
Abstract
Therapies for relapsing–remitting multiple sclerosis (RRMS) are only partially effective, and, in most patients receiving such treatment, clinical activity persists. Accurately assessing the treatment response to disease-modifying agents enables non-responder patients to be identified at an early stage into therapy. Patients can then be switched to another, potentially more effective, therapy before too much neurological damage has occurred. Several criteria based on relapses, disability progression or both have been proposed for clinical evaluation of the treatment response to disease-modifying agents. These criteria have not been independently validated, however, and no consensus over which are the best to use currently exists among investigators. MRI can also be employed to detect disease activity in patients treated with disease-modifying agents. Changes on MRI can provide subclinical data relating to disease activity that can be of great benefit in patients monitoring, as inflammatory events occur more often than clinical events. Pharmacogenomic approaches are in the early stages of development for MS, but hold great promise for the eventual development of individually tailored therapies. In this Review, we discuss the proposed approaches for monitoring and predicting treatment responses to disease-modifying agents in patients with RRMS. We evaluate the roles of clinical measures, MRI and pharmacogenomics in these processes.
Key Points
-
Relapses and progression of disability are the clinical features of relapsing–remitting multiple sclerosis (RRMS) that are monitored when determining a patient's clinical response to treatment
-
The proportion of non-responders varies depending on the definition of treatment response used
-
Criteria based on relapse measures have poor sensitivity and poor positive predictive value for assessing treatment response
-
Accumulation of new lesions on serial MRI might be a good marker of a poor response to treatment
-
Combining clinical measures of disease activity (relapses and/or progression of disability) with MRI assessment might improve our ability to identify patients who respond poorly to treatment
-
Pharmacogenomics holds great promise for developing individually tailored therapies for patients with RRMS
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
[No authors listed] Interferon β1b is effective in relapsing–remitting multiple sclerosis. I. Clinical results of a multicenter, randomized, double-blind, placebo-controlled trial. The IFNB Multiple Sclerosis Study Group. Neurology 43, 655–661 (1993).
Jacobs, L. D. et al. Intramuscular interferon β1a for disease progression in relapsing multiple sclerosis. The Multiple Sclerosis Collaborative Research Group (MSCRG). Ann. Neurol. 39, 285–294 (1996).
[No authors listed] Randomised double-blind placebo-controlled study of interferon β1a in relapsing/remitting multiple sclerosis. PRISMS (Prevention of Relapses and Disability by Interferon β1a Subcutaneously in Multiple Sclerosis) Study Group. Lancet 352, 1498–1504 (1998).
Johnson, K. P. et al. Copolymer 1 reduces relapse rate and improves disability in relapsing-remitting multiple sclerosis: results of a phase III multicenter, double-blind placebo-controlled trial. The Copolymer 1 Multiple Sclerosis Study Group. Neurology 45, 1268–1276 (1995).
Polman, C. H. et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N. Eng. J. Med. 354, 899–910 (2006).
Paty, D. W. & Li, D. K. Interferon β1b is effective in relapsing-remitting multiple sclerosis. II. MRI analysis results of a multicenter, randomized, double-blind, placebo-controlled trial. UBC MS/MRI Study Group and the IFNB Multiple Sclerosis Study Group. Neurology 43, 662–667 (1993).
Simon, J. H. et al. Magnetic resonance studies of intramuscular interferon β1a for relapsing multiple sclerosis. The Multiple Sclerosis Collaborative Research Group. Ann. Neurol. 43, 79–87 (1998).
Li, D. K. & Paty, D. W. Magnetic resonance imaging results of the PRISMS trial: a randomized, double-blind, placebo-controlled study of interferon β1a in relapsing-remitting multiple sclerosis. Ann. Neurol. 46, 197–206 (1999).
Río, J. et al. Assessment of different treatment failure criteria in a cohort of relapsing-remitting multiple sclerosis patients treated with interferon β: implications for clinical trials. Ann. Neurol. 52, 400–406 (2002).
Río, J. et al. Defining the response to interferon β in relapsing–remitting multiple sclerosis patients. Ann. Neurol. 59, 344–352 (2006).
Baranzini, S. E. et al. Transcription-based prediction of response to IFN-β using supervised computational methods. PloS Biol. 3, e2 (2005).
Panitch, H. et al. Randomized, comparative study of interferon β1a treatment regimens in MS: The EVIDENCE Trial. Neurology 59, 1496–1506 (2002).
