
Abstract
Death from some childhood disorders such as sudden infant death syndrome and the congenital long QT syndrome are associated with specific behaviors such as sleep or emotional stress. We studied young German shepherd dogs that die suddenly during presumed sleep. These dogs have inherited ventricular tachycardia (VT) which is most frequent during sinus bradycardia and sinus arrhythmia. We hypothesized that the number of VT complexes (three or more consecutive ectopic complexes) would be greatest during sleep. Moreover, we hypothesized that pauses in the sinus rhythm of greater than 1000 ms would be greatest in the behavior with the most frequent VT. Behavioral states[excited, ambulatory, sitting, lying, rapid eye movement (REM) sleep] were quantified from 24-h video recordings of seven dogs. VT and pauses were quantified for each behavior using simultaneously recorded ECGs. A multivariate model was used to analyze the results. After controlling for time of day, lying, and REM sleep were significantly (p < 0.02) associated with VT, whereas more active behaviors were not. Time of day also independently affected the number of VT complexes. However, behavior and time of day did not account for all of the variability in the number of VT complexes. Pauses were significantly associated with behavior, with the highest number of pauses occurring during lying and REM sleep. However, pauses were not always associated with VT, indicating that a pause was a necessary, but not sufficient, condition for the development of VT. These results suggest that modulation of VT incidence in these animals is multifactorial and that the highest number of VT complexes is associated with the bradycardia that accompanies REM sleep.
Similar content being viewed by others


Main
The circumstances of death for children who die of the long QT syndrome(1, 2) and infants who die of SIDS(3–6) tend to implicate the autonomic nervous system. Heterogeneous sympathetic innervation to the heart has been identified in patients with the long QT syndrome(7), and abnormal development of the neuronal innervation of the heart has been suggested to underlie some cases of SIDS(5, 6, 8). Evidence from studies of heart rate variability in infants who have died of SIDS(9–12) has prompted others to consider an autonomic disturbance that either causes cardiac instability or reflects CNS alterations which have the potential to affect vital functions(9). Sleep is not a passive state(13), and during certain stages such as REM sleep, the dominant parasympathetic tone is interrupted by bursts of sympathetic tone(14, 15). Consequently, disturbances in cardiac rhythm influenced by imbalances in autonomic tone may be exacerbated during such stages of sleep.
We have established a colony of German shepherd dogs that die suddenly during presumed sleep usually between 4 and 8 mo of age(16). Postmortem examination has not revealed a cause of death, although heterogeneous sympathetic innervation of the ventricles has been identified(17). Spontaneous VT develops in these dogs at approximately 4 mo of age(16, 18). The maturational age of these dogs at the time of death is similar to the age at which some children die with presumed long QT syndrome(2), but older than the age at which infants succumb to SIDS(3, 9). However, VT can be induced in these dogs as young as 7 wk of age if the heart rate is slowed sufficiently (our unpublished observation) Therefore, the potential exists for VT and sudden death at an early age in these animals, but it may be suppressed by the elevated heart rate of the very young dog. We suspect that VT is a prodrome for sudden death. Because VT in these dogs is more prevalent with bradycardia, it seems likely that behavior contributes to the generation of VT by affecting heart rate. Therefore, the primary objective of this study was to evaluate the effect of behavioral state (excited, ambulatory, sitting, lying, REM sleep) on the number of pauses (RR intervals greater than 1000 ms) and VT complexes to determine whether pauses were more frequent during the behavioral state with the highest number of VT complexes.
METHODS
Animals. Animals used in this study were housed in an American Association for the Accreditation of Laboratory Animal Care approved facility which conforms to the guidelines for proper animal care as described within the National Institutes of Health Guide for the Care and Use of Laboratory Animals. Experiments were approved by the Institutional Animal Care and Use Committee of the Center for Research Animal Resources at Cornell University. Seven German shepherd dogs (four females and three males between the ages of 20 and 28 wk) with VT were studied. Each of these dogs was from the colony in which ventricular arrhythmias and sudden death had occurred(19).
