of detecting abnormalities that are more conventionally evaluated by visual inspection of T2-weighted images. Hippocampal water T2 values were obtained from T2 maps constructed from a 16-echo sequence, as previously described (34, 35). The cross-section from which the hippocampal T2 values were taken was oriented in a tilted coronal plane along the anterior border of the brain stem perpendicular to and at the level of the body of the hippocampus. T2 values were measured by placing a region of interest in the largest possible circular area within the hippocampus while avoiding boundaries at which partial volume effects with cerebrospinal fluid may occur.
For the assessment of more diffuse or widespread temporal lobe pathology, 1H MRS data were obtained from 2- × 2- × 2-cm cubes centered on the medial portions of the right and left temporal lobes, using a 90–180-180 spin-echo technique, as described previously (36, 37). The positioning and volume of the selected regions are such that the hippocampi make only a minor contribution to the observed signal intensities, so the 1H MRS findings are essentially reporting on abnormalities that extend beyond the hippocampus. Signal intensities at 2.0 ppm (primarily NAA), 3.0 ppm (Cr), and 3.2 ppm (Cho) were measured from the peak areas by integration. The data are presented in the form of the signal intensity ratio NAA/(Cho + Cr), which provides a simple index of spectral abnormality, with abnormally low values indicative of neuronal loss or damage and/or astrocytosis (36, 37).
Statistics
Because of relatively small groups, with unequal numbers of subjects, and the skewed distribution of some variables, all comparisons between groups were made using nonparametric statistics. Differences between the two groups were evaluated using the Mann-Whitney U test (unrelated samples) or the Wilcoxon Signed Ranks Test (related samples), and correlations were calculated using Kendall's or Spearman's coefficients.
RESULTS
Intelligence
The WISC-III IQ and index score results are shown in Table 1. VIQ differed between the preterm and full-term groups (U = 16.5;p < 0.023), but the median scores of both groups fell within the average range. The difference in PIQ approached significance (U = 22.0;p < 0.068). Neither group showed a significant VIQ − PIQ discrepancy (preterm, Z = −0.311;p < 0.755; full-term, Z = −0.423;p < 0.673). The only index score to show a significant group difference was Freedom from Distractibility (U = 10.5;p < 0.006). Comparisons on the 13 subtest scaled scores showed that the groups differed on two subtests only, those constituting the Freedom from Distractibility Index Score: Digit Span (U = 9.0;p < 0.004) and Arithmetic (U = 10.5;p < 0.005). Digit Span consists of both forward and backward recall; although the preterm group's median score for the backward recall of digits was lower than the score of the full-term group, forward recall was similar in the two groups.
Memory
Verbal and nonverbal recall.
Table 2 presents the results for the laboratory measures of verbal and nonverbal recall, illustrating that most of these did not distinguish between the two groups. The few measures that did show a significant difference between groups were all indices of immediate, rather than delayed, recall. Furthermore, the difference was sometimes caused by an above-average level of performance by the full-term group and not a below-average score in the preterm group.
Everyday memory.
There was a highly significant difference between the preterm and full-term children for scores on the RBMT (Fig. 1 and Table 3). Most children of this age make few errors on this test (maximal score, 24), and, in keeping with this, seven of the eight full-term children had total scores in the Normal range (22–24), six with a maximal score of 24 and one with a score of 22. One full-term child's score of 21 placed him in the Poor Memory Range (17–21). In contrast to this, seven children in the preterm group scored in the Poor Memory range, with two others in the Normal (scores of 22 and 24) and two in the Moderately Impaired (10–16) ranges (scores of 15 and 16). There was a highly significant difference (U = 7.5;p < 0.002) between the scores of the preterm and full-term groups (median scores, 19 and 24, respectively), with little overlap between the two distributions. RBMT scores did not correlate significantly with VIQ (ρ = 0.391;p < 0.098).

Distribution of RBMT scores for the preterm and full-term groups. Individual scores are shown; the height of the bar represents the median value.
