
Abstract
Submucosally invasive colorectal carcinoma (pT1) has the potential to be cured by local excision. In US surgical intervention is reserved for tumors with high-grade morphology, lymphvascular invasion, and close/positive margin. In other countries, particularly Japan, surgical therapy is also recommended for mucinous tumors, tumors with >1000 μm of submucosal invasion, and those with high tumor budding. These histological features have not been well evaluated in a western cohort of pT1 carcinomas. In a cohort of 116 surgically resected pT1 colorectal carcinomas, high tumor budding (P<0.001), lymphatic invasion (P=0.003), depth of submucosal invasion >1000 μm (P=0.04), and high-grade morphology (P=0.04) were significantly associated with lymph node metastasis on univariate analysis. Mucinous differentiation, tumor location, tumor growth pattern, and size of invasive component were not significant. On multivariate analysis, only high tumor budding was associated with lymph node metastasis with an odds ratio of 4.3 (P=0.004). A subset of 48 tumors (22 node-positive and 26 node-negative) was analyzed for mutations in 50 oncogenes and tumor suppressors. No statistically significant molecular alterations in these 50 genes were associated with lymph node status. However, lymphatic invasion was associated with BRAF mutations (P=0.01). Furthermore, high tumor budding was associated with mutations in TP53 (P=0.03) and inversely associated with mutations in the mTOR pathway (PIK3CA and AKT, P=0.02). In conclusion, this study demonstrates the importance of identifying high tumor budding in pT1 carcinomas when considering additional surgical resection. Molecular alterations associated with adverse histological features are identified.
Similar content being viewed by others


Main
Submucosally invasive colorectal carcinomas usually have an indolent clinical course. For this reason, conservative management with local excision has become an accepted form of therapy. Pathology has a critical role in determining the invasive carcinomas that need additional surgical therapy to prevent either local recurrence or to remove draining lymph nodes to prevent metastatic spread. Well-studied histological features that predict an adverse outcome include polypectomy margin status, grade of tumor, and lymphvascular space invasion.1, 2, 3 More recent studies, particular from Japan, have identified tumor budding, and depth of submucosal invasion as important factors that predict lymph node metastases.4, 5, 6, 7, 8, 9, 10, 11, 12 However, there are limited data on the predictive power of these histological features in a western cohort of pT1 carcinomas. Furthermore, in the era of molecular classification of colorectal carcinoma, little is known about the molecular features of pT1 carcinomas that are associated with adverse histological features and lymph node metastasis.
This study evaluated 116 pT1 carcinomas with and without lymph node metastasis for tumor grade, depth of submucosal invasion, size of invasive component, tumor budding, lymphatic invasion, venous invasion, perineurial invasion, and tumor configuration in attempt to better define features associated with lymph node metastasis. In addition, a subset of 48 carcinomas was evaluated for mutations in 50 oncogenes and tumor suppressors by next-generation sequencing.
Materials and methods
Identification of Study Group Cases
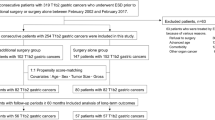
Patients diagnosed with surgically resected colorectal carcinoma with invasion limited to the submucosa (pT1) and with lymph node metastasis accessioned at the Department of Pathology, Cleveland Clinic from 2012 through 2014 and the Department of Pathology, University of Pittsburgh Medical Center from 2010 through 2014 were identified by review of institutional databases under the guidelines of the Cleveland Clinic institutional review board/ethical board (IRB# 11–131) and University of Pittsburgh institutional review board/ethical board (IRB# PR012020335; n=28, 11 from Cleveland Clinic and 17 from University of Pittsburgh Medical Center). A consecutive series of patients diagnosed with surgically resected colorectal carcinoma with invasion limited to the submucosa (pT1) and without lymph node metastasis accessioned at the Department of Pathology, Cleveland Clinic from 2013 through 2014 and the University of Pittsburgh Medical Center, Presbyterian Hospital from 2011 through 2014 were also identified by review of institutional database (n=88, 30 from Cleveland Clinic, 58 from University of Pittsburgh Medical Center). Specifically excluded from the analysis were endoscopically resected pT1 colorectal carcinomas for which lymph node status was unknown and carcinomas treated by neoadjuvant therapy.
