
Abstract
Many patients with multiple sclerosis (MS) experience clinical relapses or progression of disability, or exhibit evidence of disease activity on MRI, despite the use of disease-modifying therapy. Although evidence clearly supports the efficacy of interferon β (IFN-β) in treating MS, the factors that determine the response to this drug in individual patients have not been fully elucidated. As more treatment options become available, the early identification of factors that can affect or predict the efficacy of agents in individual patients is important, because such knowledge facilitates early switching of treatment. Despite years of research and numerous reports of promising therapy markers for MS, few markers have emerged as clinically useful. Several studies suggest, however, that development of MRI lesions within 6–24 months after the initiation of IFN-β treatment predicts an unfavorable response. In addition, persistently high titers of neutralizing antibodies diminish or abrogate the therapeutic effects of IFN-β, and help to identify patients who do not respond. This Review highlights advances in research on the response to IFN-β in patients with MS and aims to provide a practical approach for incorporating clinical data, biological markers and MRI measures of disease activity into their therapeutic management.
Key Points
-
The mean reduction in the multiple sclerosis (MS) relapse rate associated with interferon (IFN)-β treatment is ≈30%
-
The response to IFN-β treatment in patients with MS is highly heterogeneous
-
Defining treatment response is difficult in individual patients with relapsing–remitting MS
-
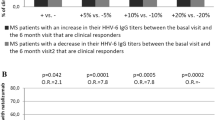
Active MRI lesions after the first 6 months of IFN-β treatment predict clinical disease activity
-
In patients with persistently high titers of neutralizing antibodies to IFN-β and/or lack of IFN-β biological activity, therapy should be switched
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others
References
Comi, G. et al. Effect of glatiramer acetate on conversion to clinically definite multiple sclerosis in patients with clinically isolated syndrome (PreCISe study): a randomised, double-blind, placebo-controlled trial. Lancet 374, 1503–1511 (2009).
Filippi, M. et al. Interferon-β1a for brain tissue loss in patients at presentation with syndromes suggestive of multiple sclerosis: a randomised, double-blind, placebo-controlled trial. Lancet 364, 1489–1496 (2004).
Jacobs, L. D. et al. Intramuscular interferon-β1a therapy initiated during a first demyelinating event in multiple sclerosis. CHAMPS Study Group. N. Engl. J. Med. 343, 898–904 (2000).
Kappos, L. et al. Effect of early versus delayed interferon-β1b treatment on disability after a first clinical event suggestive of multiple sclerosis: a 3-year follow-up analysis of the BENEFIT study. Lancet 370, 389–397 (2007).
The IFN-β Multiple Sclerosis Study Group and The University of British Columbia MS/MRI Analysis Group. Interferon-β1b in the treatment of multiple sclerosis: final outcome of the randomized controlled trial. Neurology 45, 1277–1285 (1995).
PRISMS (Prevention of Relapses and Disability by Interferon-β1a Subcutaneously in Multiple Sclerosis) Study Group. Randomised double-blind placebo-controlled study of interferon-β1a in relapsing/remitting multiple sclerosis. Lancet 352, 1498–1504 (1998).
Jacobs, L. D. et al. Intramuscular interferon-β1a for disease progression in relapsing multiple sclerosis. The Multiple Sclerosis Collaborative Research Group (MSCRG). Ann. Neurol. 39, 285–294 (1996).
Johnson, K. P. et al. Copolymer 1 reduces relapse rate and improves disability in relapsing–remitting multiple sclerosis: results of a phase III multicenter, double-blind placebo-controlled trial. The Copolymer 1 Multiple Sclerosis Study Group. Neurology 45, 1268–1276 (1995).
Giacomini, P. S., Arnold, D. L., Bar-Or, A. & Antel, J. P. Defining multiple sclerosis treatment response with magnetic resonance imaging: how much activity is too much? Arch. Neurol. 66, 19–20 (2009).
Rio, J., Comabella, M. & Montalban, X. Predicting responders to therapies for multiple sclerosis. Nat. Rev. Neurol. 5, 553–560 (2009).
Polman, C. H. et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N. Engl. J. Med. 354, 899–910 (2006).
Rudick, R. A. et al. Natalizumab plus interferon-β1a for relapsing multiple sclerosis. N. Engl. J. Med. 354, 911–923 (2006).
Giovannoni, G. et al. A placebo-controlled trial of oral cladribine for relapsing multiple sclerosis. N. Engl. J. Med. 362, 416–426 (2010).
Cohen, J. A. et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N. Engl. J. Med. 362, 402–415 (2010).
Kappos, L. et al. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N. Engl. J. Med. 362, 387–401 (2010).
