
Abstract
Surfactant nebulization improves lung function at low alveolar doses of surfactant. However, efficiency of nebulization is low, and lung deposition seems to depend on lung aeration. High frequency ventilation (HFV) has been shown to improve lung aeration. We hypothesize that the combination of HFV and surfactant nebulization may benefit lung deposition of surfactant and consequently, lung function. The aim of this study was to compare the effect of surfactant nebulization versus instillation during HFV on lung function, surfactant distribution, and cerebral blood flow. Therefore, severe respiratory failure was induced by lung lavages in 18 rabbits. HFV was applied: frequency = 8 Hz, mean airway pressure = 12 cm H2O, amplitude = 100%, fraction of inspired O2 = 1.0. Technetium-99m-labeled surfactant (Alveofact, 100 mg/kg of BW) was nebulized or instilled (n = 6 each). Six other rabbits did not receive surfactant (control, HFV only). We found that after instillation partial arterial O2 tension increased from 7.0 kPa (95% confidence interval, 6.3-8.0 kPa) to 34 kPa (16-51 kPa), and during nebulization from 7.0 kPa (6.0-9.0 kPa) to 46 kPa (27-58 kPa). Partial arterial CO2 tension decreased after instillation from 6.1 kPa (5.3-7.1 kPa) to 4.8 kPa (3.9-5.6 kPa), and during nebulization, after an initial rise, it decreased from 6.3 kPa (5.3-7.4 kPa) to 4.9 kPa (4.4-5.6 kPa). Both treatments resulted in nonuniform distribution. Surfactant deposition after nebulization was 9.8%. Instillation resulted in a drop of mean arterial blood pressure of 17% (8-31%), and an even more pronounced drop in cerebral blood flow of 39% (18-57%). Nebulization did not affect blood pressure. Cerebral blood flow decreased with a maximum of 27% (10-37%). We conclude that surfactant nebulization during HFV improves lung function in rabbits with severe respiratory failure, without improving distribution, but with less effects on blood pressure and cerebral blood flow, when compared with surfactant instillation.
Similar content being viewed by others
Main
Surfactant therapy for the treatment of neonatal respiratory distress syndrome has led to increased survival and less morbidity in preterm infants (1). However, not all respond with a sustained improvement in lung function (2,3). Presently, research is directed to the fine-tuning of surfactant therapy. Several dosing strategies are tested clinically and different modes of surfactant administration are evaluated experimentally, aiming at an more uniform distribution of surfactant throughout the lungs, which coincides with superior clinical responses (4). Additionally, fluctuations in blood pressure and cerebral perfusion after surfactant instillation have been described (5–7). Recently, concerns about this, in relation to the development of intracranial hemorrhages, have been expressed (8,9). Therefore studies are designed to develop surfactant treatment procedures that result in less hemodynamic and cerebral consequences of surfactant administration (10,11).
Surfactant nebulization during conventional ventilation resulted in a more uniform distribution of surfactant throughout the lungs and improved lung function at a much lower alveolar dose than instilled surfactant, with potentially less hemodynamic consequences (12–16). However, it was shown that nebulized surfactant is mostly deposited in aerated lung parts (17–19). On the other hand it was shown that HFV results in homogenous alveolar lung expansion, with less progressive lung injury (20–24). We hypothesize that surfactant nebulization during HFV would result in uniform distribution of surfactant in a fully aerated lung and hence improved lung function.
Therefore, we performed this study in which surfactant was nebulized or instilled during HFV in rabbits with severe respiratory failure. Primarily, we tested whether surfactant nebulization during HFV can improve arterial oxygen tension and lung dynamics. Furthermore, we tested whether surfactant aerosol is distributed more uniformly over the lungs, and whether blood pressure and cerebral blood flow are less influenced during nebulization than after surfactant instillation.
