
Abstract
Pyruvate carboxylase (PC) is a biotinylated mitochondrial enzyme that catalyzes the conversion of pyruvate to oxaloacetate. Children with inborn errors of PC metabolism have lactic acidosis, hypoglycemia, and mental retardation. The variable severity of the clinical phenotype is dependent on both genetic and environmental factors. Two consanguineous families with moderate forms of PC deficiency were characterized at the biochemical and molecular levels. In both families, the probands were found to have low PC activity (range, 2-25% of control) in blood lymphocytes and skin fibroblasts associated with either diminished or normal protein levels. In the first case, sequencing of patient-specific PC cDNA demonstrated a T to C substitution at nucleotide 434, which causes a valine to alanine change at amino acid residue 145. Direct sequencing of the parents showed that they are heterozygous for this mutation. In the second family, a brother and sister had mental retardation and episodes of severe lactic/ketoacidosis in early childhood. In these cases, a C to T substitution at nucleotide 1351 results in a cysteine for arginine substitution at amino acid residue 451; the parents were also found to be heterozygous for this mutation. In both families, no other mutations were found, and both substitutions occurred in relatively conserved amino acid residues. These mutations, located in the biotin carboxylase domain, provide a unique opportunity to analyze how natural occurring mutations affect PC function.
Similar content being viewed by others


Main
PC [pyruvate:carbon dioxide ligase (ADP-forming), EC 6.4.1.1] is a nuclear encoded mitochondrial enzyme that catalyzes the conversion of pyruvate to oxaloacetate. PC is a biotinylated homotetramer that contains three major regions encompassing the biotin-carboxylase, transcarboxylation, and biotin-binding domains(1–3). The cDNA for PC has been characterized for multiple mammalian species including human(4–7), and three-dimensional structures for the biotin-binding and biotin carboxylase domains have been proposed based on the deduced protein sequence of PC(7–9). PC activity is allosterically regulated by acetyl-CoA, and there is hormonal regulation at the level of transcription(10–12).
PC has a major role in intermediary metabolism, as the product of this reaction, oxaloacetate, is an important substrate for both synthetic and anaplerotic metabolic pathways, including gluconeogenesis, lipogenesis, and replenishment of tricarboxylic acid cycle intermediates(13, 14). Inborn errors of PC metabolism are associated with fasting hypoglycemia and lactic acidosis, severe psychomotor retardation, and neuroanatomic changes(13, 15). Based on clinical presentation, PC deficiency has been classified into severe, moderate, or mild (benign) forms depending on the severity of clinical manifestations(13, 16). It has been argued that the clinical severity of PC deficiency is related to specific molecular phenotypes, but this is not always the case(5, 13, 17), and environmental factors may also have a role in determining the impact of PC deficiency on any given subject.
To better understand the relationship between clinical phenotype and the genetic abnormality in PC deficiency, the molecular defects causing PC deficiency in two families in which the probands had moderate PC deficiency have been characterized. The identified mutations are localized to the biotin carboxylase domain. In one case, the mutation alters the amount of immunoreactive PC, whereas in the second case, the mutation affects the catalytic activity of the enzyme.
METHODS
Human subjects. Blood and cultured skin fibroblast samples from members of the two families were investigated at Case Western Reserve University. Biochemical and molecular analyses were done with the approval of the Institutional Review Board of University Hospitals of Cleveland. Control skin fibroblasts were obtained from subjects without identifiable biochemical defects.
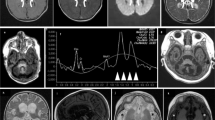
Case 1. The clinical and enzymatic data on this patient and initial molecular investigation have been previously reported(18, 19). Briefly, the proband, the product of a consanguineous union, developed alternating hemiplegia at 14 mo. Laboratory evaluation revealed the presence of fasting lactic acidosis, and magnetic resonance imaging of the brain demonstrated a leukodystrophic process involving the brainstem and subcortical white matter. After a presumptive diagnosis of PC deficiency was made based on enzymatic data, the patient was started on biotin. Treatment with biotin was associated with clinical improvement, but this was not confirmed by higher PC enzymatic activity in lymphocytes(18). A mutation was not located in the biotin-binding region of PC(19).