For more detailed examination of performance on the RBMT, median scores on the subtests were compared using the Mann-Whitney U test. As shown in Table 3, the three items involving prospective memory (remembering to take a message, remembering to ask a question to each of a verbal cue and a buzzer) were grouped together, as were immediate and delayed route following and immediate and delayed story recall. There were significant differences in performance between the groups on the prospective memory items, on route finding and on orientation, whereas the difference on the date subtest approached significance. Performance on the remaining subtests was similar in both groups. Examination of individual performance by preterm children showed that >50% made errors in following a five-stage route (both immediately after demonstration and in the delayed recall condition), in remembering to carry out prospective tasks, and on questions relating to orientation and date. In contrast, only two children born full-term made errors on any of these items, one on orientation and one on route following.
The difference between the median scores for the two groups on the second measure of everyday memory, namely the parental questionnaire, was not significant when the total scores were compared. It was clear, however, that certain behaviors were reported to occur more frequently in the preterm children than in the full-term. Responses to each item on the questionnaire were therefore compared by Mann-Whitney U tests, and the results are presented in Table 4. Although frequency ratings were higher for the preterm group on all 28 items, seven of the items (the items at the top of Table 4) proved markedly more effective than the remaining 21 in discriminating between the two groups. Median scores for this abbreviated questionnaire (preterm, 19.6; full-term, 8.5) were significantly different (U = 17.5;p < 0.03). Similarities were apparent between the items on this abbreviated questionnaire and the activities that posed difficulties on the RBMT; the correlation between these two sets of scores approached significance (Kendall = −0.30;p < 0.097) and was in the expected negative direction because low scores on the RBMT and high scores on the questionnaire both denote poor everyday memory.
Attainments.
The results of tests of academic attainment are shown in Table 5. There were no significant differences between the groups on any of the measures of the WORD: Basic Reading (single-word accuracy), Spelling, or Reading Comprehension (with no memory requirement). In neither group were the scores significantly lower than those predicted by WISC-III IQ values for any of the three subtests, indicating that development of literacy skills was commensurate with overall intellectual level.
The same was not true, however, of numeracy skills. The preterm group scored significantly lower than the full-term group on both subtests of the WOND: Mathematics Reasoning (orally presented problems to assess mathematical reasoning) and Numerical Operations (written problems assessing calculation ability involving all the basic arithmetic operations). In addition, and unlike the children born full-term, the scores obtained by the preterm group on the Numerical Operations subtest were significantly lower than IQ predictions, i.e. they showed a selective deficit for this aspect of mathematics. A significant discrepancy between expected and obtained scores was shown by six of the 11 children born preterm; although this discrepancy was not statistically significant for the other five (mean, 13.4 points), it was nevertheless larger than in the full-term group (mean, 3.3 points).
Magnetic Resonance
Visual inspection of scans.
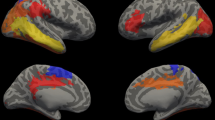
Of the 11 preterm children, only one had an MRI brain scan that was considered to be entirely normal on visual inspection. Four children demonstrated central atrophy in the form of enlargement of the lateral and third ventricles and normal sulcal spaces, and five showed reduced bulk of white matter in the parietooccipital region with a reduction in the size of the body of the corpus callosum. One demonstrated focal atrophy with focal enlargement of a part of a lateral ventricle. Three cases were noted to have small hippocampi, and in all of these, the reductions were bilateral. One child was noted to have signal abnormalities in the basal ganglia; the abnormality was seen in the putamen bilaterally.
Of the eight children born at term, all were judged to have brain scans that were entirely normal.
Quantitative measures.
The quantitative MRI and MRS data are presented in Table 6. Median intracranial volume did not differ significantly between the two groups (U = 36.5;p < 0.536). Occipital-frontal circumference data obtained when the children were seen at 7 y of age confirmed the normality of the preterm group's head size. When compared with reference charts (38), one measurement fell at the second percentile, whereas all others were well within the average range, with half falling at or above the 50th percentile.
Two quantitative magnetic resonance techniques, namely volumetric measurements and T2 relaxometry, were used for the assessment of hippocampal abnormalities. Hippocampal T2 values did not reveal any abnormalities, with no significant difference between the two groups (left, U = 41.5;p < 0.835; right, U = 33.0;p < 0.358). However, there was a highly significant difference between groups for both left and right hippocampal volumes (left, U = 6.0;p < 0.002; right, U = 6.0;p < 0.002), and no hippocampus of a child born preterm was larger than the full-term group median. Because there was no significant difference between left and right hippocampal volumes for either group, a mean hippocampal volume was calculated for each subject. Figure 2 shows the distribution of these measures.