METHODS
Animals. The experiments were performed in the central animal laboratory of the University of Groningen, under approved institutional care protocols with concerns for animal welfare. Eighteen young adult Chinchilla rabbits (1.8 ± 0.1 kg BW) were anesthetized with sodium pentobarbital, 30 mg/kg of BW (Nembutal, Abbott, the Netherlands), tracheotomized, intubated, and paralyzed with pancuronium bromide, 0.1 mg/kg of BW (Pavulon, Organon, the Netherlands). Additional pentobarbital was given hourly by 15-min infusions.
The rabbits were ventilated with a pressure-limited, time-cycled, neonatal ventilator (Babylog 8000, Drägerwerk AG, Lübeck, Germany). The initial ventilator settings were: intermittent positive pressure ventilation with a frequency of 60/min, inspiratory time equal to expiratory time was 0.5 s, gas flow was 1 L/min·kg of BW, which yielded tidal volumes varying from 7 to 8 mL/kg of BW. Peak inspiratory pressure was limited at 20 cm H2O; Fio2 was set at 1.0.
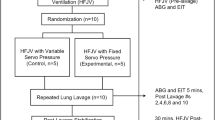
After 15 min of stabilization, the lung lavage procedure was performed, as described earlier (25–27). In short, the lungs were lavaged five times with 35 mL of saline/kg of BW at 38°C. After each lavage the rabbit was allowed to recover for 5 min. Positive end-expiratory pressure was increased stepwise to 8 cm H2O to prevent the surfactant-deficient rabbits from dying of hypoxemia. Fifteen minutes after the last lavage, positive end-expiratory pressure was decreased to 5 cm H2O, resulting in mean airway pressure of 10 cm H2O. After another 15 min, the Babylog ventilator was set in the HFV mode, with the following settings: frequency was 8 Hz, and mean airway pressure was 2 cm higher than mean airway pressure during conventional ventilation, thus 12 cm H2O. Amplitude was 100% and FIO2 was 1.0.
Fifteen minutes after the onset of HFV, surfactant treatment was started (see "Surfactant Treatments"). After 2 h of HFV, a weaning procedure was started as described previously (15,16). The ventilation was set in the conventional synchronized intermittent mandatory ventilation mode, at the settings that were used before HFV. Then, the animals were allowed to breathe spontaneously, by withholding pancuronium bromide. When more than 75% of the minute volume was achieved by spontaneous breathing, the ventilator was set on CPAP. During the last hour, CPAP was decreased from 5 to 2.5 cm H2O. During CPAP, FIO2 was lowered stepwise, every 15 min. The experiment ended when FIO2 was 0.4, PaO2 was <8 kPa, or when the animal died.
Surfactant treatments. We used Alveofact, a bovine-derived surfactant that contains 45 mg of phospholipids/mL (Dr. Karl Thomae GmbH, Biberach an der Riss, Germany). To assess the distribution of surfactant in the lungs, we mixed technetium-99m-labeled Nanocoll (5 MBq in 0.5 mL of saline) with surfactant. Nanocoll (Solco, Biomedical S.p.A. Vercelli, Italy) contains human albumin as a nanocolloid, with 95% of the particles smaller than 80 nm. We have validated this labeling technique earlier, and found a strong correlation in distribution with 14C-dipalmitoylphosphatidylcholine trace-labeled surfactant (correlation coefficient was 0.98) (15,28).
Fifteen minutes after the onset of HFV the rabbits were randomized to three groups of six animals each. In six rabbits, 100 mg of surfactant/kg of BW were nebulized in 60-75 min, using the Miniheart low flow volume medication nebulizer (MiniNEB, Vortran Medical Technology Inc., Sacramento, CA) that we tested earlier during in vitro experiments (28). This nebulizer produces an aerosol with particle sizes that enhance a peripheral deposition of the surfactant in the lungs (mass median aerodynamic diameter of 3 µm, and 70% of the particles were between 1 and 5 µm) (28). The nebulizer was connected to the ventilator circuit just proximal to the endotracheal tube, with a gas flow of 1.5 L/min. The ventilator settings were not changed during nebulization. After finishing nebulization, the nebulizer was removed from the ventilator circuit.
