
Abstract
Long-acting gonadotropin-releasing hormone (GnRH) analogs (GnRH-a) suppress gonadal steroid production and are used in precocious puberty, resulting in an arrest of pubertal development, a slower epiphyseal maturation, and a deceleration of growth, but an increased final height. However, the way that GnRH-a affect growth is not clear. GnRH-a treatment might not only affect gonadal steroid production but might also modulate the GH axis and thereby affect growth. We used a rat model to investigate the long-term effects of prepubertally started GnRH-a treatment (triptorelin) on growth, spontaneous GH secretion, hepatic GH receptors (GHR), and GH-binding protein (GHBP) and compared it with surgical gonadectomy. Triptorelin affected most parameters in the same direction as surgical gonadectomy but to a lesser extent. In females, growth was enhanced by triptorelin, baseline GH secretion was decreased, and hepatic GHR and GHBP were decreased. Apart from these effects on the GH axis, reduction of the direct inhibiting effect of estrogen on growth could be responsible for the triptorelin-induced growth. In males, triptorelin treatment enhanced body weight gain and slightly enhanced gain in length. GH peak amplitude was the only parameter of GH secretion affected and decreased, whereas GHR or GHBP were not affected. This stimulation of weight gain by long-term triptorelin treatment in male rats, which is opposite the effect of surgical gonadectomy, could indicate an interference of GnRH-a in the hormonal regulation of food intake and body weight control. We conclude that triptorelin treatment affected growth and the GH-GHR-GHBP axis in rats, more markedly in females than in males. However, triptorelin was not as effective as surgical gonadectomy.
Similar content being viewed by others

Main
Long-acting GnRH-a can reversibly suppress gonadal steroid production, when given continuously(1). After an initial stimulation of gonadotropin release, the pituitary response diminishes, and the resulting decrease in LH and FSH levels leads to a reduction in gonadal steroid synthesis(2, 3). The mechanism of reversible chemical castration by GnRH agonists is not fully understood, but both the number of GnRH receptors(4) and postreceptor signaling events(5) may be involved. Clinically, GnRH-a have proved useful in the treatment of prostate cancer, endometriosis, and central precocious puberty(6), especially with the advent of depot preparations of superagonists(7).
In precocious puberty, GnRH-a suppress the acceleration in epiphyseal maturation, which otherwise would result in short adult stature(8, 9), and there is now increasing interest(10, 11) in the potential value of using GnRH-a in other children with an impaired predicted adult height, in the hope that delaying puberty might extend the time available for growth by delaying epiphyseal closure. However, the advantages of this approach are by no means clear(11–13), because gonadal steroids also affect growth and the growth plate directly, as well as modulating pituitary GH secretion, hepatic GHR, and the related GHBP. There are only a few reports evaluating GH secretion and GHBP in GnRH-a-treated children with precocious puberty, but results are contradictory, and studies often lack untreated control groups(14–18).
The purpose of this study was to use prolonged GnRH-a treatment in an experimental animal model in which the effects on growth, GH secretion, GHR, and GHBP can all be directly assessed. In addition, the effectiveness of depot GnRH-a treatment could be compared with a state of complete gonadal steroid deficiency induced by gonadectomy.
The advantages of using the rat for such experiments is that it shows sexual dimorphism in growth and GH secretion(19–21), in its expression of hepatic GH-receptors(22) and that GHBP(23) can be measured, and it is modulated by exogenous gonadal steroids(24, 25). We have now investigated the effects of the widely used slow release GnRH-a preparation triptorelin in prepubertal male and female rats, measuring growth, gonadal weight, hepatic GHR, and GHBP levels. We have also compared the effects of GnRH-a treatment with surgical gonadectomy on the 24-h pattern of GH secretion in both male and female animals.
METHODS
Animals. Normal rats of the NIMR:AS strain were obtained from our SPF colony at the National Institute for Medical Research at Mill Hill, London, UK. Rats were housed in light- and temperature-controlled rooms(23-25°C, 14-h light) with food and water available ad libitum. Experiments were approved by the local ethical committee for animal experiments.
Experiment 1. To assess the effects of a GnRH-a, prepubertal, 4-wk-old male and female rats (n = 6-8) were injected with a slow release preparation of triptorelin (Decapeptyl-CR, Ferring AB, Malmö, Sweden) at a dose of 1 mg/kg s.c. every 3 wk. A control group received excipient alone. Weekly measurements of body weight and body length (= nose-anus length)(26, 27) were taken, and after 15 wk of treatment, rats were killed, and blood and liver samples were taken for measurement of gonadal steroids, GHBP, and hepatic GHR binding. In addition, tibial length was measured, using callipers.
Experiment 2. At 4 wk of age, groups (n = 6-22) of rats were gonadectomized or sham-operated under halothane anesthesia. Sham-operated rats immediately received either 1 mg/kg triptorelin or excipient s.c., and this treatment was repeated every 3 wk as above. At the age of 10-11 wk, rats were transferred to individual metabolic cages. Under halothane anesthesia, a catheter was inserted in the jugular vein and attached via a swivel to an automatic blood microsampling system, previously described(20). Cannulas were flushed twice daily with heparinized(20 units/mL) saline. After 2 d of recovery, serial blood samples (20 μL every 10 min) were collected for 24 h. GH was measured directly by RIA (using NIDDK reagents) in diluted whole blood(21) and expressed as nanograms/mL in terms of the rat GH-RP-2 standard. The minimal detectable concentration was 0.4 ng/mL, and the combined sampling and interassay variability was estimated at 10%.