Coles, A. The fragile benefit of BENEFIT. Lancet Neurol. 6, 753–754 (2007).
Goodin, D. S. & Bates, D. Treatment of early multiple sclerosis: the value of treatment initiation after a first clinical episode. Mult. Scler. 15, 1175–1182 (2009).
Comi, G. Shifting the paradigm toward earlier treatment of multiple sclerosis with interferon-β. Clin. Ther. 31, 1142–1157 (2009).
Sormani, M. P. et al. Magnetic resonance imaging as a potential surrogate for relapses in multiple sclerosis: a meta-analytic approach. Ann. Neurol. 65, 268–275 (2009).
Sormani, M. P. et al. The distribution of magnetic resonance imaging response to interferon-β1b in multiple sclerosis. J. Neurol. 252, 1455–1458 (2005).
Chiu, A. W. et al. Heterogeneity in response to interferon-β in patients with multiple sclerosis: a 3-year monthly imaging study. Arch. Neurol. 66, 39–43 (2009).
Rudick, R. A., Lee, J. C., Simon, J., Ransohoff, R. M. & Fisher, E. Defining interferon β response status in multiple sclerosis patients. Ann. Neurol. 56, 548–555 (2004).
Pozzilli, C. et al. Post-marketing survey on clinical response to interferon-β in relapsing multiple sclerosis: the Roman experience. Neurol. Sci. 26 (Suppl. 4), S174–S178 (2005).
Tomassini, V. et al. Predictors of long-term clinical response to interferon-β therapy in relapsing multiple sclerosis. J. Neurol. 253, 287–293 (2006).
Rio, J. et al. Relationship between MRI lesion activity and response to IFN-β in relapsing–remitting multiple sclerosis patients. Mult. Scler. 14, 479–484 (2008).
Rio, J. et al. Measures in the first year of therapy predict the response to interferon-β in MS. Mult. Scler. 15, 848–853 (2009).
Prosperini, L., Gallo, V., Petsas, N., Borriello, G. & Pozzilli, C. One-year MRI scan predicts clinical response to interferon β in multiple sclerosis. Eur. J. Neurol. 16, 1202–1209 (2009).
Polman, C. H. et al. Recommendations for clinical use of data on neutralising antibodies to interferon-β therapy in multiple sclerosis. Lancet Neurol. 9, 740–750 (2010).
[No authors listed] Neutralizing antibodies during treatment of multiple sclerosis with interferon-β1b: experience during the first three years. The IFN-β Multiple Sclerosis Study Group and the University of British Columbia MS/MRI Analysis Group. Neurology 47, 889–894 (1996).
Francis, G. S., Rice, G. P. & Alsop, J. C. PRISM Study Group. Interferon-β1a in MS: results following development of neutralizing antibodies in PRISMS. Neurology 65, 48–55 (2005).
Freedman, M. S. et al. Impact of neutralizing antibodies within 5 years of treatment with interferon β1b initiated at the first event suggestive of multiple sclerosis. Neurology 72 (Suppl. 3), A197–A198 (2009).
Goodin, D. S. et al. Neutralizing antibodies during treatment with interferon β1b in 1745 patients with relapsing–remitting multiple sclerosis. Neurology 72 (Suppl. 3), A317–A318 (2010).
Kappos, L. et al. Neutralizing antibodies and efficacy of interferon β1a: a 4-year controlled study. Neurology 65, 40–47 (2005).
Durelli, L. et al. MRI activity and neutralising antibody as predictors of response to interferon-β treatment in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 79, 646–651 (2008).
van der Voort, L. et al. Clinical effect of neutralizing antibodies to interferon β that persist long after cessation of therapy for multiple sclerosis. Arch. Neurol. 67, 402–407 (2010).
Bertolotto, A. et al. Evaluation of bioavailability of three types of IFN-β in multiple sclerosis patients by a new quantitative-competitive-PCR method for MxA quantification. J. Immunol. Methods 256, 141–152 (2001).
Pachner, A. R., Dail, D., Pak, E. & Narayan, K. The importance of measuring IFN-β bioactivity: monitoring in MS patients and the effect of anti-IFN-β antibodies. J. Neuroimmunol. 166, 180–188 (2005).
van der Voort, L. et al. Interferon-β bioactivity measurement in multiple sclerosis: feasibility for routine clinical practice. Mult. Scler. 15, 212–218 (2009).
Bertolotto, A. et al. Persistent neutralizing antibodies abolish the interferon-β bioavailability in MS patients. Neurology 60, 634–639 (2003).
Deisenhammer, F. et al. Bioavailability of interferon β1b in MS patients with and without neutralizing antibodies. Neurology 52, 1239–1243 (1999).