In six other rabbits, surfactant was instilled as a bolus injection, within 10 s, through the side lumen of the endotracheal tube without interrupting ventilation. Before instillation, the empty nebulizer was also connected to the ventilator circuit, with a gas flow of 1.5 L/min, to obtain similar ventilation. The ventilator settings also were not changed. Six other rabbits served as controls and were treated with HFV, without surfactant treatment, to study the effects of HFV only.
Measurements. Arterial PO2 and PCO2 were measured using an ABL 330 blood gas analyzer (Radiometer Co., Copenhagen, Denmark). Intravascular arterial blood pressure was measured continuously with a pressure transducer (Uniflow, Baxter Health Corporation, Santa Ana, CA). The cerebral blood flow was measured using an ultrasonic transit-time flow probe (Transonic Systems Inc., Ithaca, NY) around the left carotid artery.
Immediately after the animals were killed, the lungs were removed and degassed in a vacuum jar. Quasistatic volume pressure characteristics were obtained. The lungs were manually inflated from 0 to 30 cm H2O. Then, the lungs were deflated in six steps, for 30 s each. In each step, the pressure in the lungs was lowered 5 cm H2O. The volume of the lungs at the end of each step was recorded. Quasistatic compliance was calculated by dividing the maximal volume by that pressure (30 cm H2O) and BW. The stability index was calculated by two times the volume at 5 cm H2O added to the volume at 10 cm H2O on deflation, and this was divided by the maximal volume (29). The expansion index was calculated by the volume at 5 cm H2O on deflation, divided by the maximal volume, multiplied by 100% (30).
Processing of the lungs. The lungs were separated in lobes, further separated in central and peripheral parts, frozen by immersion in liquid nitrogen, and cut into 200 pieces. Each piece was weighed, and the radioactivity of 99mTc was counted in a gamma counter (Packard 5000, Packard Instruments Co., Inc., Meriden, CT).
Data analysis. All values are presented as medians and the 95% confidence intervals. Differences in medians between groups were tested for significance by the Kruskall-Wallis nonparametric analysis of variance with Dunn's multiple comparisons post hoc test or the Mann-Whitney test. Multiple comparison analysis of pretreatment and sequential posttreatment values within each group were assessed using Friedman's nonparametric repeated measures test with Dunn's post hoc test.
The distribution of surfactant was assessed by the procedure that we described previously (31). The normalized amount of surfactant in each lung piece was found by dividing the radioactivity per mg of tissue for each lung piece (counts/min per mg) by the average value of radioactivity per mg of tissue of all the lung pieces, for each rabbit. These normalized values were grouped in intervals of 0.1, that is 10% of the mean value (1.0). Lung pieces with normalized values <0.1 or >2.0 were grouped at the extremes of the distribution intervals.
RESULTS
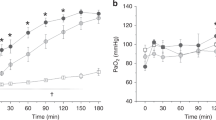
Physiologic measurements. All surfactant-treated rabbits survived the total duration of the study, including the weaning, whereas all rabbits in the HFV only control group died during the weaning. After instillation, PaO2 increased from 7.0 kPa (95% confidence interval, 6.3-8.0 kPa) to 34 kPa (16-51 kPa), and during the weaning PaO2 increased further (Fig. 1). During surfactant nebulization PaO2 rose from 7.0 kPa (6.0-9.0 kPa) to 46 kPa (27-58 kPa), and decreased during the weaning. In the control group, PaO2 did not significantly change during HFV, but decreased during the weaning. PaCO2 decreased after instillation from 6.1 kPa (5.3-7.1 kPa) to 4.8 kPa (3.9-5.6 kPa). During nebulization, after an initial rise, PaCO2 decreased from 6.3 kPa (5.3-7.4 kPa) to 4.9 kPa (4.4-5.6 kPa). PaCO2 did not change significantly during HFV, but increased during weaning.

Sequential measurements of PaO2 divided by FIO2, and PaCO2 in rabbits with severe respiratory failure, treated by HFV, and surfactant instillation or surfactant nebulization. All values are medians and 95% confidence intervals for n = 6 in each group. *p < 0.05 vs pretreatment values.
