
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) is a costly long-term condition associated with frequent Accident and Emergency (A&E) and hospital admissions. Psychological difficulties and inadequate self-management can amplify this picture.
Aims:
To compare a cognitive-behavioural manual versus information booklets (IB) on health service use, mood and health status.
Methods:
Two hundred and twenty-two COPD patients were randomly allocated to receive either the COPD breathlessness manual (CM) or IB. They were instructed to work through their programme at home, over 5 weeks. Guidance from a facilitator was provided at an initial home visit plus two telephone call follow-ups.
Results:
After 12 months, total A&E visits had reduced by 42% in the CM group, compared with a 16% rise in the IB group. The odds of people in the IB group attending A&E 12 months post-intervention was 1.9 times higher than for the CM group (CI 1.05–3.53). Reduction in hospital admissions and bed days were greatest in the CM group. At 6 months, there were significantly greater improvements in anxiety (F (2,198)=5.612, P=0.004), depression (F (1.8,176.1)=10.697, P⩽0.001) and dyspnoea (F (2,198)=18.170, P⩽0.001) in the CM group. Estimated savings at 12 months were greatest in the CM group, amounting to £30k or £270 per participant.
Conclusion:
The COPD manual, which addresses physical and mental health, is a straightforward cost-effective intervention that is worth offering to COPD patients within primary or secondary care.
Similar content being viewed by others

Introduction
Living with Chronic Obstructive Pulmonary Disease (COPD) presents significant ongoing physical, psychological, emotional and lifestyle challenges for individuals, families and carers. It is a costly condition to the UK National Health Service (NHS). Mental health problems are estimated to exist in 30% of all people with a long-term condition.1 This figure is higher in COPD (34–60%) for problems such as anxiety, panic and depression2–5 and prevalence of panic disorder is up to 10 times higher in COPD compared with the general population.6 Psychological comorbidity is associated with persistent smoking, greater Accident and Emergency (A&E) visits, hospital admissions and readmissions, longer stays and increased NHS spending.7–12 Furthermore, individuals suffer worse quality of life, functioning and disease outcomes, which is unrelated to level of disease severity.4,13–15
Breathlessness can be distressing and difficult to understand and control.16 It is a defining feature of both COPD and panic attacks and can develop through a complex interaction between physical, psychological, emotional and behavioural factors. The cognitive-behavioural model17 explains panic via a vicious cycle of catastrophic appraisals of breathlessness, escalating fear and heightened sympathetic arousal. This pattern may be emphasised further through the reactions of observers, who may feel equally frightened and helpless. The culmination can often be an overreliance on medications, over-monitoring of symptoms and inappropriate presentation at emergency services. Individuals may start to mistakenly avoid activities due to fearful beliefs about the consequences of becoming breathless,18 leading to isolation, depression, continued smoking and a lack of motivation and energy for self-management.6 This could have a knock-on effect on participation in pulmonary rehabilitation (PR), despite the demonstrated benefits of these programmes on dyspnoea, fatigue and control over the disease.19 Patients often value group support; however, in reality, encouraging attendance and adherence to PR/breathlessness groups can be an issue.20,21
There is promising evidence for the effectiveness of cognitive-behaviour therapy (CBT) in addressing mental health difficulties in COPD6,18,21–26 over and above pharmacotherapy in the short term.7 It is also important to integrate a mental health model with a framework of adjusting to a physical health condition. Applying the self-regulatory model,27 which identifies people’s idiosyncratic beliefs about their COPD, the emotional impact and their coping strategies, can help formulate and address a clients’ difficulties within this physical health context. For example, in a previous study, panic symptoms were most prevalent in participants with low perceived control over symptoms and the disease, negative beliefs about the life-limiting consequences of unpredictable breathlessness attacks and by those using emotional coping strategies such as denial and avoidance.28
The COPD breathlessness manual (CM) was developed as a guided self-help intervention that individuals complete in their own time at home, with support from a facilitator. It applies CBT techniques within a self-management framework and specifically targets the cognitive-behavioural aspects of breathlessness and panic, which, it has been indicated, may facilitate greater improvements in health outcomes than PR alone.29 A previous group cognitive-behavioural intervention targeting breathlessness and panic demonstrated a reduction in A&E and hospital admissions as well as improved mood and health status in end-stage COPD patients, resulting in NHS savings.21 The CM was adapted from this intervention. This randomised trial compares the effectiveness of the CM versus British Lung Foundation information booklets (IB) on health service use, mood and health status.