Dogs were studied individually in the usual housing for these animals. Dogs were housed in large runs, but each could see and hear others within a large facility that housed 30 dogs. Fourteen hours of consistent light were provided with 10 h of dark. Because of the adequate size of the runs, dogs were not routinely walked outside, except on occasion and not during the monitoring period. Feeding was ad libitum. Food containers were filled at 0800 h, and cleaning of the facility was performed at the same time for each dog.
Monitoring of behavior. At the historical peak age of sudden death, the activity of each of the seven dogs was monitored for a single 24-h period with a time lapse video tape recordings (Panasonic Time Lapse VCR AG6030, Japan) using a camera (Panasonic model WV 1500X, Japan) with wide conversion lens. An additional camera was positioned to record a telemetry ECG(Hewlett Packard, Bosie, ID). A screen splitter displayed and recorded the image of the dog and the ECG simultaneously and superimposed a 24-h clock(accuracy to 0.1 s). The ECG recorded with the telemeterized signal was a left precordial lead (V5) which presented normal sinus QRS complexes with a positive polarity. Concurrently, a 24-h ambulatory ECG recording (Holter monitoring) was obtained using the X, Y, Z lead configuration. Leads for the ECG were attached via electrode patches adhered to the skin after shaving the left, right, and ventral thorax with an isolated area over approximately the 7th vertebra. The lead wires, Holter monitor, and telemetry transmitter were secured to the dog's body with gauze, tape (Elasticon; Johnson and Johnson, Arlington, TX), and a fitted vest (Four Flags Over Aspen, Jamesville, MN). Each of the dogs studied had numerous (minimum of 10) 24-h Holter monitoring periods since 8 wk of age; therefore, the dogs were familiar with the procedure and the equipment.
The dog's behavior during the entire 24-h video tape was identified by trained observers (D.B., S.E., D.A.D.). These observers worked in pairs in the examination of the behaviors. Rarely, the third observer resolved any disagreements. To avoid bias the behavioral state of the dogs was identified, and the time spent in that behavior was quantified before and without knowledge of the quantification of the ventricular arrhythmias to avoid bias. Behavior classification included five states: excited, ambulatory, sitting, lying, and REM sleep. Excited behavior involved jumping, barking, running, and vigorous tail wagging. The ambulatory state included walking, standing, prehending, defecating, and urinating. Sitting required that the haunches only be on the ground. Lying was defined as sternal, lateral, or dorsal recumbency. The category lying included both awake and non-REM sleep states.
One of us (A.R.M.) has shown previously that observational identification of certain sleep states, including REM sleep, correlates with identification of such sleep states using simultaneous polygraphic recordings(20). REM sleep that could be identified only by behavioral observation, as described by A.R.M.(20) and others(21–24), was classified as such. REM sleep was identified on the basis of peripheral muscle twitches. These twitches were seen as rapid, involuntary, spastic movements of isolated muscle groups, mainly the toes, paws, ears, and tail. Occasionally the entire head or a pair of legs were observed to twitch and could be classified as such if the movement was involuntary and rapid. REM sleep was conservatively defined as the time between at least two consecutive twitches, despite the probable existence of REM sleep before and after these observed movements. Stipulations for classifying REM sleep included the absence of obvious wakefulness and stretches between twitches. Stretches were indicative of wakefulness, arousal, or non-REM sleep and were often observed after a REM episode or preceding wakefulness. Stretching movements were slow and included isolated limbs or the whole body of the dog.
Classification of arrhythmias. For every behavior throughout the 24-h period the type of ventricular arrhythmia was quantified manually by trained observers (D.B., S.E., D.A.D., W.J.F.). In three dogs (s90, s85, s99) arrhythmias were classified and quantified as single PVC (singles), two consecutive PVC (couplets), or three or more consecutive PVC (VT). In four dogs (s87, s88, s104, s110) only the complexes of the VT were quantified. For each behavioral state for all other dogs, the type and number of ventricular arrhythmias were determined for the entire 24-h period. Only the VT data were analyzed statistically.