The isolated lung compliance indices were not significantly different after both modes of surfactant therapy, quasistatic compliance was 1.01 mL/cm H2O·kg of BW (0.90-1.15 mL) after instillation and 0.98 mL (0.79-1.27 mL) after nebulization, and 0.89 mL (0.80-0.94 mL) after HFV only. The stability index was 1.01 mL (0.84-1.12 mL) after instillation, 0.90 mL (0.78-1.08 mL) after nebulization and 0.72 mL (0.55-0.82 mL) after HFV only. The expansion index was 60% (46-72%) after instillation, 54% (46-67%) after nebulization, and 38% (28-50%) after HFV only. Stability and expansion indices were significantly higher in the surfactant-treated groups than in the HFV only control group.
Surfactant distribution. Both modes of surfactant replacement resulted in nonuniform surfactant distribution (Fig. 2). Many lung pieces contained very small amounts of surfactant (<10% of the mean), especially after surfactant nebulization, and many lung pieces contained large amounts of surfactant (>200% of the mean). In contrast, only a few lung pieces contained the average amount of surfactant.

Normalized distribution histograms of surfactant after HFV, and nebulization or instillation in rabbits with severe respiratory failure. All bars represent number of lung pieces within each distribution interval of 10%. All values are means and standard deviations, for n = 6 in each group.
Surfactant nebulization resulted in less uniform lobar surfactant distribution than did surfactant instillation (data not shown). Nebulized surfactant was preferentially deposited in the right upper lobe and right lower lobe, and small amounts of surfactant were found in the right middle lobe and left upper lobe. Additionally, more nebulized surfactant was deposited in the central parts than peripherally in the lungs, as was found after surfactant instillation.
Surfactant nebulization during HFV resulted in a surfactant deposition of 9.8% (6.4-14%) of the initial amount of surfactant in the nebulizer. After instillation, 91% (85-99%) of the instilled dose of surfactant was deposited in the lungs.
Blood pressure and cerebral blood flow. The mean arterial blood pressure changed slightly, but not significantly, during surfactant nebulization (Fig. 3). Whereas, after instillation the mean arterial blood pressure decreased 17% (8-31%) in 4 min and slowly recovered. The cerebral blood flow drop was even more pronounced, 39% (18-57%) in the first 5 min after surfactant instillation, followed by a longer lasting decrease up to 51% (31-69%) after 90 min. During nebulization the cerebral blood flow decrease was less pronounced, with a maximum of 27% (10-37%) in 20 min. During the weaning, cerebral blood flow increased in both groups of surfactant-treated rabbits, 42% (4-66%) from pretreatment values in the nebulization group and 32% (1-57%) in the instillation group. In the control group, during HFV only, mean arterial blood pressure did not change significantly over time. Cerebral blood flow slowly decreased, with a maximum of 28% (10-35%) in 120 min.

Continuous measurement of mean arterial blood pressure and cerebral blood flow in left carotid artery using ultrasonic transit time flow probes, in rabbits with severe respiratory failure treated by HFV and surfactant instillation or surfactant nebulization, or HFV only. All values are expressed as median percentage change from pretreatment values with 95% confidence intervals (gray area) for n = 6 in each group.
DISCUSSION
Surfactant nebulization during HFV can improve lung function in rabbits with severe respiratory failure. However, it does not result in a more uniform distribution of surfactant throughout the lungs than after instillation. Additionally, blood pressure and cerebral blood flow are affected less during surfactant nebulization than after instillation.
We have shown that surfactant nebulization during HFV can improve gas exchange and lung dynamics in surfactant-deficient rabbits. PaO2 values increased during surfactant nebulization and reached almost prelavage levels. However, after finishing nebulization, these levels could not be maintained, and PaO2 values decreased.