Durelli, L. et al. Every-other-day interferon β1b versus once-weekly interferon 1a for multiple sclerosis: Results of a 2-year prospective randomised multicentre study (INCOMIN). Lancet 359, 1453–1460 (2002).
Troyano, M. et al. Interferon β in relapsing–remitting multiple sclerosis: an independent postmarketing study in southern Italy. Mult. Scler. 9, 451–457 (2003).
Waubant, E. et al. Clinical characteristics of responders to interferon therapy for relapsing MS. Neurology 61, 184–189 (2003).
Río, J. et al. Interferon β in RRMS. An eight years experience in a specialist multiple sclerosis centre. J. Neurol. 252, 795–800 (2005).
Wiendl, H. et al. Basic and escalating immunomodulatory treatments in multiple sclerosis: current therapeutic recommendations. J. Neurol. 255, 1449–1463 (2008).
Río, J. et al. Factors related with treatment adherence to interferon β and glatiramer acetate therapy in multiple sclerosis. Mult. Scler. 11, 306–309 (2005).
Goodin, D. S. et al. Disease modifying therapies in multiple sclerosis: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology 58, 169–178 (2002)
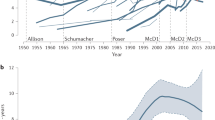
Schumacher, G. A. et al. Problems of experimental trials of therapies in multiple sclerosis: report by the panel on the evaluation of experimental trials of therapies in multiple sclerosis. Ann. NY Acad. Sci. 122, 552–568 (1965).
Weinshenker, B. G. et al. The natural history of multiple sclerosis: a geographically based study. 2. Predictive value of the early clinical course. Brain 112, 1419–1428 (1989).
Confavreux, C., Vucosic, S. & Adeleine, P. Early clinical predictors and progression of irreversible disability in multiple sclerosis: an amnesic process. Brain 126, 770–782 (2003).
Kantarci, O. et al. Survival and predictors of disability in Turkish MS patients. Turkish Multiple Sclerosis Study Group (TMSSG). Neurology 51, 765–772 (1998).
Eriksson, M., Andersen, O. & Runmarker, B. Long-term follow-up of patients with clinically isolated syndromes, relapsing–remitting and secondary progressive multiple sclerosis. Mult. Scler. 9, 260–274 (2003).
Runmarker, B. & Andersen, O. Prognostic factors in a multiple sclerosis cohort with twenty-five years follow-up. Brain 116, 117–134 (1993).
Amato, M. P. & Ponziani, G. A prospective study on the prognosis of multiple sclerosis. Neurol. Sci. 21 (4 Suppl. 2), S831–S838 (2000).
Miller, D. H., Hornabrook, P. W. & Purdie, G. The natural history of multiple sclerosis: a regional study with some longitudinal data. J. Neurol. Neurosurg. Psychiatry 55, 341–346 (1992).
O'Rourke, K., Walsh, C., Antonelli, G. & Hutchinson, M. Predicting β-interferon failure in relapsing-remitting multiple sclerosis. Mult. Scler. 13, 336–342 (2007).
Martínez-Yélamos, S. et al. Regression to the mean in multiple sclerosis. Mult. Scler. 12, 826–829 (2006).
Fog, T. & Linnemann, F. The course of multiple sclerosis in 73 cases with computer-designed curves. Acta Neurol. Scand. 47, 9–11 (1970).
Lhermitte, F., Marteau, R., Gazengel, J., Dordain, G. & Deloche, G. The frequency of relapse in multiple sclerosis: a study based on 245 cases. J. Neurol. 205, 47–59 (1973).
Patzold, U. & Pocklington, P. R. Course of multiple sclerosis: first results of a prospective study carried out of 102 MS patients from 1976–1980. Acta Neurol. Scand. 65, 248–266 (1982).
Thygesen, P. Prognosis in initial stage of disseminated primary demyelinating disease of central nervous system. Arch. Neurol. Psychiatry 61, 339–351 (1949).
Miller, D. H. Guidelines for MRI monitoring of the treatment of multiple sclerosis: recommendations of the US Multiple Sclerosis Society's task force. Mult. Scler. 1, 335–338 (1996).