As these dogs were examined at the age of peak arrhythmia incidence, it was not possible to evaluate accurately the sinus heart rate and heart rate variability or to derive respiration from the ECGs because of the frequent arrhythmias (Fig. 1). In lieu of these measurements, we determined the relationships between pauses (long RR intervals) in the cardiac rhythm, behavior, and number of VT complexes. RR intervals of greater than 1000 ms were defined as pauses and quantified for each behavioral state using four epochs (one each at 0000-0600, 0601-1200, 1201-1800, and 1801-2400 h) of 2.5 min (10 min total).

Three channel ambulatory electrocardiographic recording from dog s80 during the lying behavior. The large number of ventricular arrhythmias in dogs at this age precluded the accurate determination of heart rate variability. Note time of day for the recording on the left.
Statistical analysis. The effect of each behavior on VT was evaluated using the general linear model in SAS(25). Because we hypothesized that VT might vary both by behavior and time of day, we evaluated the effect of behavior, controlling for the time of day in a multivariate model (see below). The number of VT complexes was adjusted for the amount of time spent in each behavior and expressed as the number of VT complexes/h. For example, if the animal had 2.4 h of REM sleep during the 24-h monitoring period, and 2400 VT complexes were counted during this behavior, this was expressed as 1000 VT complexes/h for REM sleep. The number of VT complexes/h for each behavior was determined for each individual dog. To evaluate the hourly number of VT complexes for the dogs as a group in the model, it was necessary to transform this number using natural logarithms to normalize their distribution. To avoid the computational problem in the transformation of zero VT values during some hours for some of the dogs, one was added to all VT counts. Time of day was transformed using a second order polynomial to control for the trend of VT over time, because VT did not have a linear relationship with time of day. To accurately account for the behavior during each hour in the analysis, each behavior was expressed as a proportion of the time spent in that behavior. A variable for dog was included to control for the variability among dogs in the analysis, because the number of VT complexes/h was not normally distributed. The model was specified as follows: Equation where Y = number of VT complexes(logarithmic scale); μ = intercept (average VT irrespective of the other variables); α = the effect of REM on VT; β = the effect of lying on VT; γ = the effect of sitting on VT; δ = the effect of excitement on VT; Θ = the effect of ambulatory on VT; κ = the effect of hour of the day on VT; ω = the effect of hour of the day squared on VT(adjustment for the nonlinear relationship of hour to VT); ρ = the effect of dog on VT; ε = error term.

The pause data were analyzed using the Friedman test, a two-way analysis of variance by ranks for matched samples followed by the Wilcoxin signed rank test with a significance placed at p < 0.02.
RESULTS
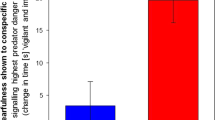
The number of VT complexes was highly dependent on behavior, as illustrated in Figure 2, where examples of the lack of VT during excitement, the emergence of PVC during ambulatory behavior, and the marked development of VT during REM sleep are given. Figure 3A shows the relationship between different behavioral states and VT for all seven dogs, using data that have been adjusted for time spent in each behavior(see Table 1). In general, the number of VT complexes increased as the behavioral state became less active. Additionally, VT occurred immediately after the dogs went from ambulatory behavior to the sitting position.

Three channel ambulatory electrocardiographic recording from dog s88. Ventricular arrhythmias were rare with excitement and infrequent with ambulating, but were frequent during periods of lying or REM sleep VT. The VT was rapid, polymorphic, and nonsustained. This dog was found dead at first observation in the morning at the age of 11 mo. Note time of day for the recording on the left.

The number of VT complexes adjusted for the time spent in each of five behaviors (number of VT complexes/h). All seven dogs had the greatest number of VT complexes (A) and pauses (B) during REM sleep.