The nonsustained effect of surfactant nebulization on oxygenation can be explained by the finding that only small amounts of nebulized surfactant were deposited in the lungs, possibly in combination with a nonuniform distribution pattern of nebulized surfactant. Only 9.8% mg/kg of BW of the initial dose of 100 mg/kg of BW was found in the lungs, in contrast to 91 mg/kg of BW deposition after instillation. Because in the lung-lavaged animal model, lung injury can be progressive, and due to leakage of serum proteins into the alveolar space and activation of mediators of inflammation, surfactant could be inactivated or metabolized. Additionally, the nonsustained effect of nebulized surfactant may be caused by the nonuniform surfactant distribution, which may result in nonuniform aeration of the lung, and overinflation with subsequent lung injury of the alveoli that received the most surfactant. In future studies this can be evaluated by histologic examination.
Almost 10 mg/kg of BW surfactant deposition in the lungs appears to be sufficient considering the calculated amount of 3 mg/kg of BW, that under physiologic conditions forms a monolayer throughout the total alveolar surface (27). However, it is much lower than the minimal instillation dose of 50 mg/kg that has been determined empirically sound for the treatment of respiratory distress syndrome. The effects of nebulized surfactant are undisputed, because we demonstrated clearly that the deflation limbs of the pressure volume curves of the excised lungs of the animals which were treated with nebulized surfactant yielded significantly higher values for stability than the lungs of the control animals that were treated with HFV only.
In contrast to our expectations, we found no improvement in uniformity of surfactant distribution after surfactant nebulization. Therefore we cannot accept our hypothesis that nebulization improves the aeration of the lungs, and thereby improves lung distribution of nebulized surfactant. Actually, in this study surfactant was distributed less uniformly after instillation than was reported by others. Walther et al. (22) and Heldt et al. (32) found no differences in uniformity of surfactant distribution between conventional ventilation and HFV after instillation in premature lambs and rabbit pups. Differences in surfactant preparation, dosage, volume, timing of therapy, and ventilation regimen that were used may explain the conflicting results of the present study. We might have been able to improve the uniformity of distribution, and consequently gas exchange, if we started surfactant therapy after optimizing lung volumes by fine-tuning mean airway pressures to the optimal continuous distending pressure for each individual animal during HFV (23,33,34).
It is interesting that the efficiency of nebulization during HFV (9.8%) was almost equal to the efficiency of nebulization during conventional ventilation (8.4%), that we found earlier under equal conditions, in the same animal model (15). We can only speculate on the mechanisms that determine aerosol deposition throughout the lungs during HFV, because a literature search of this issue was fruitless. Thus, to our knowledge, we are the first to report on aerosol therapy during HFV.
Several reports about variables that influence aerosol deposition during conventional ventilation have been published. Manthous and Hall (35) comprehensively described that these variables can be divided into four categories: nebulizer-related, ventilation-related, lung injury-related, and drug-related characteristics (35). It was shown that low tidal volumes, or minute volumes, in relation to total gas flow through a nebulizer and ventilator, significantly decreases lung deposition of a nebulized drug (36,37). Then, it is surprising that in the present study we found a deposition rate of 10%, because during HFV, tidal volumes are much smaller than they are during conventional ventilation. We speculate that, during HFV, surfactant aerosol is undergoing a driving force that is directed inward to the lung, by the same hypothesized mechanism of augmented diffusion, as oxygen is thought to undergo. Moreover, a large difference in surfactant concentration is found between the filled nebulizer and the lavaged, surfactant-depleted alveoli. In addition we have noted that part of the nebulized surfactant condenses to the walls of the endotracheal tube. In time, small droplets are formed that result in a continuous drip of surfactant into the lungs. This phenomenon is probably responsible for the relatively high deposition of surfactant in the right upper lobe.
Earlier we showed that during conventional ventilation airway pressures can be affected by nebulization (28). Then, we found that jet nebulizers that operate at high gas flows increased airway pressures in a test lung model, whereas the MiniNEB low flow jet nebulizer did not. However, whether surfactant nebulization during HFV influences airway pressures was not studied. In the present study we found during nebulization an initial rise of PaCO2 levels above the levels of the HFV-only group, and a subsequent decrease when nebulization was completed. This might be an indication that nebulization during HFV can also affect airway pressures. Further studies on this issue are warranted with respect to safety of surfactant nebulization.