Noseworthy, J. H., Vandervoort, M. K., Wong, C. J. & Ebers, G. C. Interrater variability with the Expanded Disability Status Scale (EDSS) and Functional Systems (FS) in a multiple sclerosis clinical trial. The Canadian Cooperation MS Study Group. Neurology 40, 971–975 (1990).
Albrecht, H. et al. Day-to-day variability of maximum walking distance in MS patients can mislead to relevant changes in the Expanded Disability Status Scale (EDSS): average walking speed is a more constant parameter. Mult. Scler. 7, 105–109 (2001).
Liu, C. & Blumhardt, L. D. Disability outcome measures in therapeutic trials of relapsing-remitting multiple sclerosis: effects of heterogeneity of disease course in placebo cohorts. J. Neurol. Neurosurg. Psychiatry 68, 450–457 (2000).
Fusco, C. et al. HLA-DRB1*1501 and response to copolymer-1 therapy in relapsing–remitting multiple sclerosis. Neurology 57, 1976–1979 (2001).
Kappos, L. et al. Final analysis of the European multicenter trial on IFN β-1b in secondary progressive MS. Neurology 57, 1969–1975 (2001).
Kracke, A. et al. Mx proteins in blood leukocytes for monitoring interferon β-1b therapy in patients with MS. Neurology 54, 193–199 (2000).
Stürzebecher, S. et al. Expression profiling identifies responder and non-responder phenotypes to interferon β in multiple sclerosis. Brain 126, 1419–1429 (2003).
Villoslada, P., Oksenberg, J. R., Río, J. & Montalban, X. Clinical characteristics of responders to interferon therapy for relapsing MS. Neurology 62, 1653 (2004).
Wandinger, K. P. et al. TNF-related apoptosis inducing ligand (TRAIL) as a potential response marker for interferon β treatment in multiple sclerosis. Lancet 361, 2036–2043 (2003).
Waubant, E. et al. Clinical characteristics of responders to interferon therapy for relapsing MS. Neurology 61, 184–189 (2003).
Petzold, A. et al. Treatment response in relation to inflammatory and axonal surrogate marker in multiple sclerosis. Mult. Scler. 10, 281–283 (2004).
Rudick, R., Lee, J., Simon, J., Ransohoff, R. M. & Fisher, E. Defining interferon β response status in multiple sclerosis patients. Ann. Neurol. 56, 548–555 (2004).
Portaccio, E., Zipoli, V., Siracusa, G., Sorbi, S. & Amato, M. P. Response to interferon β therapy in relapsing–remitting multiple sclerosis: a comparison of different clinical criteria. Mult. Scler. 12, 281–286 (2006).
Freedman, M. S. & Forrestal, F. G. Canadian treatment optimization recommendations (TOR) as a predictor of disease breakthrough in patients with multiple sclerosis treated with interferon β1a: analysis of the PRIMS study. Mult. Scler. 14, 1234–1241 (2008).
Barkhof, F. et al. Comparison of MRI criteria at first presentation to predict conversion to clinically definite multiple sclerosis. Brain 120, 2059–2069 (1997).
Tintoré, M. et al. Isolated demyelinating syndromes: comparison of different MR imaging criteria to predict conversion to clinically definite multiple sclerosis. AJNR 21, 702–706 (2000).
Chiu, A. W. et al. Heterogeneity in response to interferon β in patients with multiple sclerosis. Arch. Neurol. 66, 39–43 (2009).
Sormani, M. P. et al. Magnetic resonance imaging as a potential surrogate for relapses in multiple sclerosis: a meta-analytic approach. Ann. Neurol. 65, 268–275 (2009).
Río, J. et al. Relationship between MRI lesion activity and response to IFN-β in relapsing–remitting multiple sclerosis patients. Mult. Scler. 14, 479–484 (2008).
Freedman, M. S. et al. Treatment optimization in multiple sclerosis. Can. J. Neurol. Sci. 31, 157–168 (2004).
Sormani, M. P., Rovaris, M., Comi, G. & Filippi, M. A composite score to predict short-term disease activity in patients with relapsing–remitting MS. Neurology 69, 1230–1235 (2007).
Río, J. et al. Clinical and magnetic resonance imaging measures in the assessment of the response to interferon β. Mult. Scler. 15, 848–853 (2009).
Wolf, C. R., Smith, G. & Smith, R. L. Science, medicine, and the future: pharmacogenetics. BMJ 320, 987–990 (2000).