Histopathological Analysis
In 108 of the 116 cases the entire tumor was submitted for histological examination. The median number of sections submitted was 4 (range 1–63). All available slides were reviewed. All carcinomas were analyzed for tumor grade and for histological features including depth of submucosal invasion, tumor budding, mucinous differentiation, lymphatic invasion, venous invasion, and perineurial invasion. WHO criteria was used to classify histological grade with low-grade defined as tumors with ⩾50% gland formation and high grade as tumors with <50% gland formation.13 The depth of submucosal invasion was measured using the method proposed by Kawachi et al4 and recommended by the Japanese Society for Cancer of the Colon and Rectum.4, 14 Briefly, each tumor was classified into three categories based on histological review: pedunculated, non-pedunculated with identifiable muscularis mucosae, or non-pedunculated without identifiable muscularis mucosae. For pedunculated tumors, the depth of submucosal invasion was measured in micrometers (μm) starting from the line between the polyp head and stalk (‘Haggitt line’) to the invasive front of the tumor. Tumors with invasion limited to the head of a pedunculated polyp were considered to have submucosal invasion of 0 μm in depth. For non-pedunculated tumors with identifiable muscularis mucosae, submucosal invasion was measured from the bottom of the muscularis mucosae to the invasive front of the tumor. For non-pedunculated tumors without identifiable muscularis mucosae, submucosal invasion was measured from the surface of the tumor to the invasive front of the tumor. To more accurately measure the depth of invasion, a photograph was taken of the deepest point of invasion and the depth was measured digitally (cellSens standard, Olympus). Tumor budding was assessed using the method advocated by Japanese Society for the Cancer of the Colon and Rectum.4, 14 Tumor buds were defined as isolated cancer cells or a cluster of <5 neoplastic cells at the invasive front of the tumor. The tumor invasive front was assessed at a scanning (× 10 objective) magnification for the area with maximal tumor budding. In this area, the number of tumor buds was determined at the invasive front by counting the number of tumor buds in one × 20 objective field using a × 10/22 ocular (0.95 mm2). A subset of Cleveland Clinic cases were evaluated using a wide-field ocular (× 10/26.5) and the tumor bud count was multiplied by a correction factor of 0.7 to obtain the number of tumor buds per 0.95 mm2. Tumors were classified as having low tumor budding if 0 to 4 tumor buds were identified per 0.95 mm2 and high tumor budding if ⩾5 tumor buds were identified per 0.95 mm2.4, 14 The presence or absence of precursor polyps and the histological subtype of precursor polyps associated with invasive adenocarcinoma were recorded.13, 15
Next-Generation Sequencing Analysis
Genomic DNA (gDNA) extracted from formalin-fixed paraffin-embedded tissue were used for the study. Briefly, 10 ng gDNA was PCR amplified using the Ion AmpliSeq Cancer Hotspot Panel v2 (CHPv2) and the Ion AmpliSeq Library Kit 2.0 (ThermoFisher Scientific, Waltham, MA, USA). The CHPv2 targets ~2800 hotspot variants in 50 oncogenes and tumor-suppressor genes, including ABL1, AKT1, ALK, APC, ATM, BRAF, CDH1, CDKN2A, CSF1R, CTNNB1, EGFR, ERBB2, ERBB4, EZH2, FBXW7, FGFR1, FGFR2, FGFR3, FLT3, GNA11, GNAS, GNAQ, HNF1A, HRAS, IDH1, IDH2, JAK2, JAK3, KDR, KIT, KRAS, MET, MLH1, MPL, NOTCH1, NPM1, NRAS, PDGRFA, PIK3CA, PTEN, PTPN11, RB1, RET, SMAD4, SMARCB1, SMO, SRC, STK11, TP53, and VHL.
After initial amplification, barcode adapters are ligated onto each amplicon to enable multiplexing and the subsequent massive parallel sequencing. The prepared sequencing libraries were visualized and quantified using the Bioanalyzer 2100 (Agilent Technologies, Santa Clara, CA, USA), and were normalized, pooled, denatured, and sequenced on MiSeq (Illumina, San Diego, CA, USA). The resulted fastq files were aligned and analyzed using NextGENe (SoftGenetics, State College, PA, USA) bioinformatics tool. Only those variants, excluding common SNPs (single-nucleotide polymorphisms), residing in defined mutation hotspots with over 5% allele frequency were examined and scored in the study.