Case 2A. This male patient, also the product of a consanguineous marriage, was apparently normal at birth and had an uncomplicated neonatal course. However, he did not sit until 8 mo, or walk until age 3 y. Around 2 y of age he had a severe episode of lactic acidosis after a viral illness, associated with an arterial pH of 6.83 and a blood lactate of 12.3 mM (normal, 0.6-2.4 mM). Lactic, 3-hydroxybutyric, and acetoacetic acids were increased in his urine. Before making a specific diagnosis, the patient was treated with supplements of sodium bicarbonate, thiamine, biotin, pyridoxine, and a low protein diet. At age 3½ y, he had another episode of severe lactic acidosis (blood lactate, 14.8 mM) after a febrile illness associated with hypoglycemia (glucose, 0.78 mM), normal plasma ammonia, nonspecific elevation of plasma amino acids, and elevated urinary ketones. Three similar episodes occurred before he was 5 y old, all associated with increased blood lactate. Plasma alanine was noted to be increased on several occasions. When not acutely ill, his blood lactate remained moderately elevated (3-5 mM) with a lactate/pyruvate ratio of 15 (normal 10-20), and low levels of plasma aspartate and glutamate. He did not have hepatomegaly or hepatic dysfunction. After age 10 y, blood lactate was usually normal. The frequency of acute episodes of acidosis diminished and did not recur from age 6 to 17 y. Vitamin supplements and bicarbonate were discontinued after the diagnosis of PC deficiency was established, and the family was instructed not to allow the patient to fast for greater than 12 h. Home monitoring of blood glucose did not reveal episodic hypoglycemia. As an adolescent, his mental development was in the moderately retarded range, necessitating special education. Although slightly temperamental and awkward, the subject has good muscle strength and is able to participate in competitive athletic events. He has had normal growth and pubertal development.
Case 2B. This female patient is the younger sister of Case 2B. She also appeared normal at birth, but remained hospitalized as a neonate for 9 d because of failure to gain weight. At age 20 mo, she had an episode of severe acidosis (pH 6.87), ketosis, hyperammonemia (132 μM), and hypoglycemia (0.72 mM) after a viral illness. Blood lactate was 22 mM, and she was treated with peritoneal dialysis. She received similar treatment as her brother. At age 4 y, she had a severe episode of acidosis (after several earlier milder episodes) during a period of time when her food intake was diminished. At the time of illness, urinary 3-hydroxybutyric and acetoacetate were extremely elevated (50-100 times normal). During this episode, she was treated with large amounts of i.v. glucose and parenteral amino acids (as a source of oxaloacetate). Around this time, she was noted to have frequent seizures characterized by blinking and tripping (petite mal). Other than her seizure disorder, the patient has been in relatively good health, and her blood lactate has remained in the normal range. Her language development is more advanced than that of her older brother, but she also requires special education. She is relatively short (consistent with her family stature) and had menarche at age 13.
Enzyme assays, mitochondrial isolation, and immunoblotting. The activity of PC and other mitochondrial enzymes were measured as previously described(20, 21). For immunoassay, mitochondrial fractions were prepared from cultured fibroblasts by the method described by Millis and Pious(22) with modification suggested by Santorelli et al.(23). The mitochondrial content of the crude homogenates was estimated by assay of citrate synthase. Immunoblot assays were performed as previously described, with the modification that nitrocellulose membranes were blocked with skim milk and bound antibodies were visualized by the amplified streptavidin-akaline phosphatase method(24). Purified PC and total protein isolated from liver were run as standards in adjacent lanes. The membranes were reacted with rabbit anti-PC serum diluted 1:250 in BSA (anti-PC serum was a generous gift from Dr. Brian Robinson, Departments of Biochemistry and Pediatrics, University of Toronto).
