
Abstract
Post-transplantation lymphoproliferative disorder is an aggressive complication of transplantation, most frequently of diffuse large B-cell lymphoma morphology and associated with Epstein–Barr virus (EBV) infection/reactivation. In this study the microenvironment of EBV+ (n=23) and EBV− (n=9) post-transplant non-germinal center B-cell diffuse large B-cell lymphoma was characterized. Of EBV+ cases somatic hypermutation analysis, gene expression profiling, and extensive phenotyping were performed. Our results demonstrated variable cytotoxic T-cell infiltration and significantly increased CD163+ M2 macrophage infiltration in EBV+ compared with EBV− post-transplant diffuse large B-cell lymphoma. On the basis of IgM staining and hypermutation analysis, two EBV+ post-transplant diffuse large B-cell lymphoma subgroups were identified: IgM+ tumors lacking somatic hypermutations and IgM− tumors harboring somatic hypermutations. IgM− tumors arose late following transplantation (median interval: 16 months), mainly in kidney recipients. IgM+ tumors on the other hand arose early (median interval: 3 months, P-value=0.0032), almost exclusively following stem cell transplantation and were associated with worse outcome (median survival 1 month for IgM+ versus 41 months for IgM− tumors, log-rank/Wilcoxon P-value 0.07/0.04). Notably, IgM+ tumors were characterized by plasma cell features (monotypic kappa/lambda expression, high MUM1 expression, and partial CD138 expression) and a high proliferation index. Consistent with the plasma cell phenotype, unfolded protein response signaling was upregulated. In contrast, IgM− EBV+ post-transplant diffuse large B-cell lymphoma did not express kappa, lambda, IgD, or CD138 and expressed limited MUM1. In these tumors T-cell signaling was enhanced associated with increased T-cell infiltration compared with IgM+ cases. Overall, our results allow further molecular classification of EBV+ post-transplant diffuse large B-cell lymphoma and provide a rationale for the use of subtype-specific-targeted therapies (eg, bortezomib in IgM+ tumors). Our findings also provide a biological basis for the clinical differences between post-transplant lymphoproliferative disorder following solid organ and stem cell transplantation, which are regarded as different disorders.
Similar content being viewed by others


Main
Post-transplantation lymphoproliferative disorders affect a rising number of transplant recipients due to the increasing frequency of transplantations performed, more potent immunosuppressive medication, and prolonged survival following transplantation. The most common malignant subtype is post-transplant diffuse large B-cell lymphoma, which is positive for the Epstein–Barr virus (EBV) in the majority, but not all cases.1 This raises an important question: are EBV-positive (EBV+) and -negative (EBV−) post-transplant lymphomas different? We previously reported that EBV+ post-transplant diffuse large B-cell lymphoma is associated with innate immune responses and immunotolerance.2 These results suggested that the microenvironment is greatly impacted by the presence of EBV. A number of studies already touched on this subject,3, 4 however a thorough histopathological study of the non-malignant stromal component of post-transplant diffuse large B-cell lymphoma has not been performed.
In contrast to diffuse large B-cell lymphoma in the general population (which is mostly unrelated to EBV and can be of germinal center B-cell or non-germinal center B-cell origin), the vast majority of EBV-associated diffuse large B-cell lymphoma is of non-germinal center B-cell origin.5, 6, 7 The induction by EBV of pathways like NF-κB signaling, which is highly characteristic for non-germinal center B-cell diffuse large B-cell lymphoma could explain this observation.8 The non-germinal center B-cell origin of post-transplant lymphoproliferative disorders is supported by the presence of somatically hypermutated immunoglobulin variable chains (IgV) in the majority of these tumors.5, 9 However, a few rare cases that lack somatic hypermutation have been reported.10, 11, 12 Their origin is currently unclear.
Except for a number of consensus epidemiological risk factors (age at transplantation, EBV seronegativity, graft type, and immunosuppressive therapy regimen13), there are currently few clues available to predict which transplant recipients will eventually develop post-transplant lymphoproliferative disorders. In accordance with the presumed role of EBV as a key driver of pathogenesis, EBV+ post-transplant diffuse large B-cell lymphoma generally arises earlier following transplantation than EBV− post-transplant lymphoproliferative disorders. However, also within the subgroup of EBV+ post-transplant lymphoproliferative disorders the interval between transplantation and post-transplant lymphoproliferative disorder onset varies considerably. In hematopoietic stem cell recipients EBV+ post-transplant diffuse large B-cell lymphoma arises within weeks to months,14 whereas in solid organ recipients EBV+ post-transplant diffuse large B-cell lymphoma may still occur several years after transplantation.15 Low levels of anti-EBV cytotoxic T-lymphocyte precursors following hematopoietic stem cell transplantation could contribute to this higher risk of early onset post-transplant lymphoproliferative disorder.16 In the context of immunosuppression, uncontrolled lytic EBV replication has also been associated with early lymphoma onset.17 Except for increasing the spread of EBV, lytic replication is thought to contribute to early lymphomagenesis through upregulation of B-cell growth promoting factors. A key factor in this process is ZEBRA (BZLF-1, Zta), the main viral activator of EBV lytic replication.18, 19, 20 Expression of ZEBRA in EBV+ B cells is tightly regulated allowing EBV to establish long-term latency. The particular stimuli that naturally induce lytic replication are currently not defined, but several studies have shown that networks governing plasma cell differentiation are also involved in the balance between EBV latency and replication.21, 22 EBV lytic replication in EBV+ post-transplant lymphoproliferative disorder has been described,17 however the clinical and biological consequences are not clear.