Microsatellite Instability PCR and Mismatch-Repair Protein Immunohistochemistry
For all patients, colorectal carcinomas were prospectively analyzed for MMR protein abnormalities using a combination of microsatellite instability (MSI) PCR and MMR protein immunohistochemistry as part of routine pathological evaluation. Cases identified at Cleveland Clinic were analyzed using the ProMega MSI analysis system utilizing a panel of five mononucleotide microsatellite markers (BAT-25, BAT-26, NR-21, NR-24, and MONO-27) and two pentanucleotide repeats (Penta C and Penta D) incorporated into a multiplex fluorescence assay, as previously described.16 Detection of MSI for cases identified at the University of Pittsburgh was performed using a National Cancer Institute-recommended panel of microsatellite markers (BAT-25, BAT-26, D2S123, D5S346, and D17S250) as well as one novel quasi-monomorphic mononucleotide marker CAT25.17 On the basis of established criteria, if 0 markers show instability, the tumor is classified as microsatellite stable (MSS). If ⩾30% of the markers showed instability by PCR, the tumor is classified as high-level MSI (MSI-H).
MMR protein immunohistochemistry was performed using primary monoclonal antibodies against MLH1 (clone G168-728, Ventana), MSH2 (clone G219-1129, Ventana), MSH6 (clone 44, BD Transduction, San Jose, CA, USA), and PMS2 (EPR3947, Cell Marque, Rocklin, CA, USA). The sections were deparaffinized in xylene, and rehydrated through graded alcohols to distilled water before undergoing antigen retrieval by heat treatment using either Ventana CC1 buffer solution (MSH2 and MSH6) or Ventana CC2 buffer solution (MLH1 and PMS2). Automated detection using the Ventana Benchmark Ultra staining system and Ventana UltraView detection was used. Normal preserved expression was defined as nuclear staining within tumor cells, using infiltrating lymphocytes as positive internal control. Loss of protein expression was defined as complete absence of nuclear staining within tumor cells with concurrent positive labeling in internal non-neoplastic tissues.
Tumors with loss of expression of any MMR protein or with MSI-H by PCR were labeled as MMR protein deficient (MMRD). Tumors with preserved expression of all four MMR proteins and/or MSS by PCR analysis were labeled as MMR protein proficient (MMRP).
Statistical Analysis
χ2-Test or Fisher’s exact test was used to characterize the relationship between categorical variables, as appropriate. Disease-specific survival and time to disease recurrence were the primary endpoints. Disease-specific survival was defined as the time (measured in months) from the date of initial diagnosis to the date of death from disease and censored at the date of last clinical follow-up. Time to disease recurrence was defined as the time (measured in months) from the date of initial diagnosis to the date of first tumor recurrence and censored at the date of last clinical follow-up. Survival rates were determined by the Kaplan–Meier method and differences between groups were evaluated by log-rank test. Statistical analyses were performed using SPSS (for Windows 12.0, SPSS, Chicago, IL, USA).
Results
Clinicopathological Features of pT1 Colorectal Carcinomas: High Tumor Budding and Lymphatic Invasion Are Associated with Lymph Node Metastasis
Of a total of 3330 surgically resected colorectal carcinomas, 28 (0.8%) pT1 colorectal carcinomas with lymph node metastasis (lymph node-positive) were identified. For comparison 88 consecutively surgically resected pT1 colorectal carcinomas without lymph node metastasis (lymph node-negative) were identified from 921 colorectal carcinomas (88/921, 9.6%).
Table 1 details the clinicopathological features of pT1 colorectal carcinomas stratified by lymph node status. There was no difference between mean number of lymph nodes examined in patients with lymph node-negative tumors (mean 23 lymph nodes, range 5–64 lymph nodes) and patients with lymph node-positive tumors (mean 23 lymph nodes, range 6–48 lymph nodes; P=0.9). Of the 28 patients with lymph node-positive tumors, 89% (25/28) had between 1 and 3 lymph nodes with metastatic adenocarcinoma with most (17/25, 68%) having only 1 lymph node involved by metastatic adenocarcinoma. Most pT1 tumors (84/116, 72%) had a non-pedunculated tumor configuration with no difference between lymph node-negative and lymph node-positive tumors (P=0.4).