RNase protection assay. RNase protection assays were done according to the method of Lee and Costlow(25). Total RNA was isolated from cultured skin fibroblasts by a modified guanidine isothiocyanate/phenol/chloroform extraction, using a commercial kit (TRIzol, Life Technologies) according to the manufacturer's protocol. A 0.4-kb32 P-labeled antisense PC mRNA fragment corresponding to the 3′ end of the human PC cDNA clone(5) was generated using a MAXIscript in vitro transcription kit (Ambion, Austin, TX) and hybridized with the subjects' total RNA following the manufacturer's directions. RNase digestion was performed using RNase A and RNase T1 (RPA II ribonuclease protection kit, Ambion). The protected fragments were separated on a 8 M urea polyacrylamide gel and visualized by autoradiography.
DNA sequencing. Genomic DNA was isolated from patient's cultured skin fibroblasts using a DNA/RNA isolation kit (Amersham-United States Biochemical, Cleveland, OH). Sequences corresponding to the entire PC cDNA were amplified using deoxynucleotide primers complementary to either intronic or exonic sequences of human PC. The location of the primers was designed so that the entire cDNA sequence of PC would be covered by sequencing. The sites of primers used to amplify or sequence mutant cDNA as well as the sequence of intronic primers are included in the figure legends. Amplification was carried out using either Taq polymerase or a mixture of thermostable DNA polymerases (Expand High Fidelity PCR System, Boehringer Mannheim, Indianapolis, IN), and the amplified material was electrophoretically separated on an agarose gel. Discrete bands were purified and subcloned into a PCR IIA plasmid vector (Invitrogen, Carlsbad, CA) and sequenced by the dideoxy method(26). The obtained DNA sequences were analyzed using DNAsis Software (Hitachi, San Bruno, CA).
To confirm mutations and for family analyses, the regions of interest were directly sequenced. For both cases, a sequence encompassing the mutation was amplified using complementary primers (location detailed in figure legends). Amplified DNA was sequenced by the dideoxy method using nested oligonucleotide primers.
RESULTS
Enzymatic analysis. The PC enzymatic data for Case 1 has been previously reported(18). In brief, assay of PC activity showed that the proband had diminished activity in fibroblasts ranging from 7 to 25% of control, whereas PC activity in fibroblasts from his mother and father were in the range of 40 to 60% of controls. PC activity was also low in the patient's lymphocytes with intermediate activity in lymphocytes from the parents and an apparently unaffected sibling.
PC activity was assayed in Cases 2A and 2B in blood lymphocytes and cultured fibroblasts (Table 1). Activity in lymphocytes was 2-6% of the mean of controls and fibroblast activity was 7% for both the brother and affected sister. Activity of two other mitochondrial enzymes, phosphoenolpyruvate carboxykinase and citrate synthase, were normal in lymphocytes and fibroblasts. The range of activity for parents and an unaffected sister compared with the mean for controls was 38-64% for lymphocytes and 33-54% for fibroblasts. This level of PC activity is at the very lower end of the range for controls and strongly suggested that these family members were heterozygous for the defect (see below).
Immunoblot analysis. To determine whether the defect in PC enzymatic activity was related to a catalytic defect or to diminished levels of protein, immunoblot analysis was done in both families using purified mitochondria prepared from cultured fibroblasts. Isolated mitochondria were used instead of total cellular homogenates to enhance the signal to noise ratio, because the concentration of PC in cultured skin fibroblasts is extremely low. In Case 1 (Fig. 1, panel I, lane A), barely perceptible levels of PC immunoreactive protein were found. The low level of intact (full-length) immunoreactive PC in association with low enzymatic activity (7% of control) could be due to the presence of a molecular defect affecting protein synthesis or mitochondrial import of PC. Alternatively, the mutation may cause PC to be more labile, causing it to have greater susceptibility to degradation. The possibility that an inadequate amount of mitochondrial protein was transferred to the membrane is unlikely as the level of lower molecular weight cross-reacting mitochondrial proteins is present in amounts corresponding to the control sample. For Case 2A(Fig. 1, panel II, lane B), mitochondrial PC was equal to control, indicating that synthesis, stability, and the mitochondrial import of PC are apparently intact.