Experiment 3. In two other experiments, groups of rats(n = 5-7) were sham-operated, gonadectomized, or treated with triptorelin at the age of 4 wk as before. In the first experiment, they were weighed and measured weekly until the age of 7 wk, when they were killed, and plasma and liver samples were taken for GHBP and GH-radioreceptor assays. In the second experiment, they were weighed and measured weekly until the age of 10.3 wk.
Analysis of GH profiles. Pulsar analysis (PC Pulsar Program version 2.0)(28) was used to analyze the 24-h GH profiles, with the following parameter settings: peak weight 0.05, splitting parameter 2.7, smoothing time 0.5, threshold value 0.01, assay parameters A, B, C, 0, 10, and 0, respectively, and peak detection parameters G 1-5 set to 5, 3, 2, 1.5, and 1, respectively.
GHR and GHBP assays. GHR binding was assayed as previously described using radioiodinated recombinant bovine GH(27), essentially following the method of Maiter et al.(29). Results are presented as percent specific GH binding per mg of protein(30). Plasma GHBP level was measured by RIA(31). Samples were assayed in duplicate. The detection limit was 1.2 μg/L, and the interassay coefficient of variation was 10%.
Estrogen and testosterone assays. Gonadal steroids were measured by RIA, using commercial kits (RIA-mat Byk Sangtec, Dietzenbach, Germany for testosterone; RSL direct, ICN Biomedicals, Zoetermeer, The Netherlands for 17β-estradiol). The detection limit of the testosterone RIA was 0.1 ng/mL. 17β-Estradiol was measured after extraction of the plasma on C18 columns (3 mL/200 mg) (Varian), concentrating the samples 4-fold by freeze drying. The detection limit of the RIA was 1 pg/mL.
Statistics analysis. Results are presented as mean ± SEM. Data of all groups in an experiment were subjected to ANOVA followed by Student Neuman Keuls test or Fisher's protected LSD test. Growth curves were analyzed using a multivariate ANOVA for repeated measures, followed by t tests.
RESULTS
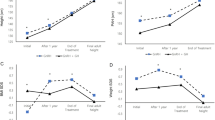
Experiment 1. Figure 1,a and b, shows the effects of chronic triptorelin treatment on body weight and body length of male and female rats. At 4 wk of age, growth rates begin to diverge in male and female rats. In females, triptorelin treatment accelerated both gain in weight and longitudinal growth. The effect became significant at 7 wk of age and was maximal by 11 wk of age, after which the growth rates were similar. Acceleration of growth in triptorelin-treated females was expected, because ovariectomy also results in increased growth rate. In contrast, the expected deceleration of growth in males, which is seen after surgical gonadectomy, was not observed after triptorelin treatment. Triptorelin in males even increased weight gain after 9 wk of treatment and gain in length after 11 wk of treatment. Tibial length (at sacrifice) was increased by triptorelin in females (3.52 ± 0.02 versus 3.62 ± 0.02 cm (saline versus triptorelin, respectively), p < 0.01), but not in males (3.98 ± 0.01 versus 3.97 ± 0.02 cm (saline versus triptorelin, respectively), p > 0.05).

Growth curves for (a) weight and(b) body length for saline and triptorelin (1 mg/kg s.c., once every 3 wk)-treated male and female rats. *p < 0.05, **p < 0.01 vs saline-treated rats of the same sex (indicating significantly different curves).
As expected, both testis and ovarian weights were significantly reduced after 15 wk of triptorelin treatment (Fig. 2a), but the effect was more marked in females than in males. None of the triptorelin-treated females showed vaginal opening, whereas all saline-treated females did, confirming that triptorelin effectively delayed puberty.

The effect of 15-wk triptorelin treatment on(a) gonadal weight, (b) hepatic GHRs, and (c) GHBP. Rats were treated with triptorelin (1 mg/kg s.c. once every 3 wk) from the age of 4 wk. *p < 0.05, **p < 0.01 vs saline-treated rats of the same sex. ††p < 0.01vs saline-treated males.
As expected, plasma GHBP levels were higher in females than in males (Fig. 2c). Triptorelin treatment in females reduced GHBP levels completely to male values, whereas this treatment had no effect on GHBP in males (Fig. 2c). Hepatic bovine GH binding was also higher in females than in males (Fig. 2b), but there were no statistically significant effects of triptorelin in either group.
Testosterone levels were significantly lower in triptorelin-treated male rats compared with saline-treated ones (0.73 ± 0.03 nmol/L (range 0.6-0.8) versus 4.2 ± 1.3 nmol/L (range 1.2-7.2) p< 0.01). Estrogen levels, sampled at various stages of the estrus cycle, ranged from 2.6 to 41.97 pg/mL (mean 15.24 ± 6.1) in saline-treated females, compared with 1.55-2.41 pg/mL (mean 1.83 ± 0.29) in triptorelin-treated females, but, due to the large variation, this did not reach statistical significance.