Histopathological examination demonstrated significant differences between lymph node-negative and lymph node-positive tumors (Figure 1). Lymph node-positive tumors more often displayed high tumor budding compared with lymph node-negative tumors (57 vs 19%, P<0.001). Lymphatic invasion was also identified more frequently in lymph node-positive tumors compared with lymph node-negative tumors (39 vs 14%, P=0.003). Lymph node-positive tumors demonstrated a higher mean depth of submucosal invasion (mean 3053 μm) compared with lymph node-negative tumors (mean 2005 μm; P=0.04). Using the 1000 μm cut-point for depth of submucosal invasion advocated by Kawachi et al4 and the Japanese Society for Cancer of the Colon and Rectum5, lymph node-positive tumors more frequently had a depth of submucosal invasion >1000 μm compared with lymph node-negative tumors (81 vs 60%, P=0.04). Notably, all three pN2 tumors had high tumor budding, lymphatic invasion, and ⩾1000 μm submucosal invasion; however, statistical comparison between pN1 and pN2 could not be performed due to the relatively small number of cases. There were no significant differences with respect to patient age, gender, tumor location, mucinous differentiation, venous invasion, perineurial invasion, or precursor polyp between lymph node-negative and lymph node-positive tumors (all with P>0.05).

Histological features of pT1 carcinomas associated with lymph node metastasis. (a) A low-grade adenocarcinoma invasive into submucosal to a depth of 1810 μm. No muscularis mucosae was visualized and the depth of invasion was measured from the surface to the deepest extent of invasion. (b) Lymphatic invasion in a high-grade adenocarcinoma with positive lymph nodes. (c) High tumor budding with numerous clusters of <5 tumor cells at the invasive front.
In addition, logistic regression analysis was performed to correlate the risk of lymph node metastasis with the number of adverse histological risk factors (Table 2). The risk of lymph node metastasis increased substantially with the number of adverse histological risk factors. Of the 14 tumors with ⩾3 histological risk factors, 9 (64%) had lymph node metastasis (odds ratio 49, P=0.001).
Multivariable Analysis of Histopathological Factors Predictive of Lymph Node Metastasis in pT1 Colorectal Carcinoma
Multivariable logistic regression analysis was performed using histopathological factors that were significantly correlated with lymph node metastasis (Table 3). Only tumor budding was independently and significantly associated with lymph node metastasis in the multivariable model (P=0.004). Tumor grade, depth of submucosal invasion, and lymphatic invasion were not independent predictors of lymph node metastasis (all with P>0.05).
Correlation of Molecular Findings and Clinicopathological Features: High Tumor Budding is Associated with TP53 Mutations and Lack of mTOR Pathway Mutations
In all, 48 cases (22 lymph node-positive and 26 lymph node-negative cases) were analyzed by next-generation sequencing using the AmpliSeq Cancer Hotspot panel (v2) for targeted multi-gene amplification (Table 4). All 48 tumors demonstrated at least 1 mutation with the following distribution: 11 tumors with 1 mutation, 12 tumors with 2 mutations, 15 tumors with 3 mutations, 7 tumors with 4 mutations, and 3 tumors with 5 mutations.
Mutations in the WNT signaling pathway were identified in 60% (29 of 48) of tumors with all 29 cases harboring an APC mutation and 1 case with a mutation both in CTNNB1 and APC. Mutations in the MAPK pathway were identified in 67% (32 of 48) of tumors including KRAS (20 cases, 42%), NRAS (4 cases, 8%), and BRAF (8 cases, 17%). Of the 24 RAS mutations, 15 were in codon 12, three in codon 13, four in codon 61, and two in codon 146. All 8 BRAF mutations were c.1799T>A, p.V600E. KRAS, NRAS, and BRAF mutations were mutually exclusive. TP53 point mutations were identified in 56% (27 of 48) of tumors with 23 tumors harboring a single point mutation and 4 tumors harboring two point mutations. Mutations in the mTOR pathway were seen in 19% (9 of 48) of tumors including eight cases with PIK3CA mutations and one case with AKT mutation. No PTEN mutations were identified. Three tumors had CDKN2A mutations, two tumors had GNAS mutations, and one tumor each had a SMAD4, FGFR3, RET, SMARCB1/c, FBXW7, JAK3, and STK11 mutation. Analysis by either MMR protein immunohistochemistry or MSI PCR was performed in 103 cases, and most cases were MMRP (82/103, 80%). Of the 21 MMRD tumors, 8 tumors had loss of MLH1 and PMS2 expression with concurrent BRAF V600E mutation, 5 tumors had loss of MLH1 and PMS2 expression with concurrent wild-type BRAF, and 7 tumors had loss of MSH2 and MSH6 expression, and 1 tumor had isolated loss of PMS2 expression.