Finally, we found that surfactant instillation during HFV is followed by a decrease in mean arterial blood pressure, and an even more pronounced drop in cerebral blood flow, whereas during surfactant nebulization these fluctuations were less extensive. Similar fluctuations in blood pressure and cerebral blood flow were found after instillation during conventional ventilation, in the same animal model (16). However, other reports regarding this appear to be conflicting (5–9). Studies in animals and humans have shown that HFV does not affect cerebral blood flow (10,38,39). Our observations in the control group that was treated with HFV only are in agreement with those findings.
Conflicting outcomes of studies on cerebral perfusion may be caused by differences in patient population or animal model, ventilator regimen, and surfactant preparation, dosage, volume, and timing. More fundamentally, cerebral blood flow is determined by many factors (40). Especially strong has been the correlation between PaCO2 and cerebral blood flow (16,41). We think that quick changes in intrathoracic pressures after improvements in lung function and quick changes in blood gasses after surfactant instillation can account for the variability in effects on cerebral perfusion.
In conclusion, surfactant nebulization during HFV can improve lung function in rabbits with severe respiratory failure, also at a low alveolar dose. Additionally, blood pressure and cerebral blood flow are less pronouncedly affected during surfactant nebulization than after instillation. Surfactant aerosol is also transported by means of HFV. However, surfactant nebulization during HFV without lung volume recruitment strategies does not result in a more uniform distribution of surfactant throughout the lungs than after instillation. Therefore we cannot accept our hypothesis that HFV improves lung distribution of nebulized surfactant. Future studies are warranted to evaluate the effects of surfactant nebulization during HFV with adequate lung volume recruitment strategies and safety aspects.
Abbreviations
- HFV:
-
high frequency ventilation
- BW:
-
body weight
- FIO2:
-
fractional inspired oxygen
- CPAP:
-
continuous positive airway pressure
- PaO2:
-
partial arterial O2 tension
- PaCO2:
-
partial arterial CO2 tension
References
Soll RF, Merritt TA, Hallman M 1994 Surfactant in the prevention and treatment of respiratory distress syndrome. In: Boynton BR (ed) New Therapies for Neonatal Respiratory Failure. Cambridge University Press, Cambridge, UK, pp 49–80.
Charnan A, Taeusch W, Fitzgibbon C, Smith GB, Treves ST, Phelps D 1989 Factors associated with surfactant treatment response in infants with severe respiratory distress syndrome. Pediatrics 83: 348–354
Mercier CE, Soll RF 1993 Clinical trials of natural surfactant extracts in respiratory distress syndrome. Clin Perinatol 20: 711–735
Jobe AH, Ikegami M, Jacobs H, Jones S 1984 Surfactant and pulmonary blood flow distributions following the treatment of premature lambs with natural surfactant. J Clin Invest 73: 848–856
Cowan F, Whitelaw A, Wertheim D, Silverman M 1991 Cerebral blood flow velocity after rapid administration of surfactant. Arch Dis Child 66: 1105–1109
Hellström-Westas L, Bell AH, Skov L, Greisen G, Svenningsen NW 1992 Cerebro-electrical depression following surfactant treatment in preterm neonates. Pediatrics 89: 643–647
Skov L, Hellström-Westas L, Jacobson T, Greisen G, Svenningsen NW 1992 Acute changes in cerebral oxygenation and cerebral blood volume in preterm infants during surfactant treatment. Neuropediatrics 23: 126–130
Wells JT, Ment LR 1995 Prevention of intraventricular hemorrhage in preterm infants. Early Hum Dev 42: 209–233