Sominanda, A., Hillert, J. & Fogdell-Hahn, A. In vivo bioactivity of interferon-β in multiple sclerosis patients with neutralising antibodies is titre-dependent. J. Neurol. Neurosurg. Psychiatry 79, 57–62 (2008).
Sorensen, P. S. et al. Neutralizing antibodies hamper IFN-β bioactivity and treatment effect on MRI in patients with MS. Neurology 67, 1681–1683 (2006).
Malucchi, S. et al. Predictive markers for response to interferon therapy in patients with multiple sclerosis. Neurology 70, 1119–1127 (2008).
van der Voort, L. F. et al. Lack of interferon-β bioactivity is associated with the occurrence of relapses in multiple sclerosis. Eur. J. Neurol. 9, 1049–1052 (2009).
Hesse, D., Sellebjerg, F. & Sorensen, P. S. Absence of MxA induction by interferon β in patients with MS reflects complete loss of bioactivity. Neurology 73, 372–377 (2009).
van der Voort. et al. Spontaneous MxA mRNA level predicts relapses in patients with recently diagnosed MS. Neurology 75, 1228–1233 (2010).
Pappas, D. J. & Oksenberg, J. R. Multiple sclerosis pharmacogenomics: maximizing efficacy of therapy. Neurology 74 (Suppl. 1), S62–S69 (2010).
Rudick, R. A. & Polman, C. H. Current approaches to the identification and management of breakthrough disease in patients with multiple sclerosis. Lancet Neurol. 8, 545–559 (2009).
Vosslamber S., van Baarsen, L. G. & Verweij, C. L. Pharmacogenomics of IFN-β in multiple sclerosis: towards a personalized medicine approach. Pharmacogenomics 10, 97–108 (2009).
Cunningham, S. et al. Pharmacogenomics of responsiveness to interferon IFN-β treatment in multiple sclerosis: a genetic screen of 100 type I interferon-inducible genes. Clin. Pharmacol. Ther. 78, 635–646 (2005).
Leyva, L. et al. IFNAR1 and IFNAR2 polymorphisms confer susceptibility to multiple sclerosis but not to interferon-β treatment response. J. Neuroimmunol. 163, 165–171 (2005).
Sriram, U. et al. Pharmacogenomic analysis of interferon receptor polymorphisms in multiple sclerosis. Genes Immun. 4, 147–152 (2003).
Byun, E. et al. Genome-wide pharmacogenomic analysis of the response to interferon-β therapy in multiple sclerosis. Arch. Neurol. 65, 337–344 (2008).
Cénit, M. D. et al. Glypican 5 is an interferon-β response gene: a replication study. Mult. Scler. 15, 913–917 (2009).
Comabella, M. et al. Genome-wide scan of 500,000 single-nucleotide polymorphisms among responders and nonresponders to interferon-β therapy in multiple sclerosis. Arch. Neurol. 66, 972–978 (2009).
Sturzebecher, S. et al. Expression profiling identifies responder and non-responder phenotypes to interferon-β in multiple sclerosis. Brain 126, 1419–1429 (2003).
Weinstock-Guttman, B. et al. Genomic effects of once-weekly, intramuscular interferon-β1a treatment after the first dose and on chronic dosing: relationships to 5-year clinical outcomes in multiple sclerosis patients. J. Neuroimmunol. 205, 113–125 (2008).
van Baarsen, L. G. et al. Pharmacogenomics of interferon-β therapy in multiple sclerosis: baseline IFN signature determines pharmacological differences between patients. PLoS One 3, e1927 (2008).
Hesse, D. et al. Breakthrough disease during interferon-β therapy in MS: no signs of impaired biologic response. Neurology 74, 1455–1462 (2010).
Comabella, M. et al. A type I interferon signature in monocytes is associated with poor response to interferon-β in multiple sclerosis. Brain 132, 3353–3365 (2009).
Axtell, R. C. et al. T helper type 1 and 17 cells determine efficacy of interferon-β in multiple sclerosis and experimental encephalomyelitis. Nat. Med. 16, 406–412 (2010).
Filippi, M. & Agosta, F. Imaging biomarkers in multiple sclerosis. J. Magn. Reson. Imaging 31, 770–788 (2010).
Vandenbroeck, K., Urcelay, E. & Comabella, M. IFN-β pharmacogenomics in multiple sclerosis. Pharmacogenomics 11, 1137–1148 (2010).
Frank, J. A. et al. Interferon-β1b slows progression of atrophy in RRMS: three-year follow-up in NAb− and NAb+ patients. Neurology 62, 719–725 (2004).