Experiment 2. Figure 3 shows representative 24-h profiles of GH secretion obtained from groups of sham-operated, gonadectomized, or triptorelin-treated male and female rats. The sham-operated male rats (Fig. 3a) showed 3-h episodic secretory bursts of GH secretion separated by periods of low baseline GH output, typical of normal male rats. At the other extreme, sham-operated female rats (Fig. 3f) exhibited a much more continuous irregular pattern with frequent, smaller GH peaks over a higher GH baseline, and an increase in pulse height after the onset of darkness, typical of normal female rats. Pulsar analysis (Fig. 4) confirmed that males had significantly higher GH peak heights and widths, but secreted fewer pulses with a longer interpulse interval and a lower baseline than do females. Despite these differences in pattern, the mean GH levels (and thus area under the curve) were not different between sham-operated males and females.

Representative spontaneous 24-h GH secretion in a(a) sham-operated saline-treated (intact) male, (b) triptorelin-treated male, (c) gonadectomized male, (d) ovariectomized female, (e) triptorelin-treated female, and(f) sham-operated saline-treated female. Note the gliding scale from typical male (a) to typical female (f) GH secretion pattern, especially for GH baseline and peak amplitude and interval. Gonadectomy, sham-operation, or start of triptorelin treatment (1 mg/kg s.c. once every 3 wk) was at 4 wk of age and blood microsampling at 10-11 wk of age.

Pulsar analysis of 24-h GH secretion profiles of control, triptorelin-treated, or gonadectomized male and female rats. Gonadectomy, sham-operation, or start of triptorelin treatment (1 mg/kg s.c. once every 3 wk) was at 4 wk of age and 10-min blood microsampling at 10-11 wk of age. *p < 0.05, **p < 0.01 vs saline-treated rats of the same sex. †††p < 0.001, ††p < 0.01 vs saline-treated males.
Figure 3b-e show the transition between these GH patterns affected by chemical or surgical gonadectomy. Triptorelin treatment in males (Fig. 3b) had no effect on the episodic pattern of GH, but the amplitude of the GH peaks was significantly reduced(p < 0.05, Fig. 4d). Gonadectomy in males had a little more pronounced effect (Fig. 3c). The regular GH pattern was somewhat disturbed, shown by a marginal increase in number of peaks (p = 0.058, Fig. 4c) and decrease in peak length (p < 0.05, Fig. 4f) and peak interval (p < 0.05, Fig. 4e). Changes in baseline (p = 0.09, Fig. 4b) and peak amplitude (p = 0.10, Fig. 4d) did not reach statistical significance. Ovariectomy in female rats (Fig. 3d) resulted in a profound decrease of baseline GH level (p < 0.01, Fig. 4b), and therefore decreased mean GH levels (p < 0.05, Fig. 4a), but none of the other parameters changed significantly. Triptorelin treatment in female rats (Fig. 3e) also decreased baseline levels (p < 0.01), but to a lesser extent than ovariectomy. Triptorelin-treated females also had a higher number of GH peaks(p < 0.01, Fig. 4c) than did sham-operated or ovariectomized females.
Experiment 3. Because triptorelin treatment was less effective than gonadectomy in altering GH secretion, we compared the short-term effects of surgical and chemical gonadectomy on other parameters. Male and female rats were gonadectomized or injected with triptorelin at the age of 4 wk and killed 3 wk later. Gonadectomy decreased gain in weight (less so in length) in male rats and increased gain in weight and length in female rats (Fig. 5,a and b). Triptorelin treatment was less effective than surgical gonadectomy in both males and females, and increased weight gain only in female rats significantly (p < 0.01). The longer experiment (until the age of 10.3 wk) gave similar results: in males, gonadectomy decreased weight and length gain (p < 0.05), but triptorelin had no effect (Table 1A). In females, ovariectomy and triptorelin treatment increased weight and length gain compared with sham-operated rats (p < 0.01). Weight and length of tritptorelin-treated females was halfway between that of sham-operated and ovariectomized rats until the age of 7 wk, after which they caught up to the level of ovariectomized rats (Table 1B). When looking more in detail to the weight data in the male rats, a similar trend was seen: weight was in between that of sham-operated and gonadectomized rats until the age of 7 wk, after which triptorelin-treated rats accelerated their growth.

Effect of short-term gonadectomy or triptorelin treatment on (a) weight gain, (b) body length gain,(c) hepatic GHRs, and (d) plasma GHBP. Treatment started at 4 wk of age, and sacrifice was at 7 wk of age. *p < 0.05,**p < 0.01 vs saline-treated rats of the same sex.†††p < 0.001, ††p< 0.01 vs saline-treated males.
Females had higher GHBP levels than males. Neither surgical nor chemical gonadectomy changed levels significantly, though GHBP levels in triptorelin-treated female rats lay between those of sham-operated and ovariectomized rats. Hepatic bovine GH binding was not significantly different between groups but showed the same tendency (Fig. 5,c and d). Again, bovine GH binding in triptorelin-treated rats was close to binding in gonadectomized animals though less so in males than in females.
DISCUSSION
Continuous GnRH exposure leads to a desensitization of the pituitary and thus to a diminished gonadotropin release and reduced gonadal steroid production(1). Long-acting GnRH-a are therefore used to delay puberty and prevent premature closure of growth plates(8, 9). However, such treatment also modulates height velocity, which could be due to an effect of GnRH-a treatment on GH secretion, hepatic GHRs or GHBP. This is difficult to assess in children in a controlled manner. It has been reported that GnRH-a do not change GH secretion(16) or decrease peak amplitude(15) and that GHBP is not changed(15) or increased(18) during GnRH-a treatment in children with precocious puberty. We therefore decided to investigate the effects of GnRH-a treatment on this GH-GHR/GHBP growth axis in a rat model, because the regulation of GH secretion, number of GHRs, and GHBP levels by gonadal steroids can be directly assessed in the rat(24, 25, 32, 33).