The number of pauses also was significantly associated with behavior(p < 0.002), although the comparisons between pairs of behavioral states did not reach statistical significance because of the small sample size. Each dog had progressively more pauses (least to most) during the behaviors: excited, ambulatory, sitting, lying, and REM sleep(Fig. 3B). However, there was no significant association between the number of pauses and the number of VT complexes across dogs. That is, the dogs with the greatest number of pauses were not necessarily the dogs with the most frequent VT and vice versa.
The number of VT complexes was not uniform throughout the day, but reached a minimum at approximately 1900 h and a maximum at approximately 0600 h(Fig. 4). As discussed below, the variation of VT incidence with time of day could not be explained entirely by parallel variations of behavior with time of day. Consequently, a separate term for time of day, derived from an analysis of these data, was included in the multivariate model.

Twenty-four hour distribution of VT in seven dogs with inherited predisposition for sudden death. A nonuniform distribution of the number of VT complexes was observed. Hourly transformed (natural logarithm) means of ventricular complexes are given with bars indicating SEM. One was added to all counts of VT/h to avoid the computational problem of negative natural logarithm.
Although the number of VT complexes increased with decreased activity, the incidence of single PVC was not correlated consistently with behavioral state, as illustrated in Figure 5. Couplets, however, did tend to be more closely correlated with VT across behavioral states(Fig. 5).

Graphs of three individual dogs (s80, s85, and s99) and the incidence of ventricular arrhythmias classified as single premature ventricular complexes (singles), two consecutive premature complexes(couplets), and three or more consecutive premature complexes (VT). Couplets and VT were similar in their distribution with respect to behavior state, but singles were not consistent within each dog.
In the multivariate model, after controlling for time of day, the behaviors REM sleep and lying were significantly associated with the number of VT complexes, whereas the behaviors of sitting, ambulatory, and excited were not(Table 2). The analysis indicated that both behavior and time of day had significant independent effects on the number of VT complexes(Table 2). The model explained 40% (r = 0.40) of the variability in the number of VT complexes and, therefore, suggested that there were other factors that influenced the number of VT complexes. Sinus heart rate and the number of pauses were not included in the model because it was not possible to quantify either over 24 h.
DISCUSSION
In this study the number of VT complexes in German shepherd dogs with inherited sudden death was highest during lying and REM sleep. This result is consistent with the observation that these animals die most frequently during observed or presumed sleep(16). Previous studies in humans have indicated that sleep typically is associated with a suppression of ventricular arrhythmias(26–28), possibly reflecting an antiarrhythmic effect of increased parasympathetic tone and decreased sympathetic tone(29). However, cardioprotection may not be a generalized feature of sleep, given that the balance of parasympathetic and sympathetic tone can be quite complex(13, 14), particularly during REM sleep and some periods of slow-wave sleep(26). Consequently, during REM sleep sinus pauses, bradycardia, and tachycardia may occur, depending on the instantaneous variations in autonomic dynamics(30–32).
The number of VT complexes also was high in these dogs during the transition from ambulatory to a sitting position. This postural change was accompanied by bradycardia, probably resulting from a transient increase in blood pressure. As expected, bradycardia facilitated the development of pausedependent VT. In contrast, VT did not occur during periods of excitement, and only limited episodes of VT occurred during ambulatory behavior. Excitement and ambulating presumably would be accompanied by elevated sympathetic tone and vagal withdrawal, resulting in fewer sinus pauses and suppression of VT.
Time of day was found to significantly, and independently, affect the number of VT complexes. This result may relate to the observation that heart rate variability is a function not only of sleep-state, but also of the time of night(12). On the other hand, according to the multivariate model, behavioral state and time of day accounted for only part of the variation in VT incidence in these animals, suggesting that other factors, such as heart rate, might independently influence the propensity for VT. Although determination of the sinus heart rate and heart rate variability during each behavior would have been desirable, the presence of ventricular arrhythmias in these dogs precluded such measurements. Using pauses as a surrogate for sinus bradycardia, we found that the number of pauses was high during those behaviors associated with the highest number of VT complexes, yet there was little correlation between the number of pauses and the number of VT complexes in any given dog. This result suggests that pauses were necessary for the induction of VT, but that other factors, which remain to be identified, were required as well.
