
Abstract
Background:
Active surveillance (AS) has excellent short to medium term outcomes in well-selected prostate cancer patients. Traditional biopsy-based selection criteria have been criticized for inaccurate determination of cancer grade and extent. We evaluated the incremental benefit of multiparametric magnetic resonance imaging (mpMRI) in patient selection using various AS criteria.
Methods:
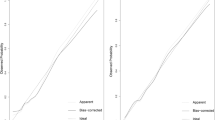
We retrospectively evaluated men who received mpMRI before radical prostatectomy between 2011 and 2014. Patients were classified as suitable for AS using four criteria: (1) Epstein, (2) National Comprehensive Cancer Network (NCCN) low-risk or (3) extended criteria (Gleason ⩽3+4, PSA ⩽15 ng/ml, clinical stage ⩽T2b) using clinical parameters. The incremental value of mpMRI was evaluated against the referent standard of surgical pathology in determining suitability for AS using sensitivity, specificity, likelihood ratios (LRs) and area under receiver operating curves (AUCs).
Results:
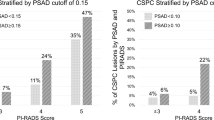
We evaluated 208 men. Only one man fulfilled Epstein criteria (1) at pathology, who was neither identified using clinical criteria nor mpMRI. Using (2), clinical criteria had a sensitivity of 80%, specificity 75%, LR+ 3.3, LR− 0.3, AUC 0.78, while combined clinical-mpMRI criteria achieved a sensitivity of 80%, specificity 99.5% (P<0.01), LR+ 162, LR− 0.2 and AUC 0.90 (P<0.01 compared to clinical). Using (3), clinical criteria had a sensitivity of 74%, specificity 47%, LR+ 1.4, LR− 0.6, AUC 0.60, while combined clinical-mpMRI criteria achieved a sensitivity of 26% (P<0.01), specificity 97% (P<0.01), LR+ 8.3, LR− 0.8 and AUC 0.62 (P=0.85).
Conclusions:
Addition of mpMRI significantly improved selection of men for AS using NCCN low-risk criteria. For selecting men with limited prognostic grade group 2, mpMRI significantly improved specificity at the expense of sensitivity.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C et al. GLOBOCAN 2012 v1.0, Cancer incidence and mortality worldwide: IARC CancerBase No. 11., Lyon, France: International Agency for Research on Cancer. Available at: http://globocan.iarc.fr.
Donovan JL, Hamdy FC, Lane JA, Mason M, Metcalfe C, Walsh E et al. Patient-reported outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med 2016; 375: 1425–1437.
Epstein JI, Walsh PC, Carmichael M, Brendler CB . Pathologic and clinical findings to predict tumor extent of nonpalpable (stage T1c) prostate cancer. JAMA 1994; 271: 368–374.
Choo R, Klotz L, Danjoux C, Morton GC, DeBoer G, Szumacher E et al. Feasibility study: watchful waiting for localized low to intermediate grade prostate carcinoma with selective delayed intervention based on prostate specific antigen, histological and/or clinical progression. J Urol 2002; 167: 1664–1669.
Klotz L, Vesprini D, Sethukavalan P, Jethava V, Zhang L, Jain S et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol 2015; 33: 272–277.
Tosoian JJ, Mamawala M, Epstein JI, Landis P, Wolf S, Trock BJ et al. Intermediate and longer-term outcomes from a prospective active-surveillance program for favorable-risk prostate cancer. J Clin Oncol 2015; 33: 3379–3385.
Tay KJ, Mendez M, Moul JW, Polascik TJ . Active surveillance for prostate cancer: can we modernize contemporary protocols to improve patient selection and outcomes in the focal therapy era? Curr Opin Urol 2015; 25: 185–190.
Klotz L, Zhang L, Lam A, Nam R, Mamedov A, Loblaw A . Clinical results of long-term follow-up of a large, active surveillance cohort with localized prostatecancer. J Clin Oncol 2010; 28: 126–131.
Hamdy FC, Donovan JL, Lane JA, Mason M, Metcalfe C, Holding P et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 2016; 75: 1415–1424.
Gupta RT, Brown AF, Silverman RK, Tay KJ, Madden JF, George DJ et al. Can radiologic staging with multiparametric MRI enhance the accuracy of the Partin tables in predicting organ-confined prostate cancer? AJR Am J Roentgenol 2016; 207: 87–95.
Arumainayagam N, Ahmed HU, Moore CM, Freeman A, Allen C, Sohaib SA et al. Multiparametric MR imaging for detection of clinically significant prostate cancer: a validation cohort study with transperineal template prostate mapping as the reference standard. Radiology 2013; 268: 761–769.
Moore CM, Giganti F, Albertsen P, Allen C, Bangma C, Briganti A et al. Reporting magnetic resonance imaging in men on active surveillance for prostate cancer: the PRECISE Recommendations—a report of a European School of Oncology Task Force. Eur Urol 2017; 71: 648–655.
