
Abstract
Background:
Erectile dysfunction (ED) represents one of the most common long-term side effects in prostate cancer (PCa) patients treated with bilateral nerve-sparing radical prostatectomy (BNSRP). The aim of our study was to assess the influence of non-surgically related causes of ED in patients treated with BNSRP.
Methods:
Overall, 716 patients treated with BNSRP were retrospectively identified. All patients had complete data on erectile function (EF) assessed by the Index of Erectile Function-EF domain (IIEF-EF) and depressive status assessed by the Center for Epidemiologic Studies-Depression (CES-D) questionnaire. EF recovery was defined as an IIEF-EF of ⩾22. Kaplan–Meier analyses assessed the impact of preoperative IIEF-EF, depression and adjuvant radiotherapy (aRT) on the time to EF recovery. Multivariable Cox regression models were used to test the impact of aRT on EF recovery after accounting for depression and baseline IIEF-EF.
Results:
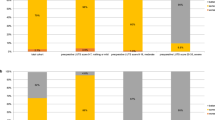
Median follow-up was 48 months. Patients with a preoperative IIEF-EF of ⩾22 had substantially higher EF recovery rates compared with those with a lower IIEF-EF (P<0.001). Patients with a CES-D of <16 had significantly higher EF recovery rates compared to those with depression (60.8 vs 49.2%; P=0.03). Patients receiving postoperative aRT had lower rates of EF compared with their counterparts left untreated after surgery (40.7 vs 59.8%; P<0.001). These results were confirmed in multivariable analyses, where preoperative IIEF-EF (P<0.001), depression (P=0.04) and aRT (P=0.03) were confirmed as significant predictors of EF recovery.
Conclusions:
Preoperative functional status and depression should be considered when counseling PCa patients regarding the long-term side effects of BNSRP. Moreover, the administration of aRT has a detrimental effect on the probability of recovering EF after BNSRP. This should be taken into account when balancing the potential benefits and side effects of multimodal therapies in PCa patients.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


References
Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T et al. EAU guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol 2014; 65: 124–137.
Resnick MJ, Koyama T, Fan KH, Albertsen PC, Goodman M, Hamilton AS et al. Long-term functional outcomes after treatment for localized prostate cancer. New Engl J Med 2013; 368: 436–445.
Salinas CA, Tsodikov A, Ishak-Howard M, Cooney KA . Prostate cancer in young men: an important clinical entity. Nat Rev Urol 2014; 11: 317–323.
Boorjian SA, Eastham JA, Graefen M, Guillonneau B, Karnes RJ, Moul JW et al. A critical analysis of the long-term impact of radical prostatectomy on cancer control and function outcomes. Eur Urol 2012; 61: 664–675.
Prabhu V, Lee T, McClintock TR, Lepor H . Short-, intermediate-, and long-term quality of life outcomes following radical prostatectomy for clinically localized prostate cancer. Rev Urol 2013; 15: 161–177.
Haglind E, Carlsson S, Stranne J, Wallerstedt A, Wilderang U, Thorsteinsdottir T et al. Urinary incontinence and erectile dysfunction after robotic versus open radical prostatectomy: a prospective, controlled, nonrandomised trial. Eur Urol 2015; 68: 216–225.
Ficarra V, Novara G, Ahlering TE, Costello A, Eastham JA, Graefen M et al. Systematic review and meta-analysis of studies reporting potency rates after robot-assisted radical prostatectomy. Eur Urol 2012; 62: 418–430.
Gandaglia G, Suardi N, Gallina A, Zaffuto E, Cucchiara V, Vizziello D et al. How to optimize patient selection for robot-assisted radical prostatectomy: functional outcome analyses from a tertiary referral center. J Endourol 2014; 28: 792–800.
Weyne E, Castiglione F, Van der Aa F, Bivalacqua TJ, Albersen M . Landmarks in erectile function recovery after radical prostatectomy. Nat Rev Urol 2015; 12: 289–297.
Walsh PC, Donker PJ . Impotence following radical prostatectomy: insight into etiology and prevention. J Urol 1982; 128: 492–497.
Montorsi F, Salonia A, Suardi N, Gallina A, Zanni G, Briganti A et al. Improving the preservation of the urethral sphincter and neurovascular bundles during open radical retropubic prostatectomy. Eur Urol 2005; 48: 938–945.
Montorsi F, Wilson TG, Rosen RC, Ahlering TE, Artibani W, Carroll PR et al. Best practices in robot-assisted radical prostatectomy: recommendations of the Pasadena Consensus Panel. Eur Urol 2012; 62: 368–381.
Radloff LS . The CES-D scale. A self-report depression scale for research in the general population. Appl Psychol Measur 1977; 1: 385–401.
Cappelleri JC, Rosen RC, Smith MD, Mishra A, Osterloh IH . Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999; 54: 346–351.
Gallina A, Bianchi M, Gandaglia G, Cucchiara V, Suardi N, Montorsi F et al. A detailed analysis of the association between postoperative phosphodiesterase type 5 inhibitor use and the risk of biochemical recurrence after radical prostatectomy. Eur Urol 2015; 68: 750–753.
Briganti A, Gallina A, Suardi N, Capitanio U, Tutolo M, Bianchi M et al. What is the definition of a satisfactory erectile function after bilateral nerve sparing radical prostatectomy? J Sex Med 2011; 8: 1210–1217.