In this study, a homogenous series of EBV+ and EBV− post-transplant diffuse large B-cell lymphoma was thoroughly characterized to study the composition of the microenvironment, the IgV mutation status, and latent and lytic EBV protein expression. These features were associated with clinical features and the tumor immunophenotype. Our results suggest that two clinically relevant subgroups of EBV+ post-transplant diffuse large B-cell lymphoma exist related to the occurrence of somatic hypermutation and associated with a particular phenotype.
Materials and methods
Case Selection
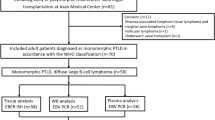
To prevent the introduction of bias, only cases of non-germinal center B-cell diffuse large B-cell lymphoma (immunohistochemically defined using the Hans algorithm23) were selected. We used a selection of diffuse large B-cell lymphoma (32 post-transplant diffuse large B-cell lymphoma, 19 diffuse large B-cell lymphoma in immunocompetent individuals), a part of which was previously reported.2 Clinical data were retrieved from the medical records and summarized in Table 1. This study was approved by the Ethical Committee of UZ Leuven (S55498) and was conducted according to the Declaration of Helsinki.
EBV-Encoded RNA In Situ Hybridization and Immunohistochemistry
All stainings were performed on formalin-fixed paraffin-embedded sections. EBV-encoded RNA in situ hybridization was performed to define the presence of EBV as previously described.2 We used two antibody panels to characterize (1) the tumor cells (Ki67, MUM1, CD138, kappa, lambda, IgM, IgD, IgG, IgA, and PDL1) and (2) the microenvironment (CD3, CD4, CD8, granzyme B, perforin 1, TIA1, FOXP3, and PD1 for T-cell subsets; CD138 for plasma cells; CD56/NCAM1 for NK cells; CD68/PGM1, CD163 for macrophages). Expression of tumor markers was estimated (in percentage) taking into account the entire tissue section. The stromal infiltrate was quantified based on positive cell counting in five high-power fields (hpf, x400). Peripheral and necrotic regions were not considered for scoring and cell counting.
The EBV latency profile was determined based on the staining pattern of LMP1 and EBNA2 latency proteins: latency III (LMP1+/EBNA2+), latency II (LMP1+/EBNA2−), latency I (LMP1−/EBNA2−/EBNA1+), latency 0 (LMP1−/EBNA2−/EBNA1−).
The occurrence of lytic EBV was defined by staining for the viral protein ZEBRA. The median number of ZEBRA+ cells was calculated based on counts of ZEBRA+ nuclei in five hpf. ZEBRA+ cells were homogenously scattered throughout the biopsies.
Automated sequential double stainings were performed of EBV-encoded RNA with CD8/CD163 (case 5) and ZEBRA with CD138 (case 19).
Details about antibody clones and staining conditions are summarized in Supplementary Table 1.
Quantitative RT-PCR
Expression of sXBP1 (forward primer 5′-AGACAGCGCTTGGGGATGGAT-3′; reverse primer 5′-CCTGCACCTGCTGCGGACTC-3′) was examined by RT-PCR according to standard methods (in cases 1, 3, 4, 6, 7, 12, 13, 15, and 19–23). Cases were selected based on the availability of fresh frozen tissue and RNA quality. Briefly, total RNA was extracted from 20 μm sections of each frozen tissue sample using the RNeasy mini kit (Qiagen, Venlo, the Netherlands) according to the manufacturers’ recommendations. RNA quality and concentration were measured using a Nanodrop spectrophotometer (Nanodrop Technologies, Wilmington, DE, USA). Of each total RNA sample, 1 μg was used for cDNA synthesis (iScript cDNA Synthesis Kit; Bio-Rad Laboratories, Irving, CA, USA). RT-PCR assays were performed in duplo using Fast SYBR Green Master Mix (Applied Biosystems, Foster City, CA, USA) according to the manufacturer’s protocol. Normalization was done using RPL13A (forward primer 5′-GTGAAGGCATCAACATTTCTG-3′; reverse primer 5′-GATAGGCAAACTTTCTTGTAGG-3′) as housekeeping gene. All primers were custom made (Invitrogen, Carlsbad, CA, USA).
Somatic Hypermutation Assay
The somatic hypermutation assay was performed on 19 cases of post-transplant diffuse large B-cell lymphoma (1–4, 6–9, 11–14, 16, and 18–23) by standard methods from the clinical laboratory, UZ Leuven.
Briefly, DNA was extracted from fresh frozen tissue using the Invisorb Spin Forensic kit (Stratec Biomedical AG, Germany). Amplification of IGHV regions by polymerase chain reaction was performed using VH framework region 1 consensus family specific primers (VH1-VH6), FR1C, and JH primers. Thermal cycling conditions were 12 min at 94 °C, followed by 32 cycles at 92 °C for 30 s, 64 °C for 15 s, 72 °C for 20 s, elongation at 72 °C for 10 min, and a final step at 4 °C for 5 min. High-resolution capillary electrophoresis was performed using the Qiaxcel system (Qiagen, Germany). Sequencing was performed using the ABI 3730xl Genetic Analyzer (Thermo Fisher Scientific, USA). The mutational status of the IgV region was ultimately determined using the IMGT database.24 In case of >2% or greater mutation frequency, the IgV region was considered as mutated.