Skinner J 1997 The effects of surfactant on haemodynamics in hyaline membrane disease. Arch Dis Child 76: F67–F69
Kinsella JP, Gerstmann DR, Clark RH, Null DM Jr Morrow WR, Taylor AF, De Lemos RA 1991 High frequency ventilatory oscillation versus intermittent mandatory ventilation: early haemodynamic effects in the premature baboon with hyaline membrane disease. Pediatr Res 29: 160–166
Claris O, Salle BL 1997 High frequency oscillation and exogenous surfactant in the treatment of neonatal respiratory distress syndrome. Acta Paediatr 86: 339–341
Lewis JF, Ikegami M, Jobe AH, Tabor B 1991 Aerosolized surfactant treatment of preterm lambs. J Appl Physiol 70: 869–876
Lewis JF, Ikegami M, Higuchi R, Jobe AH, Absolom D 1991 Nebulized vs instilled exogenous surfactant in an adult lung injury model. J Appl Physiol 71: 1270–1276
Lewis JF, Tabor B, Ikegami M, Jobe AH, Joseph M, Absolom D 1993 Lung function and surfactant distribution in saline lavaged sheep given instilled vs nebulized surfactant. J Appl Physiol 74: 1256–1264
Dijk PH, Heikamp A, Bambang Oetomo S 1997 Surfactant nebulisation: lung function, surfactant distribution and pulmonary blood flow distribution in lung lavaged rabbits. Intensive Care Med 23: 1070–1076
Dijk PH, Heikamp A, Bambang Oetomo S 1997 Surfactant nebulisation prevents the adverse effects of surfactant therapy on blood pressure and cerebral blood flow in rabbits with severe respiratory failure. Intensive Care Med 23: 1077–1081
Lewis JF, Ikegami M, Jobe AH, Absolom D 1993 Physiological responses and distribution of aerosolized surfactant (Survanta) in a non-uniform pattern of lung injury. Am J Respir Crit Care Med 147: 1364–1370
Lewis JF, McCaig L 1993 Aerosolized versus instilled surfactant in a non-uniform pattern of lung injury. Am J Respir Crit Care Med 148: 1187–1193
Henry MD, Rebello CM, Ikegami M, Jobe AH, Langenback EG, Davis JM 1996 Ultrasonic nebulized in comparison with instilled surfactant treatment of preterm lambs. Am J Respir Crit Care Med 154: 366–375
Clark RH 1994 High-frequency ventilation. J Pediatr 124: 661–670
Imai Y, Kawano T, Miyasaka K, Takata M, Imai T, Okuyama K 1994 Inflammatory chemical mediators during conventional ventilation and during high frequency oscillatory ventilation. Am J Respir Crit Care Med 148: 1550–1554
Walther FJ, Kuipers IM, Gidding CEM, Willebrand D, Buchholtz RTF, Bevers EM 1987 A comparison of high-frequency oscillation superimposed onto backup mechanical ventilation and conventional mechanical ventilation on the distribution of exogenous surfactant in preterm lambs. Pediatr Res 22: 725–729
Froese AB, McCulloch PR, Sugiura M, Vaclavik S, Possmayer F, Moller F 1993 Optimizing alveolar expansion prolongs the effectiveness of exogenous surfactant therapy in the adult rabbit. Am Rev Respir Dis 148: 569–577
Nilson R, Berggren P, Curstedt T, Grossmann G, Renheim G, Robertson B 1985 Surfactant treatment and ventilation by high frequency oscillation in premature newborn rabbits: effect on survival, lung aeration, and bronchiolar epithelial lesions. Pediatr Res 19: 143–147
Bambang Oetomo S, Reijngoud DJ, Ennema JJ, Okken A, Wildevuur CRH 1988 Surfactant replacement therapy in surfactant deficient rabbits: early effects, lung function, and biochemical aspects. Lung 166: 65–73
Lachmann B, Robertson B, Vogel J 1980 In vivo lung lavage as an experimental model of the respiratory distress syndrome. Acta Anaesthesiol Scand 24: 231–236
Berggren P, Lachmann B, Curstedt T, Grossmann G, Robertson B 1986 Gas exchange and lung morphology after surfactant replacement in experimental adult respiratory distress syndrome induced by repeated lung lavage. Acta Anaesthesiol Scand 30: 321–328