Suardi N, Moschini M, Gallina A, Gandaglia G, Abdollah F, Capitanio U et al. Nerve-sparing approach during radical prostatectomy is strongly associated with the rate of postoperative urinary continence recovery. BJU Int 2013; 111: 717–722.
Gallina A, Ferrari M, Suardi N, Capitanio U, Abdollah F, Tutolo M et al. Erectile function outcome after bilateral nerve sparing radical prostatectomy: which patients may be left untreated? J Sex Med 2012; 9: 903–908.
Novara G, Ficarra V, D'Elia C, Secco S, De Gobbi A, Cavalleri S et al. Preoperative criteria to select patients for bilateral nerve-sparing robotic-assisted radical prostatectomy. J Sex Med 2010; 7: 839–845.
Shikanov S, Desai V, Razmaria A, Zagaja GP, Shalhav AL . Robotic radical prostatectomy for elderly patients: probability of achieving continence and potency 1 year after surgery. J Urol 2010; 183: 1803–1807.
Gandaglia G, Suardi N, Gallina A, Capitanio U, Abdollah F, Salonia A et al. Preoperative erectile function represents a significant predictor of postoperative urinary continence recovery in patients treated with bilateral nerve sparing radical prostatectomy. J Urol 2012; 187: 569–574.
Steineck G, Bjartell A, Hugosson J, Axen E, Carlsson S, Stranne J et al. Degree of preservation of the neurovascular bundles during radical prostatectomy and urinary continence 1 year after surgery. Eur Urol 2015; 67: 559–568.
Weber BA, Roberts BL, Mills TL, Chumbler NR, Algood CB . Physical and emotional predictors of depression after radical prostatectomy. Am J Mens Health 2008; 2: 165–171.
Perelman MA . Erectile dysfunction and depression: screening and treatment. Urol Clin North Am 2011; 38: 125–139.
Tan HM, Tong SF, Ho CC . Men's health: sexual dysfunction, physical, and psychological health—is there a link? J Sex Med 2012; 9: 663–671.
Kohler N, Friedrich M, Gansera L, Holze S, Thiel R, Roth S et al. Psychological distress and adjustment to disease in patients before and after radical prostatectomy. Results of a prospective multi-centre study. Eur J Cancer Care 2014; 23: 795–802.
Suardi N, Gallina A, Lista G, Gandaglia G, Abdollah F, Capitanio U et al. Impact of adjuvant radiation therapy on urinary continence recovery after radical prostatectomy. Eur Urol 2014; 65: 546–551.
Showalter TN, Hegarty SE, Rabinowitz C, Maio V, Hyslop T, Dicker AP et al. Assessing adverse events of postprostatectomy radiation therapy for prostate cancer: evaluation of outcomes in the Regione Emilia-Romagna, Italy. Int J Radiat Oncol Biol Phys 2015; 91: 752–759.
Formenti SC, Lieskovsky G, Skinner D, Tsao-Wei DD, Groshen S, Petrovich Z . Update on impact of moderate dose of adjuvant radiation on urinary continence and sexual potency in prostate cancer patients treated with nerve-sparing prostatectomy. Urology 2000; 56: 453–458.
Hegarty SE, Hyslop T, Dicker AP, Showalter TN . Radiation therapy after radical prostatectomy for prostate cancer: evaluation of complications and influence of radiation timing on outcomes in a large, population-based cohort. PLoS One 2015; 10: e0118430.
Thompson IM, Tangen CM, Paradelo J, Lucia MS, Miller G, Troyer D et al. Adjuvant radiotherapy for pathological T3N0M0 prostate cancer significantly reduces risk of metastases and improves survival: long-term followup of a randomized clinical trial. J Urol 2009; 181: 956–962.
Stember DS, Mulhall JP . The concept of erectile function preservation (penile rehabilitation) in the patient after brachytherapy for prostate cancer. Brachytherapy 2012; 11: 87–96.
Zelefsky MJ, Eid JF . Elucidating the etiology of erectile dysfunction after definitive therapy for prostatic cancer. Int J Radiat Oncol Biol Phys 1998; 40: 129–133.
Clavell-Hernandez J, Wang R . Penile rehabilitation following prostate cancer treatment: review of current literature. Asian J Androl 2015; 17: 916–922.
Gandaglia G, Gallina A, Suardi N, Abdollah F, Passoni N, Bianchi M et al. Preoperative erectile function is the only predictor of the use of a high number of phosphodiesterase type-5 inhibitors after bilateral nerve-sparing radical prostatectomy. Int J Impot Res 2014; 26: 201–204.
Thompson JE, Egger S, Bohm M, Haynes AM, Matthews J, Rasiah K et al. Superior quality of life and improved surgical margins are achievable with robotic radical prostatectomy after a long learning curve: a prospective single-surgeon study of 1552 consecutive cases. Eur Urol 2014; 65: 521–531.
Edwards B, Clarke V . The psychological impact of a cancer diagnosis on families: the influence of family functioning and patients' illness characteristics on depression and anxiety. Psychooncology 2004; 13: 562–576.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Gandaglia, G., Lista, G., Fossati, N. et al. Non-surgically related causes of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Prostate Cancer Prostatic Dis 19, 185–190 (2016). https://doi.org/10.1038/pcan.2016.1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pcan.2016.1
This article is cited by
-
Reply to 'Non-surgically related causes of erectile dysfunction after bilateral nerve-sparing radical prostatectomy'
Prostate Cancer and Prostatic Diseases (2017)
-
Surgical Techniques for Managing Post-prostatectomy Erectile Dysfunction
Current Urology Reports (2017)