Gene Expression Profiling
Microarray gene expression data were available for a subset of 17 previously published EBV+ post-transplant diffuse large B-cell lymphoma that were IgM− (n=12; cases 1–12) or IgM+ (n=5; cases 17–21) (gene expression profiling data are available at GEO GSE38885). Hierarchical clustering and inference analysis to identify differentially expressed genes were performed as previously described.2 Criteria for significance were P-value <0.001 and absolute fold change of 1.5.
Pathway Analysis
To identify significantly enriched gene networks, relevant pathways and biological functions in IgM+ and IgM− EBV+ post-transplant diffuse large B-cell lymphoma, the results of inference analysis were uploaded into the ‘Ingenuity Pathway Analysis’ application (IPA, www.ingenuity.com). Only species ‘human’ was selected and from the three confidence levels provided by the system, ‘Experimentally observed’ and ‘Highly predicted’ data were used.
Statistical Analysis
Statistical test included Kaplan–Meier overall survival analysis, non-parametric t-test, χ2-test and Fisher’s exact test performed with Graphpad Prism 5 software. The threshold for statistical significance was P-value <0.05.
Results
Overall, the series consisted of 23 EBV+ non-germinal center B-cell post-transplant diffuse large B-cell lymphoma (cases 1–23), 9 EBV− non-germinal center B-cell post-transplant diffuse large B-cell lymphoma (cases 24–32), and 19 control non-germinal center B-cell diffuse large B-cell lymphoma from immunocompetent individuals (cases 33–51). The clinical features of all cases were summarized in Table 1. Immunophenotypic data are listed in Table 2 (EBV+ post-transplant diffuse large B-cell lymphoma) and Supplementary Table 2 (EBV− post-transplant diffuse large B-cell lymphoma, control diffuse large B-cell lymphoma). Compared with our previous report2 the present post-transplant diffuse large B-cell lymphoma series contained a larger fraction of hematopoietic stem cell transplants (32% versus 13% in the total series), which may account for the younger age at post-transplant lymphoproliferative disorder diagnosis and the shorter interval between transplantation and diagnosis (Supplementary Table 3, Dierickx et al25).
In the EBV+ post-transplant diffuse large B-cell lymphoma series, 52% (12/23) had plasmacytoid features. Partial CD138 expression was detected in half of the cases (11/21). MUM1 expression was highly variable (1–99%) with most cases (17/21) showing expression in ≥20% of the tumor cells.
Overall, there was no clear correlation between the presence of plasmacytoid features and expression of MUM1, CD138, kappa, or lambda. Most cases with high MUM1 expression (>50% of tumor cells) had plasmacytic features (8/11).
Regarding EBV protein expression, latency III (15/22, 68%) and II (5/22, 23%) were most frequent. EBV lytic replication (1–52 ZEBRA+ cells per hpf) was detected in 16/23 cases in large and/or small lymphoid cells. Morphologically the large ZEBRA+ cells corresponded to neoplastic B cells, whereas the smaller positive cells were likely non-tumoral B cells. No correlation between the occurrence of lytic replication and necrosis was apparent.
In our small series of EBV− post-transplant diffuse large B-cell lymphoma MUM1 expression was variable; CD138 was virtually absent in all cases and light-chain expression was limited.
EBV+ Post-Transplant Diffuse Large B-Cell Lymphoma was Associated with Increased Infiltration of T cells and M2 Macrophages
The presence of EBV significantly impacted immune cell infiltration in post-transplant diffuse large B-cell lymphoma lesions. The pan T-cell marker CD3 demonstrated fewer T cells in post-transplant compared with diffuse large B-cell lymphoma in immunocompetent individuals (median 197 cells per hpf versus 346 cells per hpf, P-value <0.0001). The same was true for the CD8+ cytotoxic T cells (median 85 cells per hpf versus 279 cells per hpf, P-value <0.0001) (not shown). In EBV+ compared with EBV− post-transplant diffuse large B-cell lymphoma, the overall number of T cells (median 198 cells per hpf versus 135 cells per hpf, P-value 0.5; Figure 1a) as well as of cytotoxic T cells, in particular, (median 100 cells per hpf versus 67 cells per hpf, P-value 0.1; Figure 1b) was not significantly different.

Comparison of immune cell markers in post-transplant Epstein–Barr virus positive post-transplant diffuse large B-cell lymphoma (EBV+ PT), EBV-negative post-transplant diffuse large B-cell lymphoma (EBV− PT), and EBV− diffuse large B-cell lymphoma in immunocompetent individuals (EBV− IC). Statistical comparisons include EBV+ versus EBV− PT, EBV+ PT versus EBV− IC, and EBV− PT versus EBV− IC. T-cell infiltration was variable in EBV+ PT, but not significantly different from EBV− PT. T-cell infiltration in both the PT groups was decreased compared with EBV− IC (a–b). Granzyme B expression in EBV+ PT was comparable to EBV− IC and significantly higher than in EBV− PT (c). Infiltration of natural killer cells (d) was limited in all subgroups. Regulatory T cells were increased in EBV− IC compared with EBV+ PT (e). A few EBV+ PT cases harbored infiltrating plasma cells (f). Overall, macrophage infiltration was similar in the three subgroups (g), however M2 macrophages were more abundant in EBV+ PT compared with the other groups (h). Double staining (in case 5) demonstrated accumulation of cytotoxic T cells (i, brown) and M2 macrophages (j, brown) in areas of EBV+ post-transplant diffuse large B-cell lymphoma (EBV-encoded RNA in blue).