Immunoblot analysis of PC protein. Mitochondrial aliquots prepared from homogenates of cultured skin fibroblasts were separated by SDS-PAGE, transferred to a nylon membrane, and incubated with anti-PC rabbit serum. The mitochondrial aliquot used for each subject was estimated relative to the initial activity of citrate synthase in the crude homogenate(10-14 mU), with an approximate yield of 20-25%. Panel I, lane A, Case 1; lane C, control; lane S, purified bovine PC (0.06 mU). Panel II, lane B, Case 2A; lane C, control;lane S, purified bovine PC (0.06 mU).
RNase protection assay. Severe PC deficiency is sometimes associated with diminished levels of both PC protein and mRNA(17). To determine qualitatively whether a defect in transcription was the reason for the low level of protein in Case 1, an RNase protection assay was performed. This subject had normal levels of PC mRNA (Fig. 2), suggesting that the defect in this case is posttranscriptional. As expected, Case 2A also had normal levels of PC mRNA.

RNAse protection assay. Total RNA (40 μg) RNA was hybridized with a 400-bp radiolabeled antisense PC mRNA probe as described in“Methods.” Lane A is case 1, lane C is a control, and lane B is case 2A.
DNA sequencing. Sequencing of the entire PC cDNA coding region indicated that for Case 1 there was a C for T substitution at nucleotide 434, which was confirmed by direct sequencing (Fig. 3,sequence A). This mutation results in alanine replacing valine at amino acid residue 145. Both the mother and father have the normal and abnormal allele (Fig. 3, sequences F and M), as demonstrated by direct DNA sequencing. No other mutation was found in the PC cDNA or at the splice junctions of the proband.

Detection of a point mutation in Case 1. Patient-specific PC genomic DNA was obtained from Case 1 and parents, and the DNA was directly sequenced. The patient has a thymine to cytosine substitution at nucleotide 434, and the parents are heterozygous for the mutations. Primers used for amplification correspond to nucleotides 181-200 (sense) and 610-629(antisense). For direct sequencing, a sense primer corresponding to nucleotides 358-378 was used(5). Key: Sequence A, case 1; sequence F, father; sequence M, mother;sequence C, control.
Abbreviations: G, guanine; A, adenine; T, thymine; C, cytosine.
For Case 2A, DNA sequencing revealed a C to T substitution at nucleotide 1351 (Fig. 4, sequence B), which results in a change from arginine to cysteine at amino acid residue 451. Family studies using direct DNA sequencing show that the affected sister, Case 2B(Fig. 5, sequence S2), has the same mutation, whereas the clinically unaffected sister and parents are heterozygous for this mutation (Fig. 5, sequence S1, F, and M).

Detection of a point mutation in Case 2. Patient-specific PC genomic DNA from Case 2A was generated by PCR using a sense primer corresponding to a sequence 800 bp forward of the 3′ end of intron 9 (5′- GCTCTCAGCTGAGTGTTCACC-3′) and an antisense primer located 200 bp beyond the 5′ end of intron 10 (5′- GCTGAGGTGAAGCCATGTGCAA-3′) (I. D. Wexler, unpublished observations). A sense primer corresponding to nucleotides 1121-1143 was used for direct sequencing(5). Case 2 (sequence B) has a cytosine to thymine mutation at nucleotide 1351. Sequence C is the control.

Direct DNA sequencing gels of siblings and parents reported in Case 2. The same primers listed in Figure 4 were used. Only the thymine and cytosine lanes are shown. The parents and an asymptomatic sister are heterozygous for the mutation at nucleotide 1351, whereas the affected brother (Case 2A) and sister (Case 2B) are homozygous for the mutation. Key: F, father; M, mother;S1, unaffected sister; S2, affected sister; B, proband; C, control.