There were no significant differences in molecular mutations or MMR protein/MSI status between lymph node-negative and lymph node-positive tumors. The molecular findings were also correlated with tumor budding given the findings of the multivariable model demonstrating that tumor budding was the only independent predictor of lymph node metastasis (Table 3). TP53 mutations were more often identified in tumors with high tumor budding compared with tumors with low tumor budding (73 vs 42%, P=0.03). In addition, mTOR pathway mutations were less often identified in tumors with high tumor budding compared with tumors with low tumor budding (5 vs 31%, P=0.02). Of note, all three pN2 tumors had TP53 mutations, whereas none had mTOR pathway mutations. BRAF mutations were also associated with lymphatic invasion (P=0.01) and all 3 BRAF-mutated MMRP had lymphatic invasion in contrast to 2 of 5 BRAF-mutated MMRD tumors.
Clinical Outcome
Of the 116 patients analyzed, 112 patients had clinical follow-up. Three patients with node-negative tumors died of post-operative complications within 1 month of surgical resection and were excluded from the analysis. A total of 109 patients were included in the survival analysis, including 85 patients with node-negative tumors and 24 patients with node-positive tumors (median follow-up 34 months, range 1–65 months). In the entire cohort, there were 4 patients who developed tumor recurrence (all with liver metastasis) occurring between 8 months and 49 months from the time of initial diagnosis and 3 deaths from disease occurring between 9 months and 52 months from the time of initial diagnosis. Using Kaplan–Meier survival functions, patients with node-positive tumors had a significantly shorter time to disease recurrence compared with patients with node-negative tumors (P=0.02). A trend to decreased disease-specific survival for patients with node-positive tumors compared with patients with node-negative tumors was identified, although this did not reach statistical significance (P=0.07). There was no difference in time to recurrence or disease-specific survival with respect to tumor budding, depth of submucosal invasion, lymphatic invasion, TP53 mutation, MAPK mutation, WNT pathway mutation, or mTOR pathway mutation (all with P>0.05).
Discussion
Local control of minimally invasive colorectal carcinoma, both non-pedunculated and pedunculated lesions, is gaining acceptance, particularly with the development of advanced endoscopic techniques such as endoscopic submucosal dissection. In the US, the accepted criteria for surgical therapy after endoscopic removal of submucosal invasive carcinoma (pT1) include tumors with positive or close margins, poor differentiation, and vascular invasion.1, 18 However, there have been studies from Japan addressing additional histological criteria that is predictive of lymph node metastasis in this setting.4, 5, 6, 7, 8, 9, 10, 11, 12 According to the 2014 guidelines from the Japanese Society for Cancer of the Colon and Rectum, the presence of one of the following histological features warrants surgical therapy after endoscopic resection: depth of submucosal invasion (⩾1000 μm), positive vascular invasion, poorly differentiated carcinoma, signet ring cell carcinoma, mucinous carcinoma, positive resection margin, and high tumor budding at the invasive front.14 Although these features have been well studied in Asian populations, the current study is the first to our knowledge to evaluate these histological features in a cohort of patients with pT1 tumors in US.
Our cohort of pT1 colorectal carcinomas with lymph node metastasis had deeper submucosal invasion, high tumor grade, high tumor budding, and higher frequency of lymphatic invasion. Univariate analysis showed significant associations between lymphatic invasion, high tumor budding, high tumor grade, and depth of submucosal invasion and the presence of lymph node metastasis. The number of adverse histological features also correlated strongly with the risk of lymph node metastasis in this group. However, multivariate analysis demonstrated tumor budding as the only independent predictor of lymph node metastasis with an odds ratio of 4.3 (P=0.004).