Rats of the AS strain are in puberty between the age of approximately 28 and 42 d. Females have their vaginal opening around 35-40 d of age, which characterizes the end of puberty. Male rats start to grow faster than females from the age of 4-5 wk, and at that age GH secretion also becomes sexually dimorphic. Neonatal gonadectomy in rats reduces growth in males and increases growth in females from the age of 30-35 d. The effect of prepubertal gonadectomy (25 or 30 d of age) in males is much less pronounced but still present, and prepubertal ovariectomy in females clearly stimulates growth(24).
This is the first report to evaluate the growth of rats treated with triptorelin from prepubertal age until adulthood. Like prepubertally ovariectomized rats(24), triptorelin-treated female rats showed enhanced growth, both in terms of weight and longitudinal growth. This enhancement of growth started at the age of 6 wk, approximately 2 wk after initiation of treatment, and continued for about 5 wk, after which the growth curve was parallel to that of saline-treated rats. A time lag was expected given the initial stimulatory phase of such GnRH-a before desensitization of the pituitary occurs(1). However, it also probably reflects a time course of steroid disappearance because surgical ovariectomy also does not affect growth immediately. Triptorelin treatment had less effect on the growth rate in male rats than in females. This agrees with earlier findings that prepubertal orchidectomy has little effect on growth(24), and suggests that growth during and after puberty is more sensitive to estrogen than to testosterone in rats.
We then wished to know whether changes in GH secretion could be responsible for the differential effects of triptorelin on growth in the two sexes. As is well known(19, 34), females have a higher baseline GH and more frequent shorter pulses of lower amplitude than do males. Pulsar analysis showed that triptorelin treatment in males affected only peak amplitude. We previously demonstrated that increases in GH peak amplitude accelerated growth in GH-deficient rats(31). Despite the decreased GH peak amplitudes, triptorelin did not inhibit growth. In females, baseline GH levels were most clearly affected by triptorelin. We recently showed that varying GH baseline independently of GH peak had little effect in growth in gonadally intact GH-deficient rats(31). Given these relatively small effects on GH secretion, it is more likely that the effects of triptorelin on growth are due to a reduction of the direct inhibiting effect of estrogen on growth(35) or to the deceleration of epiphyseal maturation in the absence of estrogen. Support for the latter option is given by the fact that a mutation in the human estrogen receptor caused a failure in growth plate closure and continuing growth in a man(36).
Although longitudinal growth, measured by body length and tibia length, was only slightly affected by long-term triptorelin treatment in male rats, their body weight was increased, the opposite to what occurs after gonadectomy in males. This might point to an increased fat mass. Although its relevance is doubtful, we calculated rat BMI as BMI = weight/nose-anus length2. BMI was increased after triptorelin treatment in both males and females (results not shown). Such increase in BMI has also been observed during triptorelin treatment in children(9, 37). Apart from fat mass, BMI is dependent on bone and muscle mass. Because it is unexpected that triptorelin treatment will increase muscle or bone mass, fat mass probably increases during triptorelin treatment. From our experiments we cannot explain this effect but leptin, the hormone involved in body weight regulation and reducing food intake in leptin-deficient mice, also stimulates the reproductive system and increases LH and FSH levels in those mice(38). Thus, a link between regulation of the GnRH-LH/FSH axis and leptin might exist.
When looking at the growth curves of Figure 1, there seems to be a time difference in the effect of triptorelin on growth in the two sexes with a relatively early effect in females compared with males. However, the effect of triptorelin on growth is the sum of positive and negative effects of triptorelin on growth: if triptorelin indeed has a fat mass and weight-increasing effect, as described above, then this would counteract the effect of reduced testosterone levels (weight-decreasing effect) in males but be additive to the effect of decreased estrogen levels(weight increasing effect) in females. This could be an explanation for the apparent time difference in the effect of triptorelin in males versus females. Experiment 3 shows that, until about 3-4 wk after the start of triptorelin treatment, the effect of triptorelin is in the direction of that of gonadectomy in both sexes, but that afterwards an acceleration in weight gain in both genders appears, suggesting a second way of action of triptorelin, besides suppression of gonadal steroid production.
Gonadectomy affected different components of GH secretion in males and females(24). Ovariectomy decreased baseline GH without altering peaks, whereas orchidectomy affected peak parameters without changing baseline GH significantly. One interpretation of these data could be that ovariectomy affects mainly somatostatin tone, whereas the most prominent effects of orchidectomy in males is on GRF. This agrees with experiments in which GH profiles were studied in sham-operated and gonadectomized male rats with and without estrogen treatment(39) and gains support from in vitro experiments showing that orchidectomy reduces the responsiveness of somatotrophs to GRF(40). Furthermore, manipulation of testosterone levels affects the number of GRF neurons and GRF mRNA levels per neuron(41), whereas both estrogen and testosterone affect somatostatin mRNA(42).