DISCUSSION
PC deficiency was first described over 25 y ago(27). Initial characterization of this inborn error of metabolism was difficult due to the instability of this enzyme especially in postmortem tissue(13). With the advent of more precise enzymatic assays and the ability to assay PC in fibroblasts and lymphocytes(21), it became easier to categorize patients with inborn errors of PC deficiency. Robinson et al.(28) studied a large series of patients with PC deficiency and divided them into two categories termed group A (moderate form) and group B (severe form)(13, 17, 28).
The severe form of PC deficiency presents with the constellation of profound lactic acidosis, elevated lactate/pyruvate ratio, hypoglycemia, hyperammonemia, and a life span not extending beyond the first 3 mo of life. In the moderate form, patients present with milder or episodic lactic acidosis and psychomotor retardation. These patients often suffer severe attacks of lactic acidosis when under stress (e.g. infection). Recently, a mild form of PC deficiency has been described that is associated with lactic acidemia and minimal CNS effects(16).
Severity of PC deficiency may be influenced by either the amount of residual activity and/or environmental factors. Robinson et al.(17) have noted that severe PC deficiency is often associated with absent immunoreactive protein and/or PC mRNA. They have suggested that in severe cases of PC deficiency, the residual activity of the enzyme is inadequate to provide sufficient substrate for either the anaplerotic or synthetic reaction pathways involving PC(13). We have shown that other factors must be involved, as there are some patients lacking both PC immunoreactive protein and mRNA who would be classified as having the moderate form based on length of survival and severity of symptoms(5). In addition, we have studied two siblings with extremely low levels of PC activity, one of whom survived only 4 mo, whereas the other lived until the age of 18 mo. Presumably, these brothers had the same mutation, and the difference in longevity was due to unidentified factors (D. S. Kerr, unpublished data). In a case of“benign” PC deficiency reported by Van Coster et al.(16), the patient had only 1.8% of residual activity in cultured fibroblasts, but had near normal neurologic development. Taken together, this would suggest that other factors, including intercurrent illnesses and other stresses such as fasting, may affect outcome. During these episodes, there is an increased requirement for oxaloacetate (for synthesis of glucose) which cannot be met due to the minimal residual levels of PC enzymatic activity. This seems to have occurred in Cases 2A and 2B who had severe exacerbations in early childhood associated with profound ketoacidosis, hypoglycemia, and lactic acidosis.
In this study, we analyzed patients who had moderate PC deficiency based on clinical manifestations and residual PC activity. In Case 1, the symptoms were milder despite the near total lack of PC mitochondrial protein. The milder phenotype may be related either to the fact that this patient appeared to be clinically biotin responsive or to lack of significant stress during infancy that could have precipitated clinical exacerbations.
In both cases, the mutations were located in the biotin carboxylase domain and caused significant amino acid substitutions. In the first case, the mutation may affect protein stability as the PC protein level in mitochondria is diminished; the low level of residual enzymatic activity is proportional to the diminished protein. Conceivably, there could be a problem in mitochondrial import of PC, but the mutation is far from the leader sequence. Another possibility is that the mutation makes PC more susceptible to proteolytic degradation. The clinical response to high doses of biotin remains unexplained, but may be related to enhanced in vivo stability of the mutant protein or increased enzymatic activity of the residual mutant protein.
In the second case, the mutation affects a residue that is conserved in prokaryotic, yeast, and mammalian species(7). Normal PC protein levels as detected by immunoblot analysis would indicate that this mutation affects catalytic activity of PC. Wallace and colleagues have generated a model of the biotin carboxylase domain, and arginine 451 is not located near the active site nor does it involve a critical residue(7). Presumably, the substitution of a cysteine for an arginine residue affects the secondary or tertiary structure of this domain in some way thereby causing diminished enzymatic activity.