Lymphatic invasion has been a well-studied histological feature predictive of lymph node metastasis. In a meta-analysis of 1438 polyps, vascular invasion was identified in 17.6% of polyps and was more common in lymph node-positive vs lymph node-negative cases (35.3 vs 7.2%) consistent with our findings.18 These results underscore the importance of careful assessment of endoscopically resected pT1 cancers for the presence of lymphatic invasion in order to guide subsequent therapy. However, lymphatic invasion has been reported with variable frequencies in submucosally invasive carcinomas and some studies have failed to demonstrate the predictive power of lymphatic invasion in this setting.19 Furthermore, lymphatic invasion can be difficult to identify with certainty and suffers from only fair interobserver agreement.20
Depth of submucosal invasion has been shown in multiple studies from Asia as predictive of lymph node metastasis.4, 5, 6, 7, 8, 9, 10, 11, 12, 21 Ueno et al8 demonstrated that no tumors with <500 μm and only 3.9% of tumors with a depth of 2000 μm had lymph node metastasis. More recently others have demonstrated that tumors <1000 μm have a low-risk of lymph node metastasis. Table 5 summarizes the major studies that evaluate depth of invasion, lymphatic invasion, and tumor budding in pT1 colorectal carcinomas. Our cohort had a similar percentage of pT1 tumors with depth of invasion ⩾1000 μm compared with these other studies (Table 5). Our study confirms that submucosal invasion ⩾1000 μm is significantly associated with more frequent lymph node metastasis; however, this features was not an independent predictor of lymph node metastasis in our multivariable model. Depth of submucosal invasion may also have limited clinical utility given that >60% of pT1 tumors without lymph node metastasis have invaded ⩾1000 μm across multiple studies. Indeed, this feature was not significant or borderline significant in some studies (Table 5).
Tumor budding, defined as clusters of ⩽5 tumor cells at the invasive front, has been shown to be strongly associated with lymph node metastasis across all stages of colorectal carcinoma.22, 23, 24, 25, 26 In 2004, Ueno et al8 demonstrated the utility of tumor budding in predicting lymph node in pT1 carcinomas and other groups have confirmed these findings (Table 5). Our study found a statistically significant association between high tumor budding and lymph node metastasis, and identified high tumor budding as the only independent predictor of lymph node metastasis. Assessment of tumor budding is not routinely performed in most institutions in US and is not part of the College of American Pathologists synoptic template commonly used by most institutions. Our findings, along with previous literature reports, indicate the histological evaluation of tumor budding should be performed when risk-stratifying patients with endoscopically resected pT1 colorectal carcinomas.
Molecular analysis of colorectal carcinoma has identified multiple molecular subtypes of carcinoma that are predictive of both response to therapy and clinical outcome.27, 28, 29, 30 In order to determine if pT1 colorectal carcinomas can be classified molecularly into high-risk and low-risk groups, we performed next-generation sequencing of a subset of tumors (22 lymph node-positive and 26 lymph node-negative cases) using the AmpliSeq Cancer Hotspot panel (v2) platform which is designed to detect ~2800 mutations in 50 oncogenes and tumor suppressors. Although no significant molecular differences were identified between lymph node-positive and lymph node-negative pT1 carcinomas there were some interesting molecular differences based on histological features.
High tumor budding was associated with the presence of mutations in TP53 (73 vs 42%, P=0.03) and absence of mutations in the mTOR pathway (5 vs 31%, P=0.02). A few prior studies have analyzed the molecular features associated with tumor budding and demonstrated mutations in the WNT and MAPK pathways were associated with high tumor budding whereas MMRD phenotype is associated with decreased tumor budding.24, 31, 32 Our findings demonstrated no associations with these pathways. TP53 regulates epithelial-to-mesenchymal transition and given that tumor budding is presumed to result from epithelial to mesenchymal transition, it is not surprising that we found an association between high tumor budding and TP53.33, 34 The inverse relationship between mutations in the PI3K/AKT/mTOR pathway and high tumor budding is also a new finding of this study. mTOR activation in normal cells results in exit from the cell cycle and senescence.35, 36 However, in transformed cell, particularly those with mutations in TP53, mTOR activation promotes cell growth.37, 38, 39 Interestingly, in our study, only one of eight tumors with a PI3KCA mutation had a concurrent mutation in TP53, and this tumor with concurrent PIK3CA and TP53 mutations demonstrated high tumor budding. The role of the mTOR pathway in tumor budding deserves additional study.