The pause-dependence of the arrhythmias in these animals may relate to the observation that the underlying mechanism for the arrhythmias is most likely EAD-induced triggered activity(33). It has been proposed that a similar mechanism may account for the pause-dependent arrhythmias in patients with the long QT syndrome(34–39). Our hypothesis that EAD-induced triggered activity is responsible for the initiation of VT is based on the observation that EAD occur spontaneously in Purkinje fibers excised from the left ventricles of affected dogs. Studies using metaiodobenzylguanidine scintigraphy and immunocytochemical histology have indicated that the regions of the left ventricle from which these Purkinje fibers are obtained lack normal sympathetic innervation(17). The specific relationship between sympathetic denervation and the generation of EAD has not been established. However, there is evidence from other studies that the autonomic nervous system influences the development of EAD and VT. Specifically, we have shown thatα1-adrenergic stimulation with phenylephrine potentiates VT in intact dogs(19) and increases the incidence of the EAD in isolated Purkinje fibers(33). The potentiation of VTin vivo results from a baroreflex-mediated sinus bradyeardia and from a direct arrhythmogenic effect on the ventricle. The latter may involve enhancement of EAD(36), possibly resulting from inhibition of the potassium channels lk(40) or lto(41). Thus, the development of VT in these dogs is facilitated by the combination of a slow heart rate, secondary to enhanced vagal tone, andα1-adrenergic stimulation. Perhaps a similar balance of autonomic tone exists during certain periods of sleep, particularly if sleep occurs at a specific time of day. Pauses generated during such a period of sleep might be more likely to initiate VT than pauses generated during other behaviors.
Correlations of specific sleep stages with the number of VT complexes were not possible in this study because sleep stages were not characterized beyond the video-based identification of REM sleep. It is likely that during the period of lying the animals were having periods of quiet sleep and transitions between quiet sleep. REM sleep and arousal. Although observation can be used to identify REM sleep, both in animals(20, 22) and in humans(42), more precise information regarding sleep state would require EEG. In future studies it might be worthwhile to identify specific sleep states, to determine whether sleep state per se influences the development of VT. Perhaps more importantly, it would be useful to monitor indices of parasympathetic and sympathetic tone(α1-adrenergic tone in particular), to determine the status of the autonomic nervous system during any particular behavior, and whether specific alterations in autonomic tone predispose to the development of VT.
Abbreviations
- VT:
-
ventricular tachycardia
- REM:
-
rapid eye movement
- SIDS:
-
sudden infant death syndrome
- PVC:
-
premature ventricular complex
- EAD:
-
early afterdepolarization
References
Villain E, Levy M, Kachaner J, Garson A Jr 1992 Prolonged QT interval in neonates: benign, transient, or prolonged risk of sudden death. Am Heart J 124: 194–197
Schwartz PJ, Locati EH, Moss AJ, Crampton RS, Trazzi R, Ruberti U 1991 Left cardiac sympathetic denervation in the therapy of congenital long QT syndrome: a worldwide report. Circulation 84: 503–511
Schwartz PJ 1987 The quest for the mechanisms of the sudden infant death syndrome: doubts and progress. Circulation 75: 677–683