Analysis of the cytotoxic cell marker granzyme B expression revealed more positive cells in EBV+ post-transplant diffuse large B-cell lymphoma compared with EBV− post-transplant diffuse large B-cell lymphoma (median 48 cells per hpf versus 14 cells per hpf, P-value 0.038; Figure 1c). Also staining for perforin 1 and TIA1 demonstrated a trend for more perforin 1-positive and TIA1-positive cells in EBV+ post-transplant diffuse large B-cell lymphoma compared with EBV− post-transplant diffuse large B-cell lymphoma (median 63 cells per hpf versus 7 cells per hpf, respectively, for perforin 1, P-value 0.3; median 53 cells per hpf versus 37 cells per hpf, respectively, for TIA1, P-value 0.2) (Supplementary Figure 1). Testing for CD56 showed few infiltrating positive cells (Figure 1d), therefore the cells expressing cytotoxic markers most likely represent activated cytotoxic T cells rather than natural killer cells.
FOXP3-expressing regulatory T cells were virtually absent in all subgroups (Figure 1e). Overall very few CD4+ T cells were present in the post-transplant diffuse large B-cell lymphoma lesions, independently of the EBV status (not shown). PD1-expressing cells were rare in all tested cases (not shown). PDL1 staining was performed on five EBV+ post-transplant and three EBV− post-transplant diffuse large B-cell lymphomas. PDL1 expression was more extensive in EBV+ (range 10–80%) versus EBV− cases (range 0–10%) and was found both in tumor cells and macrophages (Supplementary Figure 2).
On the basis of CD138 staining, a few cases of EBV+ post-transplant diffuse large B-cell lymphoma were found to contain infiltrating plasma cells (Figure 1f).
There was no difference in the amount of CD68+ macrophages infiltrating EBV+ and EBV− diffuse large B-cell lymphoma in transplant and immunocompetent patients (Figure 1g). CD163+ M2-polarized macrophages were equally abundant in EBV− diffuse large B-cell lymphoma in transplant and immunocompetent patients, but they were markedly increased in EBV+ post-transplant diffuse large B-cell lymphoma (median 165 cells per hpf in EBV+ versus 82 cells per hpf in EBV− post-transplant diffuse large B-cell lymphoma, P-value 0.018) (Figure 1h).
Double stainings demonstrated accumulation of cytotoxic T cells and M2 macrophages in the region where the EBV+ tumor cells were located, confirming the association between EBV, cytotoxic T cells (Figure 1i, left panel), and M2 macrophage infiltration (Figure 1j).
Two Subgroups of EBV+ Post-Transplant Diffuse Large B-Cell Lymphoma were Associated with a Particular Immunophenotype, IgV Mutation Status, and EBV Protein Expression
On the basis of IgM staining two subgroups of EBV+ post-transplant diffuse large B-cell lymphoma were distinguished, further referred to as IgM+ (n=10) and IgM− post-transplant diffuse large B-cell lymphoma (n=13). To analyze the association between IgM expression and other plasma cell features in EBV+ post-transplant diffuse large B-cell lymphoma, stainings for plasma cell-related markers (kappa, lambda, MUM1, IgD, IgG, IgA, and CD138) were performed (Table 2 and Figure 2). IgM+ tumor cells demonstrated monotypic cytoplasmic light-chain expression (6/10 for kappa, 4/10 for lambda), showed high expression of MUM1 (median 83% of tumor cells), and were (partially) positive for IgD. In contrast, IgM− tumors expressed MUM1 in only a fraction of the tumor cells (median 20% of tumor cells) and were negative for IgD. CD138, a marker of mature plasma cells, was co-expressed in a fraction of tumor cells in IgM+ post-transplant diffuse large B-cell lymphoma (median 12% of tumor cells), whereas tumor cells of IgM− cases did not express CD138. All tumors were negative for IgA. Notably, Ki67 staining demonstrated a difference in proliferation: the median proliferative index was 90% versus 50% in IgM+ and IgM−, respectively (P-value <0.02) (Table 2 and Figure 2). Review of tumor morphology demonstrated that plasmacytoid features were more typical for IgM+ cases. Necrosis was frequent in both subgroups (Table 2).

Immunophenotype of IgM+ and IgM− EBV+ non-germinal center B-cell post-transplant diffuse large B-cell lymphoma. Representative images of IgM+ (a, case 23) and IgM− (b, case 4) EBV+ post-transplant diffuse large B-cell lymphoma. (a) Hematoxylin–eosin staining demonstrated frequent plasmacytic features of IgM+ diffuse large B-cell lymphoma tumor cells, also characterized by high expression of kappa or lambda light chains, MUM1, and IgD indicative of a plasma cell-associated immunophenotype. Tumoral expression of the mature plasma cell marker CD138 was variable (left panel case 23, right panel case 20). The vast majority of tumor cells was actively proliferating (Ki67). ZEBRA expression, representing EBV lytic replication, was common. In contrast, in IgM− diffuse large B-cell lymphoma the tumor cells did not express antibody and MUM1 expression was more limited. A lower fraction of tumor cells proliferated. ZEBRA expression was limited or absent. Images were taken with a Leica microscope at x200 magnification. EBV, Epstein–Barr virus.