Materials and methods
Study design
This was a prospective, randomised, single-blind, parallel-group trial comparing the CM with British Lung Foundation IB.
Participants
COPD patients (n=1,217) were identified through 10 GP practices in North West London and invited by letter to participate in the trial. Inclusion criteria were: a diagnosis of COPD, verified by being on the COPD disease register at the GP practice (based on the NICE 2010 COPD guidelines30—i.e. a forced expiratory volume in the first second (FEV1)/forced vital capacity (FVC) ratio of less than 0.7, or if FEV1 is equal to or above 80% predicted normal with other respiratory symptoms being present such as breathlessness or cough); a self-rating breathlessness score on the Medical Research Council (MRC) dyspnoea scale31 of 3 or more; willingness to participate; ability to provide informed consent; and ability to read and write in English or with assistance. Exclusion criteria were: known psychosis and personality disorders; receiving psychological therapy; participating in PR, or having had PR within the previous six months; cognitive impairment; dementia; and verbal and/or written communication problems.
Randomisation
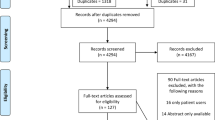
Simple blocked random sampling was undertaken. Computerised random blocks of six at a time were randomised, three in each group. Participants were blind to group allocation. Primary and secondary care staff were aware of patients’ participation in the trial, but were unaware of group allocation and the trial was separate to any clinical care provided. See Figure 1 for trial profile.

Trial profile.
Procedure
Patients who had opted-in were telephoned to discuss the trial, check whether they met the criteria and arrange a home visit. Both groups received a 90-min home visit involving obtaining signed informed consent, baseline measures, a semi-structured interview and introducing the intervention. Participants were encouraged to follow their programme for approximately 1 h per day (broken up throughout the day) over a 5-week period. For example, for the CM, this could include reading a section, writing in a question response, practising a physical exercise (e.g., walking on the spot) and listening to a track from the relaxation CD. For the IB, this involved predominantly reading, but any practical techniques in the booklets (e.g., breathing control) were reinforced. Partners/carers were encouraged to be involved. Participants received two 30-min telephone call booster sessions at weeks 3 and 6.
The CM
The CM was developed by a health psychologist, with multidisciplinary team input and piloted with small focus groups of COPD patients over 6 months. The final version consisted of a 5-week intervention, with each week divided into six sections. For example, week 1: ‘Understanding COPD and the experience of breathlessness’ was divided into the following six sections:
Section 1: What is COPD all about?
Section 2: Focus on breathlessness—part 1
Section 3: How to control breathlessness and panic
Section 4: Daily exercises
Section 5: Relaxation CD: Introduction and exercise 1: Breathing control
Section 6: Summary and weekly record
The main theme was breaking the cognitive-behavioural maintenance cycle of breathlessness, panic, frustration and depression, with a specific focus on ways to manage distress (for both patients and carers) to ultimately prevent inappropriate A&E attendance and hospital admissions. Education on distinguishing between a COPD exacerbation and a panic attack was provided alongside self-management guidance. Shifting unhelpful illness cognitions and encouraging adaptive behaviours using pacing and goal-setting was a central strategy. Breathing control and mobility exercises were demonstrated and trialled and participants were encouraged to practise these daily. Participants were asked to complete self-help tasks as well as a weekly mood and breathlessness rating. The manual was accompanied by a relaxation CD.
IB
Participants received a series of British Lung Foundation COPD booklets and were encouraged to work through them over 5 weeks.