In conclusion, this study is the first to apply the criteria recommended by the Japanese Society for Cancer of the Colon and Rectum to a US cohort of pT1 carcinomas. These results confirm the importance of tumor budding, depth of submucosal invasion, and lymphatic invasion in predicting lymph node metastasis. Tumor budding was the best predictor of lymph node metastasis in our cohort. Although molecular analysis did not identify a statistically significant difference between pT1 carcinomas with and without lymph node metastasis, specific molecular associations were seen with regards to tumor budding and lymphatic invasion.
References
Robert ME . The malignant colon polyp: diagnosis and therapeutic recommendations. Clin Gastroenterol Gepatol 2007; 5: 662–667.
Butte JM, Tang P, Gonen M et al, Rate of residual disease after complete endoscopic resection of malignant colonic polyp. Dis Colon Rectum 2012; 55: 122–127.
Cooper HS, Deppisch LM, Gourley WK et al, Endoscopically removed malignant colorectal polyps: clinicopathologic correlations. Gastroenterology 1995; 108: 1657–1665.
Kawachi H, Eishi Y, Ueno H et al, A three-tier classification system based on the depth of submucosal invasion and budding/sprouting can improve the treatment strategy for T1 colorectal cancer: a retrospective multicenter study. Mod Pathol 2015; 28: 872–879.
Egashira Y, Yoshida T, Hirata I et al, Analysis of pathological risk factors for lymph node metastasis of submucosal invasive colon cancer. Mod Pathol 2004; 17: 503–511.
Tominaga K, Nakanishi Y, Nimura S et al, Predictive histopathologic factors for lymph node metastasis in patients with nonpedunculated submucosal invasive colorectal carcinoma. Dis Colon Rectum 2005; 48: 92–100.
Oka S, Tanaka S, Nakadoi K, Kanao H, Chayama K . Risk analysis of submucosal invasive rectal carcinomas for lymph node metastasis to expand indication criteria for endoscopic resection. Dig Endosc 2013; 25 (Suppl 2), 21–25.
Ueno H, Mochizuki H, Hashiguchi Y et al, Risk factors for an adverse outcome in early invasive colorectal carcinoma. Gastroenterology 2004; 127: 385–394.
Nakadoi K, Tanaka S, Kanao H et al, Management of T1 colorectal carcinoma with special reference to criteria for curative endoscopic resection. J Gastroenterol Hepatol 2012; 27: 1057–1062.
Saitoh Y, Inaba Y, Sasaki T et al, Management of colorectal T1 carcinoma treated by endoscopic resection. Dig Endosc 2016; 28: 324–329.
Tateishi Y, Nakanishi Y, Taniguchi H, Shimoda T, Umemura S . Pathological prognostic factors predicting lymph node metastasis in submucosal invasive (T1) colorectal carcinoma. Mod Pathol 2010; 23: 1068–1072.
Ueno H, Hase K, Hashiguchi Y et al, Novel risk factors for lymph node metastasis in early invasive colorectal cancer: a multi-institution pathology review. J Gastroenterol 2014; 49: 1314–1323.
Hamilton SR, Bosman FT, Boffetta P et al, Carcinoma of the colon and rectum. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. WHO Classification of Tumors of the Digestive System, 4th edn. IARC Press: Lyon, France, 2010; 143–146.
Watanabe T, Itabashi M, Shimada Y et al, Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines 2014 for treatment of colorectal cancer. Int J Clin Oncol 2015; 20: 207–239.
Snover DC, Ahnen DJ, Burt RW et al, Serrated polyps of the colon and rectum and serrated polyposis. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. WHO Classification of Tumors of the Digestive System, 4th edn. IARC Press: Lyon, France, 2010; 160–165.
Suraweera N, Duval A, Reperant M et al, Evaluation of tumor microsatellite instability using five quasimonomorphic mononucleotide repeats and pentaplex PCR. Gastroenterology 2002; 123: 1804–1811.