A hypermutation assay performed on 19 EBV+ post-transplant diffuse large B-cell lymphoma demonstrated somatic hypermutation in IgM− lesions (n=4/11, seven assays failed), but not in the IgM+ lymphomas (n=6/8, two assays failed) (Table 2). Of note, failure of the hypermutation assay (which occurred in 9/19, particularly IgM− cases) could be due to a high number of somatic hypermutations, impeding primer binding.
Analysis of the EBV latency pattern demonstrated latency III expression in all IgM+ cases tested, whereas half of IgM− tumors (7/13) expressed latency II, I, or 0 (Table 2). Overall, more lytic cells were found in IgM+ (median 17 cells per hpf) compared with IgM− tumors (median <1 cell per hpf) (P-value 0.007).
CD138-ZEBRA double staining did not reveal co-expression of ZEBRA and CD138 (Supplementary Figure 3).
IgM+ Post-Transplant Diffuse Large B-cell Lymphoma was Associated with Early Onset Following Hematopoietic Stem Cell Transplantation
Analysis of clinical data revealed that IgM+ post-transplant diffuse large B-cell lymphoma was associated with hematopoietic stem cell transplantation (90%), whereas IgM− tumors occurred primarily in kidney transplants (46%). Notably, 6/8 IgM+ tumors developed during antiviral treatment (mainly acyclovir). The interval between transplantation and onset of diffuse large B-cell lymphoma was significantly shorter for IgM+ tumors compared with IgM− tumors (median 3 months versus 16 months, P-value 0.0032). IgM+ tumors were associated with worse outcome (IgM+ versus IgM− post-transplant diffuse large B-cell lymphoma, log-rank/Wilcoxon P-value 0.07/0.04) (Supplementary Figure 4), however, this could be influenced by non-post-transplant lymphoproliferative disorder-related cause of death (60% of EBV+ post-transplant diffuse large B-cell lymphoma patients died of sepsis or multi-organ failure).
IgM− Post-Transplant Diffuse Large B-cell Lymphoma was Associated with Infiltration of T cells
The association with hematopoietic stem cell transplantation, elaborate EBV latent protein expression, and lytic replication suggested that IgM+ post-transplant diffuse large B-cell lymphoma arises in the most severely immunocompromised transplant recipients. Reanalysis of the immune cell counts demonstrated more limited T-cell infiltration in IgM+ lesions (median 141 cells per hpf), compared with IgM− lesions (median 334 cells per hpf) but this was not significant (P-value 0.05). A similar trend was observed for cytotoxic T cells (median 95 cells per hpf in IgM+ versus 161 cells per hpf in IgM− tumors, P-value 0.37) and the associated granzyme B expression (median 49 cells per hpf in IgM+ versus 72 cells per hpf in IgM− tumors, P-value 0.37).
None of the other comparisons was informative.
IgM+ Post-Transplant Diffuse Large B-cell Lymphoma was Associated with Endoplasmic Reticulum Stress
Pathway analysis was performed using the gene expression profiling data available for 17 EBV+ post-transplant diffuse large B-cell lymphoma cases. Comparison of IgM+ (n=5) with IgM− (n=12) EBV+ post-transplant diffuse large B-cell lymphoma identified 142 differentially expressed genes, including 85 upregulated and 57 downregulated. The top dysregulated pathways in IgM− cases were involved in T-cell signaling (‘Regulation of IL2 Expression in Activated and Anergic T Lymphocytes’, ‘CTLA4 Signaling in Cytotoxic T Lymphocytes', ‘FAK Signaling’, ‘T Cell Receptor Signaling’) (Figure 3a). Upregulation of these pathways is consistent with increased T-cell infiltration in IgM− compared with IgM+ EBV+ post-transplant diffuse large B-cell lymphoma.

Unfolded protein response signaling was enhanced in IgM+ post-transplant diffuse large B-cell lymphoma. (a) Canonical pathways based on genes differentially expressed in IgM+ and IgM− EBV+ post-transplant diffuse large B-cell lymphoma were defined using IPA software. Red/green indicates upregulation in IgM+/IgM− cases, respectively. Pathways are listed on the y axis. The bold numbers on the right represent the number of molecules involved in each pathway. The top x axis shows the fraction of genes grouped in a particular pathway. The bottom x axis shows the –log(P-value) for each pathway. (b) RT-PCR for spliced XBP1 (sXBP1) demonstrated upregulation in IgM+ compared with IgM− post-transplant diffuse large B-cell lymphoma (P-value 0.0012). The numbers under the bars correspond to the case numbers. EBV, Epstein–Barr virus.
In IgM+ post-transplant diffuse large B-cell lymphoma IPA predicted enhanced ‘Unfolded Protein Response’ signaling (Figure 3a) represented by upregulation of XBP1 (FC 3.3; P-value 6.10−4) and ATF6 (FC 1.5; P-value 6.10−5). Enhanced unfolded protein response signaling was confirmed by RT-PCR for the spliced variant of XBP1 mRNA on six IgM+ (cases 15, 19–23) and seven IgM− EBV+ post-transplant diffuse large B-cell lymphoma (cases 1, 3, 4, 6, 7, 12, and 13) (P-value 0.0012) (Figure 3b).
Discussion
The results of this study indicate (1) that the presence of EBV has a significant impact on the composition of the microenvironment of post-transplant diffuse large B-cell lymphoma and (2) that two subgroups of EBV+ post-transplant diffuse large B-cell lymphoma exist associated with distinct clinical and biological features.