Facilitator input
The facilitators (psychologists) were trained in applying CBT techniques within a physical health context to formulate common cognitive-behavioural maintenance patterns as well as utilising motivational interviewing to facilitate behaviour change. A one-day training workshop consisted of understanding the physical and psychological issues in COPD, the challenges of self-management in COPD, the theory and application of the CBT model for breathlessness, panic and prevention of A&E attendance as well as managing frustration and low mood. In addition, practical role plays were conducted for enhancing skills in assessing patients’ current psychological status, explaining the interaction between emotions and COPD symptoms, motivation (and barriers) to participation, as well as demonstration of exercises and breathing techniques.
Primary outcome: health service use
Frequency of A&E attendance and frequency and duration of COPD-related hospital admissions 12 months pre- and post-intervention were recorded from a district general hospital’s electronic records. Health-care resource group tariffs32 were calculated for each activity.
Secondary outcomes
Mood and health status were measured at baseline, 6 weeks and 6 months using the following questionnaires:
– The Hospital Anxiety and Depression Scale (HADS),33 a validated, widely used measure to screen for anxiety and depression in medical settings. Scores are categorised into: 0 to 7, normal; 8 to 10, borderline; and 11 to 21, clinical levels.
– The Self-Reported Chronic Respiratory Questionnaire (CRQ-SR),34 a reproducible, reliable, and stable measure of health status in chronic lung disease, divided into four domains: (1) Dyspnoea (5 to 35); (2) Fatigue (4 to 28); (3) Emotional function (7 to 49); and (4) Mastery (4 to 28). Higher scores represent better function.
Feedback
Participants were invited to provide feedback using a 1 to 5 Likert scale to various statements such as ‘How would you rate your confidence in managing your COPD after using the programme?’ Open comments were also invited.
Clinical information
Spirometry was obtained at baseline using a portable spirometer. The percent-predicted forced expiratory volume in the first second (FEV1%) was used as an indicator of disease severity. Participants reported on length of diagnosis, details of co-existing medical conditions, current prescribed medication(s) and smoking status.
Sample size
A sample size of 186 was calculated (93 per group) for a 5% significance level and 80% power. This was based on a previous study suggesting that the number of admissions varied by a mean of 0.7 between control and intervention groups. It also indicated that the s.d. of the change in number of admissions was 1.7.21
Statistical analyses
Statistical methods were employed using SPSS for windows version 17.0. Unpaired t-tests on the mean change scores were conducted for A&E visits, hospital admissions and length of stay. Logistic regression was used to predict A&E attendance (attendance versus non-attendance) and hospital admissions (admission versus non-admission). Mixed model analysis of variance was conducted to analyse changes in mood and health status. Data were analysed on an intention to treat basis. Any health service use period culminating in patient fatality was investigated and if coded as COPD-related, was included in subsequent analyses.
Ethics
Ethical approval was obtained from NHS Central REC 3.
Results
Sample characteristics
Eight to 10 participants per week were entered into the trial between January and August 2011. Baseline comparisons with unpaired t-tests and Χ2-tests showed no major differences between groups on demographic measures, FEV1%, mood and health status. More people in the CM group attended A&E (Χ2 (1)=7.893, P=0.005) and were hospitalised (Χ2 (1)=4.833, P=0.03) 12 months pre-study, compared with the IB group (Table 1).
A&E visits
Table 2 shows that in the 12 months post-intervention, total A&E visits in the CM group had fallen by 42%, indicating a cost saving of £6,934.12, whereas A&E visits had increased by 16% in the IB group. Despite this increase in A&E visits, the cost did not rise substantially due to 73% of participants being discharged and a lower A&E tariff being charged. Unpaired t-test on the mean change scores in A&E visits just failed to reach significance (CM group mean change=−0.30, (s.e. 0.09), IB group mean change=0.06, (s.e. 0.16), t (220)=1.994, P=0.047, CI 0.01–0.73, r=0.13).
Thirty-eight percent fewer participants in the CM group visited A&E 12 months post-intervention, compared with a 24% increase in the IB group. A logistic regression model based on entering the variables ‘pre-intervention A&E activity’ and ‘group’ was significant in predicting whether or not participants attended A&E in the 12 months following study participation (Χ2 (2)=16.387, P<0.001). ‘Pre-intervention A&E attendance’ (β=1.160, (s.e. 0.311), P<0.001) and group (β=0.654, (s.e. 0.309), P=0.034) were significant in predicting ‘post-intervention A&E attendance’. The odds of people in the IB group attending A&E 12 months post was 1.9 times higher than for the CM group (CI 1.05–3.53).