Triptorelin treatment had a much smaller impact on GH secretion than did surgical gonadectomy. In males, the only factor affected was peak amplitude, and in females baseline GH levels fell, but not to the same extent as in ovariectomized rats. Inspection of the profiles shows that the GH patterns of triptorelin-treated animals lie somewhere between the extremes of the patterns of intact and gonadectomized animals. One exception is that the number of GH peaks was much higher in the triptorelin-treated females than in any of the other groups. GnRH-a treatment may affect GH pulsatility via mechanisms other than suppression of gonadal steroid production. The neuroendocrine status is different in gonadectomized animals, which have high gonadotropin and GnRH levels(43) compared with triptorelin-treated animals which have blocked GnRH signaling and suppressed gonadotropins(1–3). This different neuroendocrine status could result in a different effect on the hypothalamus-pituitary-GH axis in gonadectomized compared with triptorelin-treated rats and may account for the differences we found between the GH profiles in these groups.
We also measured hepatic GHR binding and plasma levels of GHBP, which is an alternatively spliced product of the GHR in the rat(44). Triptorelin had no effect on GHR binding, but did after long-term treatment reduce the higher plasma GHBP levels seen in normal female rats(23) to those in males, confirming earlier results for ovariectomy(25). Because GHBP levels are selectively sensitive to baseline GH exposure independent of GH peaks in the rat(31), this effect of triptorelin is probably mediated via the reduction in baseline GH exposure. We have previously commented on the inverse relationship between growth rate and GHBP that can be observed with different estrogen states in the rat(25), but the significance for growth of such changes in GHBP is unclear because GHBP can both enhance and inhibit GH action(45, 46) and the mechanism of generation of GHBP and its sensitivity to gonadal steroids is very different in humans(33, 47, 48). Triptorelin treatment in male rats did not affect GHBP levels, in line with results for orchidectomy and experiments showing that GHBP levels are not affected by testosterone(49).
Because the effects of triptorelin on growth and bone maturation in children can also be quite variable, one can question whether triptorelin suppresses gonadal steroids completely(50, 51), and whether the effectiveness of triptorelin treatment on growth parameters equals that of complete removal of gonadal steroid production.
One possible explanation for the less marked or different effects of triptorelin than of gonadectomy is that the dose was inadequate to achieve complete gonadal suppression. Surprisingly, there is little literature about the doses of long-acting triptorelin necessary for suppression of gonadal steroid production in rats. One article states that a dose of 300 μg/kg i.m. provokes pituitary desensitization in rats(4). We chose a dose of 1 mg/kg s.c. every 21 d, which is thus probably supramaximal, also compared with the usual human dose of 3.6 mg per injection, independent of body weight, every month. This dose was clearly effective, because both testis and ovarian weights were reduced by 3 wk of treatment (data not shown) and remained low over 15 wk of treatment, and plasma steroid measurements confirmed the suppression of the pituitary gonadal axis. However, ovarian weight was more reduced than testes weight (70% versus 20% decrease). Testis weight, determined by germ cell epithelium and Sertoli cells, depends mainly on the number of Sertoli cells produced during perinatal development(52) so that our later GnRH-a treatment might not be very efficient to reduce testis weight. Furthermore, testis weight and Sertoli cell number is regulated by FSH(53), which may not be completely suppressed by GnRH-a treatment(54).
Another possible explanation for the difference between surgical and chemical gonadectomy is the presence of other factors in the gonads affecting the hypothalamus-pituitary-growth axis, which are not regulated by LH/FSH and are thus not suppressed by GnRH-a. For example it is not clear how GnRH-a will affect the inhibin/activin system, which might have significant impact on GH production(55). Conversely, there may be factors other than LH that stimulate gonadal steroid production and are less affected by GnRH-a. One factor produced in the testis that stimulates steroidogenesis by Leydig cells has recently been isolated from Sertoli cells and is composed of TIMP-1 and the proenzyme form of cathepsin L(56). TIMP-1 is also produced in luteal and granulosa cells of the ovary and stimulates steroidogenesis in the ovary. Because FSH regulates TIMP-1, and may not be completely suppressed by GnRH-a(54, 57), TIMP-1 might continue to stimulate low level gonadal steroid production in the triptorelin-treated rats.
A third possibility is that extrapituitary GnRH receptors are affected differently by triptorelin treatment than pituitary GnRH receptors. There are GnRH receptors in the gonads and the hypothalamus, but also in extrahypothalamic regions, including the hippocampus and the limbic system, via which GnRH might modulate behavior(58, 59). In addition, GnRH acts as a neuromodulator/neurotransmitter in some brain areas, and GnRH is, apart from the nerve fibers in the median eminence, also released from nerve fibers near the third and lateral ventricle, maybe into the cerebrospinal fluid enabling to act at distant sites(60). It is unknown how continuous GnRH-a treatment will affect these processes. To further investigate these possibilities, more experiments are needed, for example experiments in which castrated rats will be treated with GnRH agonists.
In conclusion, we have for the first time investigated the effect of the GnRH-a triptorelin on growth in the rat and related it to changes in GH secretion, hepatic GHR, and GHBP. Triptorelin treatment was not as effective as surgical gonadectomy on most parameters tested and affected different aspects of the GH secretory pattern in male and female rats. Triptorelin treatment stimulated growth in female rats, although decreasing their GHBP and baseline GH secretion, but the stimulation of growth might be largely due to a reduction of the direct inhibiting effect of estrogen on growth. Triptorelin treatment had much less impact in males and slightly stimulated growth, although decreasing the amplitude of GH pulses. The stimulation of weight gain by triptorelin in male rats, which is opposite to the effect of surgical gonadectomy and unexpected given the decrease in GH secretion, could indicate an interference of triptorelin in the control of body weight.