Distribution of mean hippocampal volumes for the preterm and full-term groups. Individual scores are shown; the height of the bar represents the median value.
1H MRS, based on the signals from NAA, Cr, and Cho, was used for the assessment of more-diffuse temporal lobe abnormalities, extending beyond the hippocampus, that can be difficult to visualize on MRI (39). The difference between the group values for the NAA/(Cho + Cr) signal intensity ratios was significant for the right temporal lobe (U = 11.0;p < 0.016), but not for the left (U = 14.5;p < 0.140). However, 17 of the 18 values obtained from the preterm group were above a cut-off point of 0.72 previously used to denote the lower limit of normality (36, 37). Thus, the major group difference as seen on the quantitative magnetic resonance measures is the bilateral reduction in hippocampal volume.
Although both intracranial volume and head circumference measurements obtained at age 7 y indicated that head size was not reduced in the children born preterm, total brain volume could have been reduced in some of these children as a result of the atrophy noted on visual inspection of the scans. If hippocampal volume reduction was secondary to this, then the children who showed atrophy on visual inspection of the MRI scans might be expected to have smaller hippocampi. When hippocampal volumes of the preterm children with atrophy were compared with those of preterm children without atrophy, the difference was not significant for the left hippocampi (U = 8.0;p < 0.257) but was so for the right (U = 0.0;p < 0.008); the group with atrophy, however, had larger left and right hippocampi rather than smaller, indicating that the reduction in hippocampal volume in the preterm group as a whole is not an epiphenomenon of reduced head/brain size.
The atrophy and no-atrophy groups were compared on all other neuropsychological and quantitative magnetic resonance variables to determine whether the presence of atrophy was associated with any specific deficits. The atrophy group had significantly lower scores only on the Picture Completion subtest of the WISC-III (U = 2.0;p < 0.021). In addition, these children had significantly lower median T2 values for both left and right hippocampi (left, U = 0.0;p < 0.007; right, U = 3.0;p < 0.035). However, the latter finding is unlikely to have any functional significance as all four medians were within the average range and pathology tends to be associated with higher, rather than lower, T2 values.
To determine the specificity of hippocampal volume as a predictor of everyday memory performance, the following imaging variables were entered in a stepwise multiple regression with RBMT scores as the dependent variable: mean hippocampal volume, left and right MRS values, and left and right T2 values. Mean hippocampal volume was the only variable that met the criteria for inclusion in the analysis (r2 = 0.45), thus confirming the relationship between hippocampal volume and RBMT scores.
DISCUSSION
The neuropsychological studies reported here reveal that the children who had been VLBW babies showed deficits in everyday memory. A clear differentiation between groups was demonstrated in their scores on the RBMT, which is an objective measure of episodic memory in everyday situations. Such deficits in everyday memory have not previously been recognized in this population.
Several considerations make it unlikely that this deficit in everyday memory is related to impaired cognition, even though VIQ was significantly lower in the preterm compared with the full-term group. The first is their unimpaired performance on a wide variety of other memory measures. Second is the fact that children of this cognitive level (i.e. toward the lower limit of the average range) would not be expected to show deficits on the RBMT (24). Moreover, the correlation between VIQ and RBMT scores was not significant, indicating that the memory impairment is independent of cognitive level.
The memory deficits of the preterm group in this study had characteristics that were both similar to and different from those of the amnesic children reported by Vargha-Khadem et al. (21). Deficits in everyday memory, with relative preservation of most aspects of semantic memory, are consistent with the results of the amnesic children who showed the same pattern after early hippocampal pathology. Vargha-Khadem et al. (21) concluded that the hippocampi, which showed severe atrophy bilaterally in all cases, might have a special role in subserving episodic memory, with subhippocampal cortices mediating the acquisition of semantic memories. The preterm children in the present study also showed reduced hippocampal volumes compared with age matched full-term controls, in conjunction with impairments in everyday memory, although both the volume reductions and memory impairments were far less severe than the deficits observed in the amnesic children.