Dijk PH, Heikamp A, Piers DA, Weller E, Bambang Oetomo S 1997 Surfactant nebulisation: safety, efficiency and influence on surface lowering properties and biochemical composition. Intensive Care Med 23: 456–462
Gruenwald PA 1962 A numerical index of the stability of lung expansion. J Appl Physiol 18: 645–667
Clements JA, Hustead F, Johnson RP, Gibetz J 1961 Pulmonary surface tension and alveolar stability. J Appl Physiol 16: 444–450
van der Bleek J, Plotz FB, Overbeek FM, Heikamp A, Beekhuis H, Wildevuur CRH, Okken A, Bambang Oetomo S 1993 Distribution of exogenous surfactant ins rabbits with severe respiratory failure: the effect of volume. Pediatr Res 34: 154–158
Heldt GP, Merritt A, Golembeski D, Gilliard N, Bloor C, Spragg R 1992 Distribution of surfactant, lung compliance and aeration of preterm rabbit lungs after surfactant therapy and conventional and high-frequency oscillatory ventilation. Pediatr Res 31: 270–275
Bond DM, Froese AB 1993 Volume recruitment manoeuvres are less deleterious than persistent low lung volume in the atelectasis prone rabbit lung during high-frequency oscillation. Crit Care Med 21: 402–412
McCulloch PR, Forkert PG, Froese AB 1988 Lung volume maintenance prevents lung injury during high frequency oscillatory ventilation in surfactant deficient rabbits. Am Rev Respir Dis 137: 1185–1192
Manthous CA, Hall JB 1994 Administration of therapeutic aerosols to mechanically ventilated patients. Chest 106: 560–571
O'Doherty MJ, Thomas SHL, Page CG, Treacher DF, Nunan TO 1992 Delivery of a nebulized aerosol to a lung model during mechanical ventilation. Am Rev Respir Dis 146: 383–388
O'Riordan TG, Greco MJ, Perry RJ, Smaldone GC 1992 Nebulizer function during mechanical ventilation. Am Rev Respir Dis 145: 1117–1122
Mirro R, Tamura M, Kawano T 1985 Systemic cardiac output and distribution during high-frequency oscillation. Crit Care Med 13: 724–732
Laubscher B, van Melle G, Fawer CL, Sekarski N, Calame A 1996 Haemodynamic changes during high-frequency oscillation for respiratory distress syndrome. Arch Dis Child 74: F172–F176
Pryds O, Edwards AD 1996 Cerebral blood flow in newborn infants. Arch Dis Child 74: F63–F69
Edwards AD, McCormick DC, Roth SC, Elwell CE, Peebles DM, Cope M, Wyatt JS, Delpy DT, Reynolds EOR 1992 Cerebral hemodynamic effects of treatment with modified natural surfactant investigated by near infrared spectroscopy. Pediatr Res 32: 532–536
Acknowledgements
The MiniNEB nebulizers (Vortran Medical Technology Inc., Sacramento, CA) were kindly supplied by Medeco B.V. Health Care Products, Oud Beijerland, the Netherlands. The Babylog 8000 ventilator was kindly provided by Drägerwerk AG, Lübeck, Germany.
Author information
Authors and Affiliations
Additional information
Supported by a research grant from Thomae GmbH, Biberach an der Riss, Germany.
Rights and permissions
About this article
Cite this article
Dijk, P., Heikamp, A. & Oetomo, S. Surfactant Nebulization versus Instillation during High Frequency Ventilation in Surfactant-Deficient Rabbits. Pediatr Res 44, 699–704 (1998). https://doi.org/10.1203/00006450-199811000-00012
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199811000-00012
This article is cited by
-
A novel delivery system for supraglottic atomization allows increased lung deposition rates of pulmonary surfactant in newborn piglets
Pediatric Research (2020)
-
From bench to bedside: in vitro and in vivo evaluation of a neonate-focused nebulized surfactant delivery strategy
Respiratory Research (2019)
-
Pharmacokinetics and clinical predictors of surfactant redosing in respiratory distress syndrome
Intensive Care Medicine (2011)