Hospital admissions and bed days
All hospital admissions were emergency admissions (via A&E). Table 2 shows that in 12 months, the total number of admissions had fallen by 54 and 23% in the CM and IB group, respectively. Total number of bed days reduced by 61% in the CM group (cost saving £23,263.00) but had increased by 18% in the IB group (cost saving £7,439.00 due to bed days falling under the ‘reduced short stay emergency tariff’32). Unpaired t-tests showed no significant difference between groups on the mean change scores in hospital admissions (CM group mean change=−0.22 (s.e. 0.07), IB group mean change=−0.09, (s.e. 0.13), t (220)=0.927, P=0.36, CI −0.15–0.41, r=0.06) or bed days (CM group mean change=−0.92 (s.e. 0.40), IB group mean change=−0.16 (s.e. 0.62), t (220)=1.033, P=0.30, CI −0.69–2.20, r=0.07).
A logistic regression model based on entering the variables ‘pre-intervention hospital admissions’ and ‘group’ was not significant in predicting whether or not participants were admitted to hospital in the 12 months post-intervention (Χ2 (2)=2.799, P=0.247). See Supplementary Table 1 for logistic regression summary table.
The total savings from the CM at 12 months amounted to £30,197.12, or £269.62 per participant, compared with a £50 cost of delivering the programme.
Mood and health status
All participants completed questionnaires at baseline. Six-week response rate was 63 (n=71) and 62% (n=68) in the CM and IB group, respectively, and at 6 months, 59 (n=60) and 57% (n=61) in the CM and IB group, respectively. See Table 3 for mean scores and s.d. on self-report measures.
Anxiety
At 6 months, 3% remained clinically anxious in the CM group, compared with 23% in the IB group. Mixed model analysis of variance showed a significant main effect of anxiety and time (F (2,198)=3.870 P=0.022) and a significant interaction between anxiety and group (F (2,198)=5.612, P=0.004) (see Figure 2). The contrast between group and anxiety at baseline versus six months was significant (F (1,99)=7.948, P=0.006, r=0.3) as well as at 6 weeks versus 6 months (F (1,99)=7.863, P=0.006, r=0.3).

Estimated marginal means of anxiety over time.
When selecting participants with borderline to clinically significant anxiety at baseline (HADS⩾8), there was a significant main effect of clinical anxiety and time (F (2,92)=12.658, P=0.001), but the interaction between clinical anxiety and group over time just failed to reach significance (F (2,92)=3.181, P=0.046). The contrast between group and clinical anxiety at baseline versus 6 months was significant (F (1,46)=5.247, P=0.027, r=0.3) (see Figure 3).

Estimated marginal means of clinical anxiety over time.
Depression
At 6 months, 7% in the CM group remained clinically depressed, compared with 15% in the IB group. Greenhouse–Geisser estimates showed a significant main effect of depression and time (F (1.8,176.0)=14.179, P⩽0.001) and a significant interaction between depression and group (F (1.8,176.0)=10.697, P⩽0.001) (see Figure 4). The contrast between group and depression at baseline versus 6 months was significant (F (1,99)=10.341, P=0.002, r=0.3) with lower depression levels in the CM group, but not at 6 weeks versus 6 months (F (1,99)=0.378, P=0.540, r=0.1).

Estimated marginal means of depression over time.
Dyspnoea
There was a significant main effect of dyspnoea and time (F (2,188)=18.283, P⩽0.001) and a significant interaction between dyspnoea and group (F (2,198)=18.170, P⩽0.001). The contrast between group and dyspnoea at baseline versus 6 months was significant (F (1,94)=32.835, P⩽0.001, r=0.5) as well as at 6 weeks versus 6 months (F (1,94)=19.953, P⩽0.001, r=0.4) with improved dyspnoea ratings in the CM group.