In our series we found variable numbers of T cells in general and cytotoxic T cells in particular in EBV+ post-transplant diffuse large B-cell lymphoma biopsies, indicating increased T-cell infiltration in some but not all EBV+ post-transplant diffuse large B-cell lymphoma. M2-polarized macrophages were abundant in EBV+ compared with EBV− diffuse large B-cell lymphoma in transplant and immunocompetent patients, confirming previously published gene expression profiling data.2 The presence of M2 macrophages together with overexpression of genes involved in immunotolerance (PDL1, IDO1) suggests that in EBV+ diffuse large B-cell lymphoma the immune system is (locally) actively suppressed. Nevertheless, the expression of granzyme B, perforin 1, and TIA1 in the cytotoxic T cells suggests these cells are functional.
In line with the previous reports, regulatory T cells were rarely detected in post-transplant diffuse large B-cell lymphoma. This may be attributed to obstruction of regulatory T-cell development by immunosuppressive agents. Analysis of the normal intestinal mucosa showed that liver transplant patients on a long-term combination regimen had significantly lower levels of regulatory T cells compared with healthy controls.26
Notably, similar findings have been reported for EBV+ classic Hodgkin lymphoma. A gene expression study found upregulation of antiviral signaling and macrophage-related genes (among which CD163) in EBV+ samples.27 In vitro, EBV was shown to induce PDL1 expression28 providing an explanation for PDL1 overexpression.
On the basis of staining for IgM and analysis of somatic hypermutation, two subgroups of EBV+ post-transplant diffuse large B-cell lymphoma were distinguished.
IgM−-mutated post-transplant diffuse large B-cell lymphoma was associated with late onset following kidney transplantation. In contrast, IgM+-unmutated post-transplant diffuse large B-cell lymphoma arose almost exclusively in hematopoietic stem cell transplant recipients, early following transplantation and was associated with worse outcome. The latter may be biased by the high number of non-post-transplant lymphoproliferative disorder-related deaths, however the IgM+ tumors were associated with a significantly higher proliferation index than IgM− cases indicating they are more aggressive.
Morphologically and immunophenotypically, IgM+ post-transplant diffuse large B-cell lymphoma was associated with a plasma cell phenotype linked with increased unfolded protein response signaling. The mechanisms behind this phenotype are unclear but it could reflect accelerated plasma cell differentiation of an unmutated naive IgM+/IgD+ B-cell activated outside the germinal center. Also in chronic lymphocytic leukemia, the presence or absence of somatic hypermutation distinguishes two clinically distinct forms. Chronic lymphocytic leukemia with unmutated IgV genes is characterized by more aggressive disease and a poorer prognosis than cases with mutated IgV.29 A factor that potentially contributes to the more aggressive clinical course of unmutated cases is (auto)antigenic stimulation of the IgM-type B-cell receptor of tumor cells resulting in induction of tumor-promoting signaling.30, 31, 32 Whether this is also the case for IgM+ post-transplant diffuse large B-cell lymphoma remains to be determined.
Post-transplant lymphoproliferative disorder is classically associated with EBV latency III, however also latency II and I have been reported.6 In this series, the elaborate latency program III was expressed in all IgM+ tumors, whereas also more restricted latency profiles II, I, and 0 were expressed in IgM− cases. This finding points to an interaction between the level of immunosuppression and EBV protein expression. In line with this hypothesis, most abundant EBV lytic replication was detected in IgM+ post-transplant diffuse large B-cell lymphoma.
In this study we did not assess the origin (donor or host) of the post-transplant diffuse large B-cell lymphoma. Interestingly, however, post-transplant lymphoproliferative disorder following hematopoietic stem cell transplantation is most frequently of donor origin, whereas post-transplant lymphoproliferative disorder following solid organ transplantation is usually host-derived.5 The implications of the origin of post-transplant lymphoproliferative disorder are not clear, but in two studies donor-derived post-transplant lymphoproliferative disorder was associated with earlier onset following transplantation and a higher rate of EBV infection compared with host-derived post-transplant lymphoproliferative disorder.33, 34 On the basis of our results we hypothesize that because of the particularly severe immunosuppression in hematopoietic stem cell transplants compared with solid organ transplants, donor-derived EBV+ B cells are the source of uncontrolled lytic replication. Whether this process is a cause of lymphomagenesis or merely a consequence of immunosuppression is not clear at the moment. Most likely, the interaction between both favors lymphomagenesis. Previous studies have demonstrated promising results for prophylactic use of antivirals in transplant recipients.35, 36, 37 In our study, however, the majority of IgM+ EBV+ post-transplant diffuse large B-cell lymphoma arose in patients who received antiviral treatment. A potential explanation is that in moderately immunosuppressed solid organ transplants, but not in hematopoietic stem cell transplants, antivirals may be effective for prophylaxis.
Currently, standard treatment for post-transplant diffuse large B-cell lymphoma is independent of the EBV status of the tumor and consists of chemotherapy (CHOP; cyclophosphamide, doxorubicin, vincristin, and prednisone) frequently combined with anti-CD20 immunotherapy. The discovery of two subgroups with distinct biological features may allow stratification of post-transplant lymphoproliferative disorder patients and more effective treatment with targeted therapies. IgM+ tumors may be sensitive to compounds that increase endoplasmatic reticulum stress, eg, bortezomib.38 As bortezomib was shown to induce EBV lytic replication in vitro39 combination therapy with antivirals could be an attractive treatment approach.