Perini, P., Calabrese, M., Biasi, G. & Gallo, P. The clinical impact of interferon-β antibodies in relapsing–remitting MS. J. Neurol. 251, 305–309 (2004).
Malucchi, S. et al. Neutralizing antibodies reduce the efficacy of β IFN during treatment of multiple sclerosis. Neurology 62, 2031–2037 (2004).
Sorensen, P. S. et al. Clinical importance of neutralising antibodies against interferon-β in patients with relapsing–remitting multiple sclerosis. Lancet 362, 1184–1191 (2003).
Boz, C., Oger, J., Gibbs, E. & Grossberg, S. E. Reduced effectiveness of long-term interferon-β treatment on relapses in neutralizing antibody-positive multiple sclerosis patients: a Canadian multiple sclerosis clinic-based study. Mult. Scler. 13, 1127–1137 (2007).
Gilli, F. et al. Neutralizing antibodies against IFN-β in multiple sclerosis: antagonization of IFN-β mediated suppression of MMPs. Brain 127, 259–268 (2004).
Pachner, A. R., Narayan, K. & Pak, E. Multiplex analysis of expression of three IFN-β-induced genes in antibody-positive MS patients. Neurology 66, 444–446 (2006).
Gilli, F. Biological markers of interferon-β therapy: comparison among interferon-stimulated genes MxA, TRAIL and XAF-1. Mult. Scler. 12, 47–57 (2006).
Santos, R. et al. Dynamics of interferon-β modulated mRNA biomarkers in multiple sclerosis patients with anti-interferon-β neutralizing antibodies. J. Neuroimmunol. 176, 125–133 (2006).
Scagnolari, C. et al. Pharmacodynamics of interferon-β in multiple sclerosis patients with or without serum neutralizing antibodies. J. Neurol. 254, 597–604 (2007).
Hoffmann, L. A. Multiple sclerosis: relating MxA transcription to anti-interferon-β-neutralizing antibodies. Neurology 68, 958–959 (2007).
Capra, R. et al. IFNβ bioavailability in multiple sclerosis patients: MxA versus antibody-detecting assays. J. Neuroimmunol. 189, 102–110 (2007).
Aarskog, N. K., Marøy, T., Myhr, K. M. & Vedeler, C. A. Antibodies against interferon-β in multiple sclerosis. J. Neuroimmunol. 212, 148–150 (2009).
Pachner, A. R., Warth, J. D., Pace, A. & Goelz, S. Effect of neutralizing antibodies on biomarker responses to interferon-β: the INSIGHT study. Neurology 73, 1493–1500 (2009).
Zanotti, C. et al. Transfer of myxovirus-protein-A mRNA assay for interferon-β bioactivity measurement in multiple sclerosis patients to routine laboratory practice. A 4-year experience. Clin. Chem. Lab. Med. 48, 1235–1238 (2010).
Author information
Authors and Affiliations
Contributions
Both authors contributed equally to researching data for the article, made substantial contributions to the discussions of the content, and contributed equally to writing the article and to reviewing and/or editing of the manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
J. Killestein has received consulting fees from Merck-Serono and Novartis, and research support from Bayer Schering Pharma, Biogen-Idec, GlaxoSmithKline, Merck Serono, Novartis and Teva.
C. H. Polman has accepted consulting fees or honoraria from Actelion, Antisense Therapeutics, Bayer Schering, Biogen Idec, GlaxoSmithKline, Merck-Serono, Novartis, Roche, Teva and UCB. He has received grant support from Bayer Schering, Biogen Idec, GlaxoSmithKline, Merck-Serono, Novartis, Teva and UCB.
Rights and permissions
About this article
Cite this article
Killestein, J., Polman, C. Determinants of interferon β efficacy in patients with multiple sclerosis. Nat Rev Neurol 7, 221–228 (2011). https://doi.org/10.1038/nrneurol.2011.22
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrneurol.2011.22
This article is cited by
-
miR-145 and miR20a-5p Potentially Mediate Pleiotropic Effects of Interferon-Beta Through Mitogen-Activated Protein Kinase Signaling Pathway in Multiple Sclerosis Patients
Journal of Molecular Neuroscience (2017)
-
Consider switching to another disease-modifying therapy when unacceptable disease activity occurs in relapsing multiple sclerosis
Drugs & Therapy Perspectives (2014)
-
Defining and scoring response to IFN-β in multiple sclerosis
Nature Reviews Neurology (2013)
-
Interferon-beta therapy in multiple sclerosis: the short-term and long-term effects on the patients’ individual gene expression in peripheral blood
Molecular Neurobiology (2013)
-
Switching Therapies in Multiple Sclerosis
CNS Drugs (2013)