The preterm group differed from the amnesic children in that they failed, by and large, to show marked deficits on laboratory-based tasks of verbal and nonverbal recall. This may be related to the smaller reductions in hippocampal volumes in the former children. Furthermore, Vargha-Khadem et al. (21) reported abnormally high hippocampal T2 values in the amnesic children, suggesting the presence of pathology in the remaining hippocampal tissue. In contrast, T2 values in the preterm group were normal. It may be, therefore, that the children lie along a continuum of hippocampal abnormality, with the amnesic children showing more-severe memory impairments attributable to the presence of tissue that is abnormal as well as reduced in volume, and this may explain why they show additional deficits that the preterm group does not. It is also possible that some additional memory deficits will be demonstrable when the study group is expanded to include more children.
The memory deficits in the preterm group presented very real difficulties in everyday life; responses to the parental questionnaire identified these, demonstrating that the deficit in RBMT scores is of more than just academic interest. Parents and teachers also described such difficulties during interviews, almost always ascribing these to lack of attention or even naughtiness on the part of the child, with little recognition that a specific memory deficit might be involved. Indeed, problems in attention have been described in preterm children (40, 41), and it is possible that these may coexist and contribute to their impaired performance, particularly on tests of immediate recall. In this respect, it should be noted that the WISC-III Freedom from Distractibility index score was significantly lower for the preterm group compared with the full-term group. The Freedom from Distractibility index, however, consists of the Arithmetic and Digit Span subtests, and because the WOND scores indicate poor mathematical ability in the preterms, low index scores may be reflecting this, particularly inasmuch as the digit span scores were age-appropriate. The lower Freedom from Distractibility index score, therefore, may not be indicative of attentional difficulties per se. It also seems unlikely that problems with attention would produce such a consistent pattern of failed items as seen on the RBMT. Nevertheless, the role of attentional difficulties needs to be addressed, and will be investigated through a larger study that we are now undertaking with the same population.
The striking deficit in mathematics, particularly numerical operations, is in marked contrast to adequate performance on all aspects of literacy. Poor mathematical ability has been reported in follow-up studies of preterm babies in the past (42, 43), so this was not an unexpected finding. Recent research has indicated that areas of both the frontal and parietal lobes (44, 45) may be implicated in mathematics. Our results, however, raise the possibility that a deficit in the spatial ability attributed to the hippocampus (46) may underlie the difficulties with mathematics, because of the spatial component involved in numerical operations.
The hypothesis underlying this study was that deficits in some aspects of episodic memory would be demonstrable in conjunction with reductions in hippocampal volume. The results indicate that this is, in fact, the case. Hippocampal volumes were demonstrably smaller in the preterm children, appearing to be selectively so rather than as a by-product of a general reduction in brain volume. Regression analyses indicated that hippocampal volume was the best predictor of performance on the RBMT. A recent study by Moradi et al. (47) has reported the results of a group of children and adolescents suffering from posttraumatic stress disorder on the RBMT. Interestingly, like our preterm group, these children showed difficulty on the prospective memory items and with orientation; moreover, reductions in hippocampal volume in sufferers of posttraumatic stress disorder have been reported by Bremner et al. (48). However, we cannot preclude the possibility that the impaired memory performance of the preterm group may also be a reflection of additional abnormalities that may be present elsewhere in the brain [for example, in the prefrontal cortex, which is known to play a significant role in episodic memory (49, 50)]. Indeed, we acknowledge the existence of other neural abnormalities when we report the results of visual inspection of the magnetic resonance scans. We plan to undertake voxel-based morphometry studies (51, 52) on our expanded study group to help identify other areas of the brain that may be structurally abnormal. Nevertheless, both the prevalence and magnitude of structural hippocampal abnormalities in our group of neurologically normal children born preterm are striking.
Being born early and very small entails a major risk for developing cognitive difficulties in childhood. Our findings suggest that reduced hippocampal volumes and associated everyday memory deficits may be an important factor in this risk, playing a hitherto unacknowledged role in development. The children in this study had all been small, sick infants who may have been vulnerable to a variety of insults in addition to the respiratory distress syndrome for which they had required ventilation. Determining the causality of the reduced hippocampal volumes awaits the outcome of an investigation with a larger sample of children so that the effects of other variables can be examined. Early nutrition may be of particular importance inasmuch as the children in this study were part of the cohort reported by Lucas et al. (53) to show substantial differences in IQ at age 7–8 y depending on nutritional intervention shortly after birth. Sex may also be an important variable. It proved to be of significance in the study by Lucas et al. (53), and there are reports of interesting sex differences in brain pathology in conditions such as schizophrenia (54) and epilepsy (55). Whichever factor is causal, our observations suggest an important mechanism underlying cognitive compromise in this population of children.