Our findings confirm those of Atkin(20) who found that enzymatic activity measurements could be used to identify carriers of the PC mutation. In the two families reported here, the consistently low normal PC activity of the parents and unaffected siblings was confirmed by mutational analysis. It is possible that not all carriers will be detected by enzymatic analysis, as some recessive mutations may be expressed only when the entire homotetramer consists of the mutant protomer. Hence, mutational analysis could enhance the reliability of carrier detection and prenatal diagnosis.
In conclusion, two mutations responsible for the moderate form of PC deficiency have been identified. These mutations occur in the biotin carboxylase domain of PC. Additional studies are necessary to determine how these mutations affect enzymatic activity and clinical manifestations.
Abbreviations
- PC:
-
pyruvate carboxylase
References
Attwood PV, Keech DB 1984 Pyruvate carboxylase. Curr Top Cell Regul 23: 1–55.
Lim F, Morris CP, Occhiodoro F, Wallace JC 1988 Sequence and domain structure of yeast pyruvate carboxylase. J Biol Chem 263: 11493–11497.
Knowles JR 1989 The mechanism of biotin-dependent enzymes. Annu Rev Biochem 58: 195–221.
Zhang J, Xia WL, Brew K, Ahmad F 1993 Adipose pyruvate carboxylase: amino acid sequence and domain structure deduced from cDNA sequencing. Proc Natl Acad Sci USA 90: 1766–1770.
Wexler ID, Du Y, Lisgaris MV, Mandal SK, Freytag SO, Yang BS, Liu TC, Kwon M, Patel MS, Kerr DS 1994 Primary amino acid sequence and structure of human pyruvate carboxylase. Biochim Biophys Acta 1227: 46–52.
MacKay N, Rigat B, Douglas C, Chen HS, Robinson BH 1994 cDNA cloning of human kidney pyruvate carboxylase. Biochem Biophys Res Commun 202: 1009–1014.
Jitrapakdee S, Booker GW, Cassady AI, Wallace JC 1996 Cloning, sequencing and expression of rat liver pyruvate carboxylase. Biochem J 316: 631–637.
Brocklehurst SM, Perham RN 1993 Prediction of the three-dimensional structures of the biotinylated domain from yeast pyruvate carboxylase and of the lipoylated H-protein from the pea leaf glycine cleavage system: a new automated method for the prediction of protein tertiary structure. Protein Sci 2: 626–639.
Toh H, Kondo H, Tanabe T 1993 Molecular evolution of biotin-dependent enzymes. Eur J Biochem 215: 687–696.
Freytag SO, Collier KJ 1984 Molecular cloning of a cDNA for human pyruvate carboxylase. Structural relationship to other biotin-containing carboxylases and regulation of mRNA content in differentiating preadipocytes. J Biol Chem 259: 12831–12837.
Zhang J, Xia WL, Ahmad F 1995 Regulation of pyruvate carboxylase in 3T3-L1 cells. Biochem J 306: 205–210.
Jitrapakdee S, Booker GW, Cassady AI, Wallace JC 1997 The rat pyruvate carboxylase gene structure. J Biol Chem 272: 20522–20530.
Robinson BH. 1995 Lactic acidemia (Disorders of pyruvate carboxylase, pyruvate dehydrogenase). In: Scriver CR, Beaudet AL, Sly WS, Valle D (eds) Metabolic and Molecular Basis of Inherited Disease, 7th Ed. McGraw-Hill, New York, pp 1479–1499.
Attwood PV 1995 The structure and the mechanism of action of pyruvate carboxylase. Int J Biochem Cell Biol 27: 231–249.
Robinson BH, MacKay N, Chun K, Ling M 1996 Disorders of pyruvate carboxylase and the pyruvate dehydrogenase complex. J Inherit Metab Dis 19: 452–462.
Van Coster RN, Fernhoff PM, De Vivo DC 1991 Pyruvate carboxylase deficiency: a benign variant with normal development. Pediatr Res 30: 1–4.