Verrier RL, Kirby DA 1988 Sleep and cardiac arrhythmias. Ann NY Acad Sci 533: 238–251
Schwartz PJ 1976 Cardiac sympathetic innervation and the sudden infant death syndrome: a possible pathogenic link. Am J Med 60: 167–172
Stramba-Badiale M, Lazzarotti M, Schwartz PJ 1992 Development of cardiac innervation, ventricular fibrillation, and sudden infant death syndrome. Am J Physiol 263:H1514–H1522
Muller K, Jakob H, Neuzner J, Grege S, Schlepper M, Pitschner H 1993 123I-metaiodobenzylguanidine scintigraphy in the detection of irregular regional sympathetic innervation in long QT syndrome. Eur Heart J 14: 316–325
Stramba-Badiale M, Spagnolo D, Schwartz PJ 1996 Neonatal ECG for QT interval measurement: a feasible predictive test for SIDS. In: Rognum TO (ed) Sudden Infant Death Syndrome: New Trends for the Nineties. Scandinavian University Press, Oslo ( in press)
Schechtman VL, Raetz SL, Harper RK, Garfinkel A, Wilson AJ, Southhall DP, Harper RM 1992 Dynamic analysis of cardiac R-R intervals in normal infants who subsequently succumbed to the sudden infant death syndrome. Pediatr Res 31: 606–612
Schechtman VL, Harper RK, Harper RM 1993 Development of heart rate dynamics during sleep-waking states in normal infants. Pediatr Res 34: 618–623
Schechtman VL, Harper RM, Kluge KA, Wilson AJ, Hoffman HJ, Southhall DP 1989 Heart rate variation in normal infants and victims of sudden infant death syndrome. Early Hum Dev 19: 167–181
Schechtman VL, Harper RM 1991 Time of night effects on heart rate variation in normal neonates. J Dev Physiol 16: 349–353
Morrison AR 1988 Sleep arousal and motor control. In: Harper RM, Hoffman HJ (eds) Sudden Infant Death Syndrome: Risk Factors and Basic Mechanisms. PMA Publications, New York, pp 347–359
Somers VK, Phil D, Dyken ME, Mark AL, Abboud FM 1993 Sympathetic-nerve activity during sleep in normal subjects. N Engl J Med 328: 303–307
Mancia G 1993 Autonomic modulation of the cardiovascular system during sleep. N Engl J Med 328: 347–349
Moïse NS, Meyers-Wallen V, Flahive WJ, Valentine BA, Scarlett JM, Brown CA, Chavkin MJ, Dugger DA, Renaud-Farrell S, Kornreich B, Schoenborn WCD, Sparks JR, Gilmour RF Jr 1994 Inherited ventricular arrhythmias and sudden death in German shepherd dogs. J Am Coll Cardiol 24: 233–243
Dae M, Ursell PC, Lee RJ, Stilson C, Chin M, Moïse NS 1995 Heterogenous sympathetic innervation in German shepherd dogs with inherited ventricular arrhythmias and sudden death. J Am Coll Cardiol 20:A
Riccio ML, Gilmour RF Jr, Flahive WJ, Moïse NS 1994 The nonrandom patterning of beat types and time intervals preceding ventricular tachycardia in German shepherd dogs with inherited sudden death. Upstate New York Cardiac Electrophysiology Society 5:A
Moïse NS, Moon PF, Flahive WJ, Brittain D, Lewis BA, Lee RJ, Gilmour RF Jr 1996 Phenylephrine induced ventricular arrhythmias in German shepherd dogs with inherited sudden death. J Cardiovasc Electrophysiol 7: 217–230
Squires LJ, Morrison AR 1981 Sleep cycle lengths determined behaviorally in the family felidae. Sleep Res 10: 121
Hendricks JC, Kline LR, Kovalski, O'Brien JA, Morrison AR, Pack AI 1987 The English bulldog: a natural model of sleep-disordered breathing. J Appl Physiol 63: 1344–1350
Hendricks JC, Lager A, O'Brien D, Morrison AR 1989 Movement disorders during sleep in cats and dogs. J Am Vet Med Assoc 194: 686–689
Thoman EB, Zeidner LP, Denenberg VH 1981 Cross-species invariance in state-related motility patterns. Am J Physiol 241:R312–R315