Abbreviations
- GnRH:
-
gonadotropin-releasing hormone
- GHR:
-
GH receptor
- GHBP:
-
GH binding protein
- GnRH-a:
-
GnRH analog
- BMI:
-
body mass index
- TIMP-1:
-
tissue inhibitor of metalloproteinase-1
References
Belchetz PE, Plant TM, Nakai Y, Keogh EJ, Knobil E 1978 Hypophyseal response to continuous and intermittent delivery of hypothalamic gonadotropin releasing hormone. Science 202: 631–633
Furr B 1989 Pharmacology of the luteinizing hormone releasing hormone (LHRH) analogue, Zoladex. Horm Res 32( suppl 1): 86–92
Ward JA, Furr BJA, Valcaccia B, Curry B, Bardin CW, Gunsalus GL, Morris ID 1989 Prolonged suppression of rat testis function by a depot formulation of Zoladex, a GnRH agonist. J Androl 10: 478–486
Lerrant Y, Kottler M-L, Bergametti F, Moumni M, Blumberg-Tick J, Counis R 1995 Expression of gonadotropin-releasing hormone(GnRH) receptor gene is altered by GnRH agonist desensitization in a manner similar to that of gonadotropin B subunit genes in normal and castrated rat pituitary. Endocrinology 136: 2803–2808
Conn P, Staley D, Yasumoto T 1987 Homologous desensitization with gonadotropin releasin hormone also diminishes gonadotrope responsiveness to maitotoxin: a role for the GnRH receptor-regulated calcium channel in mediation of cellular desensitization. Mol Endocrinol 1: 154–159
Conn PM 1994 Gonadotropin-releasing hormone and its analogs. Annu Rev Med 45: 391–405
Redding TW, Schally AV, Tice TR, Meyers WE 1984 Long-acting delivery systems for peptides: inhibition of rat prostate tumors by controlled release of [D-Trp6]-luteinizing hormone-releasing hormone from injectable microcapsules. Proc Natl Acad Sci USA 81: 5845–5848
Oerter KE, Manasco P, Barnes KM, Jones J, Hill S, Cutler GBJ 1991 Adult height in precocious puberty after long-term treatment with deslorelin. J Clin Endocrinol Metab 73: 1235–1240
Oostdijk W, Rikken B, Schreuder S, Otten B, Odink R, Rouwe C, Jansen M, Gerver WJ, Waelkens J, Drop S 1996 Final height in central precocious puberty after long-term treatment with a slow-release GnRH-agonist. Arch Dis Childhood 75: 292–297
Job JC, Toublanc JE, Landier F 1994 Growth of short normal children in puberty treated for 3 years with growth hormone alone or in association with gonadotropin-releasing hormone agonist. Horm Res 41: 177–184
Saggese G, Cesaretti G, Barsanti S, Rossi A 1995 Combination treatment with growth hormone and gonadotropin-releasing hormone analogs in short normal girls. J Pediatr 126: 468–473
Balducci R, Toscano V, Mangiantini A, Municchi G, Vaccaro F, Picone S, Di Rito A, Boscherinin B 1995 Adult height in short normal adolescent girls treated with gonadotropin-releasing hormone analog and growth hormone. J Clin Endocrinol Metab 80: 3596–3600
Lindner D, Job JC, Chaussain JL 1993 Failure to improve height prediction in short-stature pubertal adolescents by inhibiting puberty with luteinizing hormone-releasing hormone analogues. Eur J Pediatr 152: 393–396
Dimartino-Nardi J, Wu R, Fishman K, Saenger P 1991 The effect of long-acting analog of luteinizing hormone-releasing hormone on growth hormone secretory dynamics in children with precocious puberty. J Clin Endocrinol Metab 73: 902–906
DiMartino NJ, Wu R, Varner R, Wong WL, Saenger P 1994 The effect of luteinizing hormone-releasing hormone analog for central precocious puberty on growth hormone (GH) and GH-binding protein. J Clin Endocrinol Metab 78: 664–668
Kamp GA, Manasco PK, Barnes KM, Jones J, Rose SR, Hill SC, Cutler GJ 1991 Low growth hormone levels are related to increased body mass index and do not reflect impaired growth in luteinizing hormone-releasing hormone agonist-treated children with precocious puberty. J Clin Endocrinol Metab 72: 301–307
Sklar C, Rothenberg S, Blumberg D, Oberfield SE, Levine LS, David R 1991 Suppression of the pituitary-gonadal axis in children with central precocious puberty: effects on growth, growth hormone, insulin-like growth factor-I and prolactin secretion. J Clin Endocrinol Metab 73: 734–738
Oliveira SB, Donnadieu M, Chaussain JL 1993 Changes in growth hormone-binding protein in girls with central precocious puberty treated with a depot preparation of luteinizing hormone-releasing hormone analogue. Horm Res 39: 42–46
Tannenbaum GS, Martin JB 1976 Evidence for an endogenous ultradian rhythm governing growth hormone secretion in the rat. Endocrinology 98: 562–570
Clark RG, Chambers G, Lewin J, Robinson ICAF 1986 Automated repetitive microsampling of blood: growth hormone secretion in conscious male rats. J Endocrinol 111: 27–35