In conclusion, our study allows further molecular classification of post-transplant diffuse large B-cell lymphoma, the most frequent type of monomorphic post-transplant lymphoproliferative disorder, and provides a rationale for the use of treatments that target subtype-specific features. The particular phenotype and gene expression profile of IgM+ tumors provides a biological basis for the clinical differences between post-transplant lymphoproliferative disorder following solid organ transplantation and post-transplant lymphoproliferative disorder following hematopoietic stem cell transplantation, which are regarded as very different disorders.40
The authors acknowledge the potential biases that may have influenced the conclusions of this study, mainly the limited number of cases. Therefore, we encourage other groups to validate our findings in larger series of post-transplant diffuse large B-cell lymphoma.
References
Swerdlow SH CE HN, Jaffe ES, Pileri SA et al, Post-transplant Lymphoproliferative Disorders. WHO Classification of Tumors of Hematologic and Lymphoid Tissue. IARC Press: Lyon, France, 2008, pp 343–349.
Morscio J, Dierickx D, Ferreiro JF et al, Gene expression profiling reveals clear differences between EBV-positive and EBV-negative posttransplant lymphoproliferative disorders. Am J Transplant 2013; 13: 1305–1316.
Richendollar BG, Tsao RE, Elson P et al, Predictors of outcome in post-transplant lymphoproliferative disorder: an evaluation of tumor infiltrating lymphocytes in the context of clinical factors. Leuk Lymphoma 2009; 50: 2005–2012.
Chen BJ, Chapuy B, Ouyang J et al, PD-L1 expression is characteristic of a subset of aggressive B-cell lymphomas and virus-associated malignancies. Clin Cancer Res 2013; 19: 3462–3473.
Kinch A, Baecklund E, Backlin C et al, A population-based study of 135 lymphomas after solid organ transplantation: the role of Epstein-Barr virus, hepatitis C and diffuse large B-cell lymphoma subtype in clinical presentation and survival. Acta Oncol 2014; 53: 669–679.
Vakiani E, Basso K, Klein U et al, Genetic and phenotypic analysis of B-cell post-transplant lymphoproliferative disorders provides insights into disease biology. Hematol Oncol 2008; 26: 199–211.
Craig FE, Johnson LR, Harvey SA et al, Gene expression profiling of Epstein-Barr virus-positive and negative monomorphic B-cell posttransplant lymphoproliferative disorders. Diagn Mol Pathol 2007; 16: 158–168.
Kato H, Karube K, Yamamoto K et al, Gene expression profiling of Epstein-Barr virus-positive diffuse large B-cell lymphoma of the elderly reveals alterations of characteristic oncogenetic pathways. Cancer Sci 2014; 105: 537–544.
Capello D, Rossi D, Gaidano G . Post-transplant lymphoproliferative disorders: molecular basis of disease histogenesis and pathogenesis. Hematol Oncol 2005; 23: 61–67.
Capello D, Cerri M, Muti G et al, Molecular histogenesis of posttransplantation lymphoproliferative disorders. Blood 2003; 102: 3775–3785.
Bräuninger A, Spieker T, Mottok A et al. Epstein-Barr virus (EBV)-positive lymphoproliferations in post-transplant patients show immunoglobulin V gene mutation patterns suggesting interference of EBV with normal B cell differentiation processes. Eur J Immunol 2003; 33: 1593–1602.
Timms JM, Bell A, Flavell JR et al, Target cells of Epstein-Barr-virus (EBV)-positive post-transplant lymphoproliferative disease: similarities to EBV-positive Hodgkin's lymphoma. Lancet 2003; 361: 217–223.
Knight JS, Tsodikov A, Cibrik DM et al. Lymphoma after solid organ transplantation: risk, response to therapy, and survival at a transplantation center. J Clin Oncol 2009; 27: 3354–3362.
Landgren O, Gilbert ES, Rizzo JD et al, Risk factors for lymphoproliferative disorders after allogeneic hematopoietic cell transplantation. Blood 2009; 113: 4992–5001.
Izadi M, Taheri S . Features, predictors and prognosis of lymphoproliferative disorders post-liver transplantation regarding disease presentation time: report from the PTLD.Int. survey. Ann Transplant 2011; 16: 39–47.
Lucas KG, Small TN, Heller G et al. The development of cellular immunity to Epstein-Barr virus after allogeneic bone marrow transplantation. Blood 1996; 87: 2594–2603.
Gonzalez-Farre B, Rovira J, Martinez D et al, In vivo intratumoral Epstein-Barr virus replication is associated with XBP1 activation and early-onset post-transplant lymphoproliferative disorders with prognostic implications. Mod Pathol 2014; 27: 1599–1611.
Hong GK, Gulley ML, Feng WH et al, Epstein-Barr virus lytic infection contributes to lymphoproliferative disease in a SCID mouse model. J Virol 2005; 79: 13993–14003.
Mahot S, Sergeant A, Drouet E et al, A novel function for the Epstein-Barr virus transcription factor EB1/Zta: induction of transcription of the hIL-10 gene. J Gen Virol 2003; 84: 965–974.
Tsai SC, Lin SJ, Chen PW et al, EBV Zta protein induces the expression of interleukin-13, promoting the proliferation of EBV-infected B cells and lymphoblastoid cell lines. Blood 2009; 114: 109–118.
Laichalk LL, Thorley-Lawson DA . Terminal differentiation into plasma cells initiates the replicative cycle of Epstein-Barr virus in vivo. J Virol 2005; 79: 1296–1307.
Taylor GM, Raghuwanshi SK, Rowe DT et al, Endoplasmic reticulum stress causes EBV lytic replication. Blood 2011; 118: 5528–5539.