Fatigue
There was no significant main effect of fatigue and time (F (2,194)=2.574, P=0.079) but a significant interaction between fatigue and group (F (2,194)=9.457, P⩽0.001). The contrast between group and fatigue at baseline versus 6 months was significant (F (1,97)=15.945, P⩽0.001, r=0.4) as well as at 6 weeks versus 6 months (F (1,97)=6.910, P=0.010, r=0.3) with less fatigue reported in the CM group.
Emotional function
Greenhouse–Geisser estimates showed a significant main effect of emotional function and time (F (1.8,175.7)=13.595 P⩽0.001) and a significant interaction between emotional function and group (F (1.8,175.7)=11.453, P⩽0.001). The contrast between group and emotional function at baseline versus 6 months was significant (F (1,96)=17.503, P⩽0.001, r=0.4) as well as at 6 weeks versus 6 months (F (1,96)=13.079, P⩽0.001, r=0.3) with improved emotional function reported in the CM group.
Mastery (control)
There was a significant main effect of mastery and time (F (2,200)=18.241 P⩽0.001) and a significant interaction between mastery and group (F (2,200)=11.212, P⩽0.001). The contrast between group and mastery at baseline versus six months was significant with improved mastery in the CM group (F (1,100)=17.704, P⩽0.001, r=0.4) but not at 6 weeks versus 6 months (F (1,100)=2.081, P=0.152, r=0.1).
Participant feedback
Seventy-eight percent reported that the CM was very useful, 92% reported more confidence in managing COPD, and 79% reported a great improvement to their quality of life. Most useful aspects were discussions on the phone, managing breathlessness and panic, distinguishing anxiety and a flare up, pacing, breathing and relaxation. Improvements included increasing the programme length as well as combining it with group sessions to increase motivation and social contact.
Thirty-seven percent reported that the information booklets were useful and 28% reported an improvement in their quality of life. Participants appreciated the facilitator input, although as a programme, they generally wanted more practical elements in addition to reading information.
Discussion
Main findings
The COPD breathlessness manual (CM) resulted in greater improvements in health-care use, mood and health status, with greater NHS savings, compared to IB. It appears that the latter plus facilitator input is beneficial up to a point, but does not result in long term sustained changes compared to the CBT component underpinning the CM. This is in keeping with previous evidence that providing information is important, but in itself does not lead to significant behaviour change.35
Participants in the IB group were almost twice as likely to attend A&E in the 12 months post intervention, compared to participants in the CM group. At 12 months, A&E visits in the IB group had increased by 16%. Furthermore, the majority of IB participants were discharged from A&E in the 12-month follow-up period, indicating potentially avoidable visits, perhaps due to almost a quarter remaining clinically anxious and reporting greater dyspnoea. In comparison, A&E visits in the CM group had fallen by 42% along with a greater reduction in anxiety and depression.
Interpretation of findings in relation to previously published work
The results of this study replicate the findings from a previous breathlessness group CBT intervention21 and highlight the comparable benefits of delivering CBT in both group and home-based settings. The CM was a targeted intervention and not part of a wider PR or other exercise/education programme. The findings correspond to a recent meta-analysis,36 which showed a small effect of CBT for anxiety and highlighted the need for adequately powered RCT’s disentangling the contributions of exercise training, education and CBT.
This study highlights that providing no CBT intervention leaves potential for psychological problems to escalate and can lead to inappropriate health-care use and increasing NHS costs. It raises the importance of intervening early in COPD with brief targeted CBT interventions, to prevent the development and worsening of anxiety, panic attacks and panic disorder and associated hospital admissions, which has equally been emphasised in previous studies.6,37
The delivery of the CM intervention, i.e., brief with minimal telephone-based support appears feasible and relates to a similar study,25 which found that six weekly sessions and three telephone booster sessions of CBT improved anxiety, depression, mastery and fatigue in COPD. Furthermore, a recent RCT38 provided evidence that a self-managed programme in primary care offering minimal telephone support can lead to health benefits similar to PR.
Strengths and limitations of this study
The CM is the first known ‘manualised’ psychological intervention, targeting breathlessness, panic and prevention of hospital use in COPD. This programme demonstrated clinical and cost-effectiveness, was acceptable to participants, and has the potential to be used in both primary and secondary care.