Clark RG, Carlsson L, Robinson I 1987 Growth hormone secretory profiles in conscious female rats. J Endocrinol 114: 399–407
Maes M, de Hertogh R, Watrin-Granger P, Ketelslegers JM 1983 Ontogeny of liver somatotropic and lactogenic binding sites in male and female rats. Endocrinology 113: 1325–1332
Massa G, Mulumba N, Ketelslegers J-M, Maes M 1990 Initial characterization and sexual dimorphism of serum growth hormone-releasing binding protein in adult rats. Endocrinology 126: 1976–1980
Jansson JO, Eden S, Isaksson OGP 1985 Sexual dimorphism in the control of growth hormone secretion. Endocr Rev 6: 128–150
Carmignac DF, Gabrielsson BM, Robinson ICAF 1993 Growth hormone binding protein (GHBP) in the rat: effects of gonadal steroids. Endocrinology 133: 2445–2452
Hughes P, Tanner J 1970 A longitudinal study of the growth of the blackhooded rat: methods of measurement and rates of growth for skull, limbs, pelvis, nos-rump and tail lengths. J Anat 106: 349–370
Gevers EF, Wit JM, Robinson ICAF 1995 Effect of gonadectomy on growth and GH responsiveness in dwarf rats. J Endocrinol 145: 69–79
Merriam GR, Wachter KW 1982 Algorithms for the study of episodic hormone secretion. Am J Physiol 243:E310–E318
Maiter D, Underwood LE, Maes M, Ketelslegers JM 1988 Acute down-regulation of the somatogenic receptors in rat liver by a single injection of growth hormone. Endocrinology 122: 1291–1296
Lowry O, Rosebrough N, Farr A, Randall R 1951 Protein measurement with the Folin phenol reagent. J Biol Chem 193: 265–275
Gevers EF, Wit JM, Robinson ICAF 1996 Growth, growth hormone (GH)-binding protein and GH receptors are differentially regulated in the rat by peak and trough components of the GH secretory pattern. Endocrinology 137: 1013–1018
Massa GG, Bouillon R, Vanderschueren-Lodewyckx M 1992 Serum growth hormone binding protein and insulin-like growth factor I levels in Turner syndrome before and during treatment with recombinant human growth hormone and ethinylestradiol. J Clin Endocrinol Metab 75: 1298–1302
Postel VM, Tar A, Hocquette JF, Clot JP, Fontoura M, Brauner R, Rappaport R 1991 Human plasma growth hormone (GH)-binding proteins are regulated by GH and testosterone. J Clin Endocrinol Metab 73: 197–202
Clark RG, Carlsson L, Robinson ICAF 1987 Growth hormone secretory profiles in conscious female rats. J Endocrinol 114: 399–407
Jansson JO, Eden S, Isaksson O 1983 Sites of action of testosterone and estradiol on longitudinal bone growth. Am J Physiol 243:E135–E140
Smith EP, Boyd J, Frank GR, Takahashi H, Cohen RM, Specker B, Williams TC, Lubahn DB, Korach KS 1994 Estrogen resistance caused by a mutation in the estrogen-receptor gene in a man. N Engl J Med 331: 1056–1061
Juul A, Scheike T, Nielsen CT, Krabbe S, Muller J, Skakkebaek NE 1995 Serum insulin-like growth factor I (IGF-I) and IGF-I binding protein 3 levels are increased in central precocious puberty: effects of two different treatment regimens with gonadotropin-releasing hormone agonists, without or in combination with an antiandrogen (cyproterone acetate). J Clin Endocrinol Metab 80: 3059–3067
Barash IA, Cheung CC, Weigle DS, Ren H, Kabigting EB, Kuijper JL, Clifton DK, Steiner RA 1996 Leptin is a metabolic signal to the reproductive system. Endocrinology 137: 3144–3147
Painson J, Thorner M, Krieg R, Tannenbaum GS 1992 Short term adult exposure to estradiol feminizes the male pattern of spontaneous and growth hormone-releasing factor-stimulated growth hormone secretion in the rat. Endocrinology 130: 511–519
Ohlsson L, Isaksson O, Jansson JO 1987 Endogenous testosterone enhances growth hormone (GH)-releasing factor induced GH secretion in vitro. J Endocrinol 113: 249–253
Chowen JA, Argente J, GonzalezParra S, GarciaSegura LM 1993 Differential effects of the neonatal and adult sex steroid environments on the organization and activation of hypothalamic growth hormone-releasing hormone and somatostatin neurons. Endocrinology 133: 2792–2802
Werner H, Koch Y, Baldino F, Gozes I 1988 Steroid regulation of somatostatin mRNA in the rat hypothalamus. J Biol Chem 263: 7666–7671
Reichlin S 1992 In: Wilson JD, Foster DW (eds) Williams Textbook of Endocrinology, Saunders, Philadelphia, pp 178
Baumbach WR, Horner DL, Logan JS 1989 The growth hormone-binding protein in rat serum is an alternatively spliced form of the rat growth hormone receptor. Genes Dev 3: 1199–1205
Clark RG, Mortensen DL, Carlsson LMS, Spencer SA, McKay P, Mulkerrin M, Morre J, Cunningham BC 1996 Recombinant human growth hormone(GH)-binding protein enhances the growth promoting activity of human GH in the rat. Endocrinology 137: 4308–4315