Zeidner LP, Denenberg VH, Thoman EB, Weyand T 1983 Comparisons of behavioral, motoric, and electrical criteria for assessment of sleep-wake states in the rabbit. Physiol Behav 31: 273–278
SAS Institute, Inc 1985 SAS Users Guide: Statistics, Version 5. SAS Institute, Cary, NC, pp 431–506
Lown B, Tykocinski M, Garfein A, Brooks P 1973 Sleep and ventricular premature beats. Circulation 48: 691–701
Pickering TG, Goulding L, Cobern BA 1977 Diurnal variations in ventricular ectopic beats and heart rate. Cardiovasc Med 2: 1013–1022
Pickering TG, Johnston J, Honour AJ 1978 Comparison of the effects of sleep, exercise, and autonomic drugs on ventricular extra systoles using ambulatory monitoring of electrocardiogram and electroencephalogram. Am J Med 65: 575–583
Baccelli G, Guazzi M, Mancia G, Zanchetti A 1969 Neural and nonneural mechanisms influencing circulation during sleep. Nature 223: 184–185
Dickerson LW, Huang AH, Nearing BD, Verrier RL 1993 Primary coronary vasodilation associated with pauses in heart rhythm during sleep. Am J Physiol 264:R186–R196
Kirby DA, Verrier RL 1989 Differential effects of sleep stage on coronary hemodynamic function. Am J Physiol 256:H1378–H1383
Verrier RL, Dickerson LW 1991 Autonomic nervous system and coronary blood flow changes related to emotional activation and sleep. Circulation 83: 1181–1189
Gilmour RF, Moise NS 1996 Triggered activity as a mechanism for inherited ventricular arrhythmias in German shepherd dogs. J Am Coll Cardiol 27: 1526–1533
Kadish AH, Morady F 1990 Torsade de pointes. In: Zipes DP, Jalife J (eds) Cardiac Electrophysiology from Cell to Bedside. WB Saunders, Philadelphia, pp 605–610
El-Sherif N, Zeiler RH, Craelius W, Gough WB, Henkin R 1988 QTU prolongation and polymorphic ventricular tachyarrhythmias due to bradycardia dependent early after-depolarizations. Circ Res 63: 286–305
Ben David J, Zipes DP 1988 Differential response to right and left ansae subclaviae stimulation of early afterdepolarizations and ventricular tachycardia induced by cesium in dogs. Circulation 78: 1241–1250
Patterson E, Szabo B, Scherlag BJ, Lazzara R 1990 Early and delayed afterdepolarizations associated with cesium chloride induced arrhythmias in the dog. J Cardiovasc Pharmacol 15: 323–331
Hanich RF, Levine JH, Spear JF, Moore EN 1988 Autonomic modulation of ventricular arrhythmia in cesium chloride induced long QT syndrome. Circulation 77: 1149–1161
Antzelevitch C, Sicouri S 1994 Clinical relevance of cardiac arrhythmias generated by afterdepolarizations: role of M cells in the generation of U waves, triggered activity and torsade de pointes. J Am Coll Cardiol 24: 259–277
Lee JH, Rosen MR 1994 Alpha-adrenergic receptor modulation of repolarization in canine Purkinje fibers. J Cardiovasc Electrophysiol 5: 232–240
Fedida D, Shimoni Y, Giles R 1990 Alpha-adrenergic modulation of the transient outward current in rabbit atrial myocytes. J Physiol 423: 257–277
Anders T, Sostek-Miller A 1976 The use of time lapse video recording of sleep-wake behavior in human infants. Psychophysiology 13: 155–158
Author information
Authors and Affiliations
Additional information
Supported by National Institute of Child Health and Human Development, U.S. Public Health Service, Grant HD 23938.
Rights and permissions
About this article
Cite this article
Moïse, N., Dugger, D., Brittain, D. et al. Relationship of Ventricular Tachycardia to Sleep/Wakefulness in a Model of Sudden Cardiac Death. Pediatr Res 40, 344–350 (1996). https://doi.org/10.1203/00006450-199608000-00025
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199608000-00025