Abbreviations
- CAVLT-2:
-
Children's Auditory-Verbal Learning Test, 2nd edition
- Cho:
-
choline-containing compounds
- Cr:
-
creatine + phosphocreatine
- IQ:
-
intelligence quotient
- MRI:
-
magnetic resonance imaging
- MRS:
-
magnetic resonance spectroscopy
- NAA:
-
N-acetylaspartate
- PIQ:
-
performance IQ, ppm, parts per million
- RBMT:
-
Rivermead Behavioural Memory Test
- VIQ:
-
verbal IQ
- VLBW:
-
very low birth weight
- WISC-III:
-
Wechsler Intelligence Scale for Children, 3rd edition
- WOND:
-
Wechsler Objective Numerical Dimensions
- WORD:
-
Wechsler Objective Reading Dimensions
- 3-D:
-
three dimensional
References
Aylward GP, Pfeiffer SI, Wright A, Verhulst SJ 1989 Outcome studies of low birth weight infants published in the last decade: a meta-analysis. J Pediatr 15: 515–520
Rose SA, Feldman JF 1996 Memory and processing speed in preterm children at eleven years: a comparison with full-terms. Child Dev 67: 2005–2021
Briscoe J, Gathercole S, Marlow N 1998 Short-term memory and language outcomes after extreme prematurity at birth. J Speech Lang Hear Res 41: 654–666
Matthews A, Ellis AE, Nelson CA 1996 Development of preterm and full-term infant ability on AB, recall memory, transparent barrier detour, and means-end tasks. Child Dev 67: 2658–2676
Bouza H, Dubowitz L, Rutherford M, Cowan F, Pennock J 1994 Late magnetic resonance imaging and clinical findings in neonates with unilateral lesions on cranial ultrasound. Dev Med Child Neurol 36: 951–964
Barkovitch AJ, Truwit CL 1990 Brain damage from perinatal asphyxia; correlation of MR findings with gestational age. Am J Neuroradiol 11: 1087–1096
Flodmark O, Lupton B, Li D, Stimac GK, Roland EH, Hill A, Whitfield MF, Norman MG 1989 MR imaging of periventricular leukomalacia in childhood. Am J Roentgenol 152: 583–590
Huppi PS, Schuknect B, Boesch C, Bossi E, Felblinger J, Fusch C, Herschkowitz H 1996 Structural and neurobehavioral delay in postnatal brain development of preterm infants. Pediatr Res 39: 895–901
Fuller PW, Guthrie D, Alvord EC 1983 A proposed neuropathological basis for learning disabilities in children born prematurely. Dev Med Child Neurol 25: 214–231
Kuchna I 1994 Quantitative studies of human newborns' hippocampal pyramidal cells after perinatal hypoxia. Folia Neuropathol 32: 9–16
Volpe JJ 1995 Neurology of the Newborn, 3rd ed. WB Saunders, Philadelphia
Schmidt-Kastner R, Freund TF 1991 Selective vulnerability of the hippocampus in brain ischemia. Neuroscience 40: 599–636
Fujioka M, Okuchi K, Hiramatsu KI, Sakaki T, Sakaguchi S, Ishil Y 1997 Specific changes in human brain after hypoglycemic injury. Stroke 28: 584–587
Katz HB, Davies C, Dobbing J 1982 Effects of undernutrition at different ages early in life and later environmental complexity on parameters of the cerebrum and hippocampus in rats. J Nutr 112: 1362–1368
Madeira MD, Sousa N, Lima-Andrade MT, Calheiros F, Cadete-Leite A, Paula-Barbosa MM 1992 Selective vulnerability of the hippocampal pyramidal neurons to hypothyroidism in male and female rats. J Comp Neurol 322: 501–518
Squire LR 1992 Memory and the hippocampus: a synthesis from findings with rats, monkeys and humans. Psychol Rev 99: 195–231
Golomb J, deLeon MJ, Kluger A, George AE, Tarshshi C, Ferris SH 1993 Hippocampal atrophy in normal ageing. Arch Neurol 50: 967–73
Golomb J, Kluger A, deLeon MJ, Ferris SH, Mittelman M, Cohen J, George AE 1996 Hippocampal formation size predicts declining memory performance in normal ageing. Neurology 47: 810–813