Lim L, Spencer SA, McKay P, Waters MJ 1990 Regulation of growth hormone (GH) bioactivity by a recombinant human GH-binding protein. Endocrinology 127: 1287–1291
Sotiropoulos A, Goujon L, Simonin G, Kelly PA, Postel-Vinay MC, Finidori J 1993 Evidence for generation of the growth hormone-binding protein through proteolysis of the growth hormone receptor membrane receptor. Endocrinology 132: 1863–1865
Weissberger AJ, Ho KK, Lazarus L 1991 Contrasting effects of oral and transdermal routes of estrogen replacement therapy on 24-hour growth hormone (GH) secretion, insulin-like growth factor I, and GH-binding protein in postmenopausal women. J Clin Endocrinol Metab 72: 374–381
Maiter D, Lause P, Adam E, Mulumba N, Robinson ICAF 1996 Long-term effects of gonadal hormones on liver IGF-I and GH receptor(GHR)/GH binding protein (GHBP) gene expression in the rat. Proceedings of the 10th International Conference of Endocrinology, San Francisco, Abstract P2-344
Cook J, Doty K, Conn P, Hansen J 1992 Assessment of depot leuprolide acetate dose-adequacy for central precocious puberty. J Clin Endocrinol Metab 74: 1206–1209
Filicori M, Flamigni C, Cognigni G, Dellai P, Arnone R, Falbo A, Capelli M 1993 Comparison of the suppressive capacity of different depot gonadotropin-releasing hormone analogs in women. J Clin Endocrinol Metab 77: 130–133
Orth JM, Gunsalus G, Lamperti AA 1988 Evidence from Sertoli cell-depleted rats indicates that spermatic number in adults depends on numbers of Sertoli cells produced during perinatal development. Endocrinology 122: 787–794
Garnelo P, Pinilla L, Gaytan F, Aguilar E 1992 Pituitary-testis function in rats treated neonatally with a gonadotrophin-releasing hormone agonist: short- and long-term effects. J Endocrinol 134: 269–277
Kolho K-L, Huhtaniemi I 1989 Suppression of pituitary-testis function in rats treated neonatally with a gonadotrophin-releasing hormone agonist and antagonist: acute and long-term effects. J Endocrinol 123: 83–91
Struthers RS, Gaddy KD, Vale WW 1992 Activin inhibits binding of transcription factor Pit-1 to the growth hormone promoter. Proc Natl Acad Sci USA 89: 11451–11455
Boujrad N, Ogwuegbu O, Garnier M, Lee CH, Martin BM, Papadopoulos V 1995 Identification of a stimulator of steroid hormone synthesis isolated from testis. Science 268: 1609–1612
Santen RJ, Demers LM, Max DT, Smith J, Stein BS, Glode LM 1984 Long term effects of a gonadotropin-releasing hormone superagonist analog in men with prostatic carcinoma. J Clin Endocrinol Metab 58: 397–400
Marchetti B, Gallo F, Farinella Z, Romeo C, Morale MC 1996 Luteinizing hormone-releasing hormone receptors in the neuroendocrine-immune network. Annals New York Academy of Sciences 784: 209–236
Stojilkovic SS, Catt KJ 1995 Expression and signal transduction pathways of gonadotropin-releasing hormone receptors. Recent Prog Horm Res 50: 161–205
Pfaff DW, Schwanzel-Fukuda M, Parhar IS, Lauber AH, McCarthy MM, Kow L-M 1994 GnRH neurons and other cellular and molecular mechanisms for simple mammalian reproductive behaviors. Recent Prog Horm Res 49: 1–25
Acknowledgements
The authors thank Anita Mynett for help with some of the experiments, Danielle Carmignac for measuring GHBP, and Organon(The Netherlands) for measuring estrogen levels. We thank Ferring (Malmö, Sweden) for the generous supply of Decapeptyl-CR. We also thank NIDDK for the supply of GH-RIA reagents and Dr. William Baumbach (American Cyanamid Co., Princeton, NJ), Dr. Lena Carlsson and Dr. Ross Clark (Genentech, South San Francisco, CA) for GHBP-RIA reagents. We are grateful to Lyset Rekers for statistical help and to Dr. Wilma Oostdijk for critical advice on preparing the manuscript.
Author information
Authors and Affiliations
Additional information
Supported in part by a grant from the Ter Meulen Fund (Royal Netherlands Academy for Arts and Sciences).
Rights and permissions
About this article
Cite this article
Gevers, E., Wit, JM. & Robinson, I. Effects of Long-Term Gonadotropin-Releasing Hormone Analog Treatment on Growth, Growth Hormone (GH) Secretion, GH Receptors, and GH-Binding Protein in the Rat. Pediatr Res 43, 111–120 (1998). https://doi.org/10.1203/00006450-199801000-00017
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199801000-00017
This article is cited by
-
Choroid plexus aquaporin 1 and intracranial pressure are increased in obese rats: towards an idiopathic intracranial hypertension model?
International Journal of Obesity (2017)
-
Aromatase inhibitors in pediatrics
Nature Reviews Endocrinology (2012)