A number of study limitations should be noted. The response rate to the mailed letters for recruitment was low (25%), making it a small study. A larger study would have enhanced the representativeness and generalisability of the sample to a wider COPD population. Hospital data were collected from a single hospital database, and hence did not account for attendance at hospitals elsewhere. Self-report measures were not collected beyond 6 months, and the moderate follow-up rates may have biased results. Anxious and depressed individuals were not selected per se; rather, COPD was considered to be an innately psychologically challenging condition and research has shown that psychological issues can often go unrecognised and remain untreated in COPD patients.39 It should be noted that a small proportion of participants were taking medication for depression and anxiety, which may have confounded the results, although these percentages were comparable in both groups (16 and 12% reported taking antidepressants from the CM and IB group, respectively; for anxiolytics, this was 4 and 5%).
It is appreciated that motivation and commitment are a prerequisite for patients engaging in guided self-help interventions; likewise, facilitator skills make a huge difference. Both groups received equal facilitator guidance, which in itself may have positively influenced results. The facilitators in the study were psychologists; however, this is not an integral requirement, and a facilitator training workshop has been developed and delivered. This is in keeping with the current emphasis on providing CBT skills training for respiratory nurses and community matrons to help address psychological issues in COPD.40,41 It is recognised that levels of participation in the CM programme would have varied. Fidelity to completing the intervention was discussed during follow-ups, although was not recorded objectively and level of adherence rate would have enhanced the study rigour. Furthermore, it is not possible to state which particular aspect of the CM was most effective, which is necessary for future research.
Implications for future research, policy and practice
The CM is cost-effective and easy to deliver in different settings. It could be particularly beneficial for anxious/depressed individuals, frequent GP or A&E attenders, post exacerbation or as an ‘add-on’ to PR to increase adherence. It could also be implemented within a respiratory service or an Improving Access to Psychological Therapies service in accordance with government policy on addressing mental health in long-term conditions.12 Future research intends to explore the delivery of the CM in different formats such as Telemedicine as well as interventions for carers.
Conclusions
Results show that the CM provided psychological benefit, improved self-management and reduced costs to the NHS in an unselected group. It is emphasised that it should be considered as an option for the majority of COPD patients as a preventative measure, to help them cope better.
References
Cimpean D, Drake RE . Treating co-morbid medical conditions and anxiety/depression. Epidemiol Psychiatr Sci 2011; 20: 141–150.
Brenes GA . Anxiety and chronic obstructive pulmonary disease: prevalence, impact and treatment. Psychosom Med 2003; 65: 963–970.
Yohannes AM, Baldwin RC, Connelly MJ . Depression and anxiety in elderly patients with chronic obstructive pulmonary disease. Age Ageing 2006; 35: 457–459.
Howard C, Hallas CN, Wray J, Carby M . The relationship between illness perceptions and panic in chronic obstructive pulmonary disease. Behav Res Ther 2009, 47: 71–76.
Andenaes R, Kalfoss MH . Psychological distress in hospitalised patients with chronic obstructive pulmonary disease. Eur J Epidemiol 2004; 19: 851–859.
Livermore N, Sharpe L, McKenzie D . Prevention of panic attacks and panic disorder in COPD. Eur Respir J 2010; 35: 557–563.
Usmani ZA, Cheng NJ, Smith BJ, Carson KV . A meta-analysis (Cochrane review) of pharmacological and psychological interventions for anxiety and depression in COPD. Respirology 2010; 15: 1323–7799.
Coventry PA, Gemmell I, Todd CJ . Psychosocial risk factors for hospital readmission in COPD patients on early discharge services: a cohort study. BMC Pulm Med 2011; 11: 49.
Ng TP, Niti M, Tan WC, Cao Z, Ong KC, Eng P . Depressive symptoms and chronic obstructive pulmonary disease: Effect on mortality, hospital readmission, symptom burden, functional status and quality of life. Arch Intern Med 2007; 167: 60–67.
Dahlen I, Janson C . Anxiety and depression are related to the outcome of emergency treatment in patients with obstructive pulmonary disease. Chest 2002; 122: 1633–1637.