Deweer B, Leheircy S, Pillon B, Baulac M, Chiras J, Marsault C, Agid Y, Dubois B 1995 Memory disorders in probable Alzheimer's disease: the role of hippocampal atrophy as shown with MRI. J Neurol Neurosurg Psychiatry 58: 590–597
Press GA, Amaral DG, Squire LR 1989 Hippocampal abnormalities in amnesic patients revealed by high-resolution magnetic resonance imaging. Nature 341: 54–57
Vargha-Khadem F, Gadian DG, Watkins KE, Connelly A, Van Paesschen W, Mishkin M 1997 Differential effects of early hippocampal pathology on episodic and semantic memory. Science 277: 376–380
Lucas A, Morley R, Cole TJ, Lister G, Leeson-Payne C 1992 Breast milk and subsequent intelligence quotient in children born preterm. Lancet 339: 261–264
Bracken BA ( ed) 1992 Wechsler Intelligence Scale for Children, 3rd ed. The Psychological Corporation, Sidcup, Kent
Wilson B, Cockburn J, Baddeley A 1991 The Rivermead Behavioural Memory Test, 2nd ed. Thames Valley Test Co, Bury St. Edmunds, UK
Sunderland A, Harris JE, Baddley AD 1983 Do laboratory tests predict everyday memory? A neuropsychological study. J Verb Learn Verb Behav 22: 341–357
Wechsler D, Stone CP 1945 Wechsler Memory Scale. Psychological Corporation, San Antonio, TX
Vargha-Khadem F, Isaacs E, Van der Werf S, Robb S, Wilson J 1992 Development of intelligence and memory in children with hemiplegic cerebral palsy. Brain 115: 315–329
Talley JL 1993 Children's Auditory Verbal Learning Test (CAVLT-2). Psychological Assessment Resources, Odessa, FL, USA
Coughlan J, Hollows SE 1985 Adult Memory and Information Processing Battery. St James Hospital, Leeds, UK
Rey A 1964 L'Examen Clinique en Psychologie. Presses Universitaire de France, Paris
Rust J, Golombrok S, Trickey G 1993 Wechsler Objective Reading Dimensions Manual. The Psychological Corporation, London
Rust J 1996 Wechsler Objective Numerical Dimensions Manual. The Psychological Corporation, London
Mugler JP, Brookeman JR 1990 Three-dimensional magnetization-prepared rapid gradient-echo imaging (3D MP RAGE). Magn Reson Med 15: 152–157
Van Paesschen W, Connelly A, King MD, Jackson GD, Duncan JS 1997 The spectrum of hippocampal sclerosis: a quantitative magnetic resonance imaging study. Ann Neurol 41: 41–51
Jackson GD, Connelly A, Duncan JS, Grunewald RA, Gadian DG 1993 Detection of hippocampal pathology in intractable partial epilepsy: increased sensitivity with quantitative magnetic resonance relaxometry. Neurology 43: 1793–1799
Connelly A, Jackson GD, Duncan JS, King MD, Gadian DG 1994 Magnetic resonance spectroscopy in temporal lobe epilepsy. Neurology 44: 1411–1417
Cross JH, Connelly A, Jackson GD, Johnson CL, Neville BGR, Gadian DG 1996 Proton magnetic resonance spectroscopy in children with temporal lobe epilepsy. Ann Neurol 39: 107–113
Buckler JMF 1997 A Reference Manual of Growth and Development, 2nd ed. Blackwell Science, Oxford, pp 25–29
Connelly A, Van Paesschen W, Porter DA, Johnson CL, Duncan JS, Gadian DG 1998 Proton magnetic resonance spectroscopy in MRI-negative temporal lobe epilepsy. Neurology 51: 61–66
Astbury J, Orgill AA, Bajuk B 1987 Relationship between two-year behaviour and neurodevelopmental outcome at five years of very low-birthweight survivors. Dev Med Child Neurol 29: 370–379
Lou HC 1996 Etiology and pathogenesis of attention-deficit hyperactivity disorder (ADHD): significance of prematurity and perinatal hypoxic-haemodynamic encephalopathy. Acta Paediatr 85: 1266–1271
Klein NK, Hack M, Breslau N 1989 Children who were very low birthweight: developmental and academic achievement at nine years of age. Dev Behav Paediatr 10: 32–37