Gupta RT, Faridi KF, Singh AA, Passoni NM, Garcia-Reyes K, Madden JF et al. Comparing 3- T multiparametric MRI and the Partin tables to predict organ-confined prostate cancer after radical prostatectomy. Urol Oncol 2014; 32: 1292–1299.
ACR. PI-RADS: Prostate Imaging - Reporting and Data System version 2, 2015. Available at: http://www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/PIRADS/PIRADS%20V2.pdf.
Hambrock T, Somford DM, Huisman HJ, van Oort IM, Witjes JA, Hulsbergen-van de Kaa CA et al. Relationship between apparent diffusion coefficients at 3.0- T MR imaging and Gleason grade in peripheral zone prostate cancer. Radiology 2011; 259: 453–461.
Somford DM, Hambrock T, Hulsbergen-van de Kaa CA, Futterer JJ, van Oort IM, van Basten JP et al. Initial experience with identifying high-grade prostate cancer using diffusion-weighted MR imaging (DWI) in patients with a Gleason score </= 3+3=6 upon schematic TRUS-guided biopsy: a radical prostatectomy correlated series. Invest Radiol 2012; 47: 153–8.
Woo S, Kim SY, Cho JY, Kim SH . Preoperative evaluation of prostate cancer aggressiveness: using ADC and ADC ratio in determining Gleason score. AJR Am J Roentgenol 2016; 207: 114–120.
Fitzsimons NJ, Sun LL, Dahm P, Moul JW, Madden J, Gan TJ et al. A single-institution comparison between radical perineal and radical retropubic prostatectomy on perioperative and pathological outcomes for obese men: an analysis of the Duke Prostate Center database. Urology 2007; 70: 1146–1151.
Kryvenko ON, Carter HB, Trock BJ, Epstein JI . Biopsy criteria for determining appropriateness for active surveillance in the modern era. Urology 2014; 83: 869–874.
Mohler JL, Armstrong AJ, Bahnson RR, D'Amico AV, Davis BJ, Eastham JA et al. Prostate cancer, version 1.2016. J Natl Compr Canc Netw 2016; 14: 19–30.
Jaeschke R, Guyatt GH, Sackett DL . Users' guides to the medical literature. III. How to use an article about a diagnostic test. B. What are the results and will they help me in caring for my patients? The Evidence-Based Medicine Working Group. JAMA 1994; 271: 703–707.
Da Rosa MR, Milot L, Sugar L, Vesprini D, Chung H, Loblaw A et al. A prospective comparison of MRI-US fused targeted biopsy versus systematic ultrasound-guided biopsy for detecting clinically significant prostate cancer in patients on active surveillance. J Magn Reson Imaging 2015; 41: 220–225.
Somford DM, Hoeks CM, Hulsbergen-van de Kaa CA, Hambrock T, Futterer JJ, Witjes JA et al. Evaluation of diffusion-weighted MR imaging at inclusion in an active surveillance protocol for low-risk prostate cancer. Invest Radiol 2013; 48: 152–157.
Henderson DR, de Souza NM, Thomas K, Riches SF, Morgan VA, Sohaib SA et al. Nine-year follow-up for a study of diffusion-weighted magnetic resonance imaging in a prospective prostate cancer active surveillance cohort. Eur Urol 2016; 69: 1028–1033.
Porpiglia F, Cantiello F, De Luca S, De Pascale A, Manfredi M, Mele F et al. Multiparametric magnetic resonance imaging and active surveillance: how to better select insignificant prostate cancer? Int J Urol 2016; 23: 752–757.
Donati OF, Mazaheri Y, Afaq A, Vargas HA, Zheng J, Moskowitz CS et al. Prostate cancer aggressiveness: assessment with whole-lesion histogram analysis of the apparent diffusion coefficient. Radiology 2014; 271: 143–152.
Rosenkrantz AB, Triolo MJ, Melamed J, Rusinek H, Taneja SS, Deng F-M . Whole-lesion apparent diffusion coefficient metrics as a marker of percentage Gleason 4 component within Gleason 7 prostate cancer at radical prostatectomy. J Magn Reson Imaging 2015; 41: 708–714.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Prostate Cancer and Prostatic Diseases website
Rights and permissions
About this article

Cite this article
Tay, K., Gupta, R., Holtz, J. et al. Does mpMRI improve clinical criteria in selecting men with prostate cancer for active surveillance?. Prostate Cancer Prostatic Dis 20, 323–327 (2017). https://doi.org/10.1038/pcan.2017.20
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pcan.2017.20
This article is cited by
-
Perspective: a critical assessment of PI-RADS 2.1
Abdominal Radiology (2020)
-
MRI in active surveillance: a critical review
Prostate Cancer and Prostatic Diseases (2019)
-
New prostate cancer prognostic grade group (PGG): Can multiparametric MRI (mpMRI) accurately separate patients with low-, intermediate-, and high-grade cancer?
Abdominal Radiology (2018)