Coultas D, Edwards DW, Barnett B, Wludyka P . Predictors of depressive symptoms in patients with COPD and health impact. COPD 2007; 4: 23–28.
Naylor C, Parsonage M, McDaid D, Knapp M, Fossey M, Galea A . Long-term conditions and mental health. The cost of co-morbidities. The King’s Fund and Centre for Mental Health. The King’s Fund, London 2012; 1–32.
Al-shair K, Dockry R, Mallia-Milanes B, Kolsum U, Singh D, Vestbo J . Depression and its relationship with poor exercise capacity, BODE index and muscle wasting in COPD. Resp Med 2009; 103: 1572–1579.
Fan VS, Ramsey SD, Giardino ND, Make BJ, Emery CF, Diaz PT et al. Sex, depression, and risk of hospitalization and mortality in chronic obstructive pulmonary disease. Arch Intern Med 2007; 167: 2345–2353.
Omachi TA, Katz PP, Yelin EH, Gregorich SE, Iribarren C, Blanc PD et al. Depression and health-related quality of life in chronic obstructive pulmonary disease. Am J Med 2009; 122: 778.
Yohannes AM . Palliative care provision for patients with chronic obstructive pulmonary disease. Health Qual Life Outcomes 2007; 5: 1–6.
Clark DM . A cognitive approach to panic. Behav Res Ther 1986; 24: 461–470.
Heslop K, Foley T . Using cognitive behavioural therapy to address the psychological needs of patients with COPD. Nurs Times 2009; 105: 18–19.
Lacasse Y, Goldstein R, Lasserson TJ, Martin S . Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2006; 4: Art. No.: CD003793.
Grant AR, Sutton SR . Interventions for adherence to pulmonary rehabilitation for chronic obstructive pulmonary disease (Protocol). Cochrane Database Syst Rev 2009; 1: Art No.: CD005605.
Howard C, Dupont S, Haselden B, Lynch J, Wills P . The effectiveness of a group cognitive-behavioural breathlessness intervention on health status, mood and hospital admissions in elderly patients with chronic obstructive pulmonary disease. Psychol Health Med 2010; 15: 371–385.
Baraniak A, Sheffield D . The efficacy of psychologically based interventions to improve anxiety, depression and quality of life in COPD: a systematic review and meta-analysis. Patient Educ Couns 2011; 83: 29–36.
Ramsenthaler C, Siegert RJ, Weatherall M, Bausewein C, Koffman J, Higginson IJ et al. Cognitive behavioural therapy (CBT) for panic and anxiety in chronic obstructive pulmonary disease—a systematic review. Palliat Med 2012; 26: 0269–2163.
Hynninen MJ, Bjerke N, Pallesen S, Bakke PS, Nordhus IH . A randomized controlled trial of cognitive behavioral therapy for anxiety and depression in COPD. Respir Med 2010; 104: 986–994.
Cully JA, Stanley MA, Deswal A, Hanania NA, Phillips LL, Kunik ME . Cognitive-behavioral therapy for chronic cardiopulmonary conditions: preliminary outcomes from an open trial. Prim Care Companion J Clin Psychiatry 2010; 12: pii: PCC.09m00896.
Coventry PA, Gellatly JL . Improving outcomes for COPD patients with mild-to-moderate anxiety and depression: a systematic review of cognitive behavioural therapy. Br J Health Psychol 2008; 13: 381–400.
Leventhal II, Meyer D, Nerenz DR . The Common Sense Representations of Illness Danger. In Rachman S (ed.) Contributions to Medical Psychology. Pergamon: New York, 1980: 17–30.
Hallas CN, Howard C, Theadom A, Wray J . Negative beliefs about breathlessness increases panic for patients with chronic respiratory disease. Psychol Health Med 2012; 17: 467–477.
Cafarella P, Williams MT, Petkov J, Frith P . Cognitive behavioural therapy for modifying sensations of breathlessness in people with COPD. Respirology 2010; 5: 1323–7799.