Hans CP, Weisenburger DD, Greiner TC et al, Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 2004; 103: 275–282.
Giudicelli V, Chaume D, Lefranc MP . IMGT/GENE-DB: a comprehensive database for human and mouse immunoglobulin and T cell receptor genes. Nucleic Acids Res 2005; 33: D256–D261.
Dierickx D, Tousseyn T, Sagaert X et al, Single-center analysis of biopsy-confirmed posttransplant lymphoproliferative disorder: incidence, clinicopathological characteristics and prognostic factors. Leuk Lymphoma 2013; 54: 2433–2440.
Verdonk RC, Haagsma EB, Jonker MR et al, Effects of different immunosuppressive regimens on regulatory T-cells in noninflamed colon of liver transplant recipients. Inflamm Bowel Dis 2007; 13: 703–709.
Chetaille B, Bertucci F, Finetti P et al, Molecular profiling of classical Hodgkin lymphoma tissues uncovers variations in the tumor microenvironment and correlations with EBV infection and outcome. Blood 2009; 113: 2765–3775.
Green MR, Rodig S, Juszczynski P et al, Constitutive AP-1 activity and EBV infection induce PD-L1 in Hodgkin lymphomas and posttransplant lymphoproliferative disorders: implications for targeted therapy. Clin Cancer Res 2012; 18: 1611–1618.
Stevenson FK, Forconi F, Packham G . The meaning and relevance of B-cell receptor structure and function in chronic lymphocytic leukemia. Semin Hematol 2014; 51: 158–167.
Guarini A, Chiaretti S, Tavolaro S et al, BCR ligation induced by IgM stimulation results in gene expression and functional changes only in IgV H unmutated chronic lymphocytic leukemia (CLL) cells. Blood 2008; 112: 782–792.
Chiorazzi N, Rai KR, Ferrarini M . Chronic lymphocytic leukemia. N Engl J Med 2005; 352: 804–815.
Messmer BT, Albesiano E, Efremov DG et al, Multiple distinct sets of stereotyped antigen receptors indicate a role for antigen in promoting chronic lymphocytic leukemia. J Exp Med 2004; 200: 519–525.
Capello D, Rasi S, Oreste P et al, Molecular characterization of post-transplant lymphoproliferative disorders of donor origin occurring in liver transplant recipients. J Pathol 2009; 218: 478–486.
Weissmann DJ, Ferry JA, Harris NL et al, Posttransplantation lymphoproliferative disorders in solid organ recipients are predominantly aggressive tumors of host origin. Am J Clin Pathol 1995; 103: 748–755.
Marty FM, Rubin RH . The prevention of infection post-transplant: the role of prophylaxis, preemptive and empiric therapy. Transpl Int 2006; 19: 2–11.
Funch DP, Walker AM, Schneider G et al, Ganciclovir and acyclovir reduce the risk of post-transplant lymphoproliferative disorder in renal transplant recipients. Am J Transplant 2005; 5: 2894–2900.
Darenkov IA, Marcarelli MA, Basadonna GP et al, Reduced incidence of Epstein-Barr virus-associated posttransplant lymphoproliferative disorder using preemptive antiviral therapy. Transplantation 1997; 64: 848–852.
Camicia R, Winkler HC, Hassa PO . Novel drug targets for personalized precision medicine in relapsed/refractory diffuse large B-cell lymphoma: a comprehensive review. Mol Cancer 2015; 14: 207.
Shirley CM, Chen J, Shamay M et al, Bortezomib induction of C/EBPbeta mediates Epstein-Barr virus lytic activation in Burkitt lymphoma. Blood 2011; 117: 6297–6303.
Loren AW, Porter DL, Stadtmauer EA et al, Post-transplant lymphoproliferative disorder: a review. Bone Marrow Transplant 2003; 31: 145–155.
Acknowledgements
This study was supported by the concerted action grant from the KU Leuven no. 3M040406 (TT and IW) (http://www.kuleuven.be/) and the research grant from FWO-Vlaanderen (G081411N to GV and TT). TT holds a Mandate for Fundamental and Translational Research from the ‘Stichting tegen Kanker’ (2014-083). JM is the recipient of the Yvonne Boël’s Prize 2015 (Boël Foundation).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on Modern Pathology website
Supplementary information
Rights and permissions
About this article

Cite this article
Morscio, J., Finalet Ferreiro, J., Vander Borght, S. et al. Identification of distinct subgroups of EBV-positive post-transplant diffuse large B-cell lymphoma. Mod Pathol 30, 370–381 (2017). https://doi.org/10.1038/modpathol.2016.199
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2016.199
This article is cited by
-
Genomic profiling of post-transplant lymphoproliferative disorders using cell-free DNA
Journal of Hematology & Oncology (2023)
-
Comparative analysis of post-transplant lymphoproliferative disorders after solid organ and hematopoietic stem cell transplantation reveals differences in the tumor microenvironment
Virchows Archiv (2021)
-
The Tumor Microenvironment in Post-Transplant Lymphoproliferative Disorders
Cancer Microenvironment (2019)
-
Targeting the polarization of tumor-associated macrophages and modulating mir-155 expression might be a new approach to treat diffuse large B-cell lymphoma of the elderly
Cancer Immunology, Immunotherapy (2019)
-
Other immunomodulatory agent-related lymphoproliferative diseases: a single-center series of 72 biopsy-confirmed cases
Modern Pathology (2018)