Robinson BH, Oei J, Saudubray JM, Marsac C, Bartlett K, Quan F, Gravel R 1987 The French and North American phenotypes of pyruvate carboxylase deficiency, correlation with biotin containing protein by3 H-biotin incorporation, 35S-streptavidin labeling, and Northern blotting with a cloned cDNA probe. Am J Hum Genet 40: 50–59.
Higgins JJ, Glasgow AM, Lusk M, Kerr DS 1994 MRI, clinical, and biochemical features of partial pyruvate carboxylase deficiency. J Child Neurol 9: 436–439.
Higgins JJ, Ide SE, Oghalai JS, Polymeropoulos MH 1997 Lack of mutations in the biotin-binding region of the pyruvate carboxylase(PC) gene in a family with partial PC deficiency. Clin Biochem 30: 79–81.
Atkin BM 1979 Carrier detection of pyruvate carboxylase deficiency in fibroblasts and lymphocytes. Pediatr Res 13: 1101–1104.
Atkin BM, Utter MF, Weinberg MB 1979 Pyruvate carboxylase and phosphoenol-pyruvate carboxykinase activity in leukocytes and fibroblasts from a patient with pyruvate carboxylase deficiency. Pediatr Res 13: 38–43.
Millis AJT, Pious DA 1973 Oxidative phosphorylation in mitochondria isolated from human fibroblasts. Biochim Biophys Acta 292: 73–77.
Santorelli FM, Mak SC, Vazquez-Memije ME, Shanske S, Kranz-Eble P, Jain KD, Bluestone DL, DeVivo DC, DiMauro S 1996 Clinical heterogeneity associated with the mitochondrial DNA T8993C point mutation. Pediatr Res 39: 914–917.
Hemalatha SG, Kerr DS, Wexler ID, Lusk MM, Kaung M, Du Y, Kolli M, Schelper RL, Patel MS 1995 Pyruvate dehydrogenase complex deficiency due to a point mutation (P188L) within the thiamine pyrophosphate binding loop of the E1 alpha subunit. Hum Mol Genet 4: 315–318.
Lee JJ, Costlow NA 1997 A molecular titration assay to measure transcript prevalence levels. Methods Enzymol 152: 633–648.
Sanger F, Nicklen S, Coulson AR 1977 DNA sequencing with chain-terminating inhibitors. Proc Natl Acad Sci USA 74: 5463–5467.
Hommes FA, Polman HA, Reerink JD 1968 Leigh's encephalomyelopathy: and inborn error of gluconeogenesis. Arch Dis Child 43: 423–426.
Robinson BH, Oei J, Sherwood WG, Applegarth D, Wong L, Haworth J, Goodyer P, Casey R, Zaleski LA 1984 The molecular basis for the two different clinical presentations of classical pyruvate carboxylase deficiency. Am J Hum Genet 36: 283–294.
Author information
Authors and Affiliations
Additional information
Supported by National Institutes of Health Grants HD-32434 (I.D.W.), DK20478 (D.S.K.), the Diabetes Association of Greater Cleveland (I.D.W. and D.S.K.), the Indiana State Department of Health (R.S.W.), and the National Institute of Neurologic Disorders and Stroke. (J.J.H.).
Rights and permissions
About this article
Cite this article
Wexler, I., Kerr, D., Du, Y. et al. Molecular Characterization of Pyruvate Carboxylase Deficiency in Two Consanguineous Families. Pediatr Res 43, 579–584 (1998). https://doi.org/10.1203/00006450-199805000-00004
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199805000-00004
This article is cited by
-
Structure and function of biotin-dependent carboxylases
Cellular and Molecular Life Sciences (2013)
-
Crystal structures of human and Staphylococcus aureus pyruvate carboxylase and molecular insights into the carboxyltransfer reaction
Nature Structural & Molecular Biology (2008)
-
CREB regulates hepatic gluconeogenesis through the coactivator PGC-1
Nature (2001)