Dorman C, Katzir B 1994 Cognitive Effects of Early Brain Injury. The Johns Hopkins University Press, Baltimore, pp 164–215
Dehaene S, Spelke E, Pinel P, Stanescu R, Tsivkin S 1999 Sources of mathematical thinking: behavioral and brain-imaging evidence. Science 284: 970–974
Butterworth B 1999 The Mathematical Brain. Macmillan, London, pp 163–215
O'Keefe J, Nadel L 1978 The Hippocampus as a Cognitive Map. Clarendon Press, New York
Moradi AR, Doost HTN, Taghavi MR, Yule W, Dalgleish T 1999 Everyday memory deficits in children and adolescents with PTSD: performance on the Rivermead Behavioural Memory Test. J Child Psychol Psychiatr 40: 357–361
Bremner JD, Randall P, Scott TM, Bronen RA, Seibyl JP, Southwick SM, Delaney RC, McCarthy G, Charney DS, Innis RB 1995 MRI-based measurement of hippocampal volume in patients with combat-related post-traumatic stress disorder. Am J Psychiatry 152: 973–981
Wagner AD, Schacter DL, Rotte M, Koutstaal W, Maril A, Dale AM, Rosen B, Buckner R 1998 Building memories: remembering and forgetting of verbal experiences as predicted by brain activity. Science 281: 1188–1191
Tulving E, Kapur S, Markowitsch HJ, Craik FIM, Habib R, Hule S 1994 Neuroanatomical correlates of retrieval in episodic memory: auditory sentence recognition. Proc Natl Acad Sci USA 91: 2012–2015
Wright IC, McGuire PK, Poline J-B, Travere JM, Murray RM, Frith CD, Frackowiak RSJ, Friston KJ 1995 A voxel-based method for the statistical analysis of gray and white matter density applied to schizophrenia. Neuroimage 2: 244–252
Vargha-Khadem F, Watkins KE, Price CJ, Ashburner J, Alcock KJ, Connelly A, Frackowiak RSJ, Friston KJ, Pembrey ME, Mishkin M, Gadian DG, Passingham RE 1998 Neural basis of an inherited speech and language disorder. Proc Natl Acad Sci USA 95: 12695–12700
Lucas A, Morley R, Cole TJ 1998 Randomised trial of early diet in preterm babies and later intelligence quotient. BMJ 317: 1481–1487
Bryant NL, Buchanan RW, Vladar K, Breier R, Rothman M 1999 Gender differences in temporal lobe structures of patients with schizophrenia: a volumetric MRI study. Am J Psychiatry 156: 603–609
Zaidel DW, Esiri MM, Oxbury JM 1994 Sex-related asymmetries in the morphology of the left and right hippocampi?. J Neurol 241: 620–623
Acknowledgements
The authors thank the children who took part in this study, and their families and schools, for their keen interest in participating.
Author information
Authors and Affiliations
Additional information
Supported by the Medical Research Council and the Wellcome Trust.
Rights and permissions
About this article
Cite this article
Isaacs, E., Lucas, A., Chong, W. et al. Hippocampal Volume and Everyday Memory in Children of Very Low Birth Weight. Pediatr Res 47, 713–720 (2000). https://doi.org/10.1203/00006450-200006000-00006
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-200006000-00006
This article is cited by
-
Novel metrics to characterize temporal lobe of very preterm infants on term-equivalent brain MRI
Pediatric Research (2023)
-
Meta-Analysis of Hippocampal Volume and Episodic Memory in Preterm and Term Born Individuals
Neuropsychology Review (2023)
-
Investigating altered brain development in infants with congenital heart disease using tensor-based morphometry
Scientific Reports (2020)
-
Regional brain volume reduction and cognitive outcomes in preterm children at low risk at 9 years of age
Child's Nervous System (2017)
-
Hippocampal volume reduction is associated with intellectual functions in adolescents with congenital heart disease
Pediatric Research (2016)