Comabella, M. & Martin, R. Genomics in multiple sclerosis—current state and future directions. J. Neuroimmunol. 187, 1–8 (2007).
Singh, M. K. et al. Gene expression changes in peripheral blood mononuclear cells from multiple sclerosis patients undergoing β-interferon therapy. J. Neurol. Sci. 258, 52–59 (2007).
van Baarsen, L. G. et al. Pharmacogenomics of interferon β therapy in multiple sclerosis: baseline IFN signature determines pharmacological differences between patients. PLoS One 3, e1927 (2008).
Villoslada, P. et al. The HLA locus and multiple sclerosis in Spain. Role in disease susceptibility, clinical course and response to interferon β. J. Neuroimmunol. 130, 194–201 (2002).
Sriram, U. et al. Pharmacogenomic analysis of interferon receptor polymorphisms in multiple sclerosis. Genes Immun. 4, 147–152 (2003).
Fernández, O. et al. HLA class II and response to interferon β in multiple sclerosis. Acta Neurol. Scand. 112, 391–394 (2005).
Cunningham, S. et al. Pharmacogenomics of responsiveness to interferon IFN-β treatment in multiple sclerosis: a genetic screen of 100 type I interferon-inducible genes. Clin. Pharmacol. Ther. 78, 635–646 (2005).
Leyva, L. et al. IFNAR1 and IFNAR2 polymorphisms confer susceptibility to multiple sclerosis but not to interferon β treatment response. J. Neuroimmunol. 163, 165–171 (2005).
Martínez, A. et al. An IFNG polymorphism is associated with interferon β response in Spanish MS patients. J. Neuroimmunol. 173, 196–199 (2006).
Weinstock-Guttman, B., Tamaño-Blanco, M., Bhasi, K., Zivadinov, R. & Ramanathan, M. Pharmacogenetics of MXA SNPs in interferon β treated multiple sclerosis patients. J. Neuroimmunol. 182, 236–239 (2007).
Comabella, M. et al. HLA class I and II alleles and response to treatment with interferon β in relapsing–remitting multiple sclerosis. J. Neuroimmunol. 210, 116–119 (2009).
Grossman, I. et al. Pharmacogenetics of glatiramer acetate therapy for multiple sclerosis reveals drug-response markers. Pharmacogenet. Genomics 17, 657–666 (2007).
Lucchinetti, C. et al. Heterogeneity of multiple sclerosis lesions: implications for the pathogenesis of demyelination. Ann. Neurol. 47, 707–717 (2000).
Hartung, H. P. et al. Neutralising antibodies to interferon β in multiple sclerosis: expert panel report. J. Neurol. 254, 827–837 (2007).
Byun, E. et al. Genome-wide pharmacogenomic analysis of the response to interferon β therapy in multiple sclerosis. Arch. Neurol. 65, 337–344 (2008).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
X. Montalban has acted as a consultant and on the speaker's bureau for Almirall, Bayer Schering Pharma, Biogen Idec, Merck Serono, Novartis, Sanofi-aventis, Teva and UCB Pharma. He has also received research support from these companies. J. Río and M. Comabella have received honoraria for speaking from Bayer Schering Pharma, Biogen Idec, Merck Serono, Novartis, Sanofi-aventis and Teva.
Rights and permissions
About this article
Cite this article
Río, J., Comabella, M. & Montalban, X. Predicting responders to therapies for multiple sclerosis. Nat Rev Neurol 5, 553–560 (2009). https://doi.org/10.1038/nrneurol.2009.139
Issue Date:
DOI: https://doi.org/10.1038/nrneurol.2009.139
This article is cited by
-
Peripheral myeloid-derived suppressor cells are good biomarkers of the efficacy of fingolimod in multiple sclerosis
Journal of Neuroinflammation (2022)
-
Treatment response scoring systems to assess long-term prognosis in self-injectable DMTs relapsing–remitting multiple sclerosis patients
Journal of Neurology (2022)
-
Chronic inflammation in multiple sclerosis — seeing what was always there
Nature Reviews Neurology (2019)
-
Predictive value of early magnetic resonance imaging measures is differentially affected by the dose of interferon beta-1a given subcutaneously three times a week: an exploratory analysis of the PRISMS study
BMC Neurology (2018)
-
Assessing treatment outcomes in multiple sclerosis trials and in the clinical setting
Nature Reviews Neurology (2018)