National Institute for Health and Clinical Excellence. Chronic obstructive pulmonary disease: Management of chronic obstructive pulmonary disease in adults in primary and secondary care (partial update). NICE Clinical Guideline 101, June 2010. https://www.nice.org.uk/guidance/cg101.
Fletcher CM, Elmes PC, Fairbairn MB, Wood CH . The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. BMJ 1959; 2: 257–266.
Department of Health. 2011-12 tariff information spreadsheet—revised on 23 March 2011. Available at http://webarchive.nationalarchives.gov.uk/20130507170152/https://www.gov.uk/government/publications/confirmation-of-payment-by-results-pbr-arrangements-for-2011-12 (first accessed online in August 2011).
Zigmond AS, Snaith RP . The hospital anxiety and depression scale. Acta Psychiatr Scand 1983; 67: 361–370.
Williams J, Singh S, Sewell L, Guyatt GH, Morgan MDL . Development of a self-reported Chronic Respiratory Questionnaire (CRQ-SR). Thorax 2001; 56: 954–959.
Newman S, Steed L, Mulligan K . Self-management interventions for chronic illness. Lancet 2004; 364: 1523–1537.
Ramsenthaler C, Siegert RJ, Weatherall M, Bausewein C, Koffman J, Higginson IJ et al. Cognitive behavioural therapy (CBT) for panic and anxiety in chronic obstructive pulmonary disease—a systematic review. Pall Med 2012; 26: 405–406.
Willgoss TG, Yohannes AM, Goldbart J, Fatoye F . ‘Everything was spiralling out of control’. Experiences of anxiety in people with chronic obstructive pulmonary disease. Heart Lung 2012; 41: 562–571.
Horton E, Mitchell K, Jonhson-Warrington V, Apps L, Young H, Singh S . A self-management programme of activity, coping and education (SPACE) for COPD: a randomised non-inferiority trial in a pulmonary rehabilitation population. Thorax 2013; 68: A15–A16.
Fritzsche A, Clamor A, Von Leupoldt A . Effects of medical and psychological treatment of depression in patients with COPD—a review. Respir Med 2011; 105: 1422–1433.
Heslop K, Newton J, Baker C, Burns G, Carrick-Sen D, De Soyza A . Effectiveness of cognitive behavioural therapy (CBT) interventions for anxiety in patients with chronic obstructive pulmonary disease (COPD) undertaken by respiratory nurses: the COPD CBT CARE study: (ISRCTN55206395). BMC Pulm Med 2013; 13: 62.
Barker D, Davies C, Dixon B, Hodgson A, Reay S, Barclay N . Training community matrons in basic cognitive behavioural therapy-based techniques for patients with COPD. Br J Community Nurs 2014; 19: 274–283.
Acknowledgements
Thanks to Mr Paul Bassett and Dr Gordon Taylor for advice on statistical analysis.
Author information
Authors and Affiliations
Contributions
CH contributed to the design and implementation of the study, enrolment and follow-up of participants, data collection, statistical analysis and interpretation of results and writing of the report. SD contributed to the study conception and design. SD acted as the guarantor for the study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Howard, C., Dupont, S. ‘The COPD breathlessness manual’: a randomised controlled trial to test a cognitive-behavioural manual versus information booklets on health service use, mood and health status, in patients with chronic obstructive pulmonary disease. npj Prim Care Resp Med 24, 14076 (2014). https://doi.org/10.1038/npjpcrm.2014.76
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/npjpcrm.2014.76
This article is cited by
-
Systematic review of effectiveness and quality assessment of patient education materials and decision aids for breathlessness
BMC Pulmonary Medicine (2022)
-
Psychosocial Evaluation for Lung Transplantation: an Empirically Informed Update
Current Transplantation Reports (2022)
-
Management of Refractory Breathlessness: a Review for General Internists
Journal of General Internal Medicine (2021)
-
Systematic review of the effectiveness of community-based self-management interventions among primary care COPD patients
npj Primary Care Respiratory Medicine (2018)
-
The Breathing, Thinking, Functioning clinical model: a proposal to facilitate evidence-based breathlessness management in chronic respiratory disease
npj Primary Care Respiratory Medicine (2017)