Bianchi F, Galizia E, Catalani R et al, CAT25 is a mononucleotide marker to identify HNPCC patients. J Mol Diagn 2009; 11: 248–252.
Hassan C, Zullo A, Risio M et al, Histologic risk factors and clinical outcome in colorectal malignant polyp: a pooled-data analysis. Dis Colon Rectum 2005; 48: 1588–1596.
Volk EE, Goldblum JR, Petras RE et al, Management and outcome of patients with invasive carcinoma arising in colorectal polyps. Gastroenterology 1995; 109: 1801–1807.
Harris EI, Lewin DN, Wang HL et al, Lymphovascular invasion in colorectal cancer: an interobserver variability study. Am J Surg Pathol 2008; 32: 1816–1821.
Kitajima K, Fujimori T, Fujii S et al, Correlations between lymph node metastasis and depth of submucosal invasion in submucosal invasive colorectal carcinoma: a Japanese collaborative study. J Gastroenterol 2004; 39: 534–543.
Barresi V, Bonetti LR, Ieni A et al, Histologic grading based on counting poorly differentiated clusters in preoperative biopsy predicts nodal involvement and pTNM stage in colorectal cancer patients. Hum Pathol 2014; 45: 268–275.
Betge J, Kornprat P, Pollheimer MJ et al, Tumor budding is an independent predictor of outcome in AJCC/UICC stage II colorectal cancer. Ann Surg Oncol 2012; 19: 3706–3712.
Graham RP, Vierkant RA, Tillmans LS et al, Tumor budding in colorectal carcinoma: confirmation of prognostic significance and histologic cutoff in a population-based cohort. Am J Surg Pathol 2015; 39: 1340–1346.
Mitrovic B, Schaeffer DF, Riddell RH et al, Tumor budding in colorectal carcinoma: time to take notice. Mod Pathol 2012; 25: 1315–1325.
Koelzer VH, Zlobec I, Lugli A . Tumor budding in colorectal cancer—ready for diagnostic practice? Hum Pathol 2016; 47: 4–19.
Phipps AI, Limburg PJ, Baron JA et al, Association between molecular subtypes of colorectal cancer and patient survival. Gastroenterology 2015; 148: 77–87.
Sinicrope FA, Shi Q, Smyrk TC et al, Molecular markers identify subtypes of stage III colon cancer associated with patient outcomes. Gastroenterology 2015; 148: 88–99.
Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012; 487: 330–337.
Sadanandam A, Lyssiotis CA, Homicsko K et al, A colorectal cancer classification system that associates cellular phenotype and responses to therapy. Nat Med 2013; 19: 619–625.
Prall F, Weirich V, Ostwald C . Phenotypes of invasion in sporadic colorectal carcinomas related to aberrations of the adenomatous polyposis coli (APC) gene. Histopathology 2007; 50: 318–330.
Jass JR, Barker M, Fraser L et al, APC mutation and tumour budding in colorectal cancer. J Clin Pathol 2003; 56: 69–73.
Araki K, Ebata T, Guo AK et al, p53 regulates cytoskeleton remodeling to suppress tumor progression. Cell Mol Life Sci 2015; 72: 4077–4094.
Puisieux A, Brabletz T, Caramel J . Oncogenic roles of EMT-inducing transcription factors. Nat Cell Biol 2014; 16: 488–494.
Huang K, Fingar DC . Growing knowledge of the mTOR signaling network. Semin Cell Dev Biol 2014; 36: 79–90.
Leontieva OV, Gudkov AV, Blagosklonny MV . Weak p53 permits senescence during cell cycle arrest. Cell Cycle 2010; 9: 4323–4327.
Feng Z, Hu W, Rajagopal G, Levine AJ . The tumor suppressor p53: cancer and aging. Cell Cycle 2008; 7: 842–847.
Feng Z, Zhang H, Levine AJ et al, The coordinate regulation of the p53 and mTOR pathways in cells. Proc Natl Acad Sci USA 2005; 102: 8204–8209.
Akeno N, Miller AL, Ma X et al, p53 suppresses carcinoma progression by inhibiting mTOR pathway activation. Oncogene 2015; 34: 589–599.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Pai, R., Chen, Y., Jakubowski, M. et al. Colorectal carcinomas with submucosal invasion (pT1): analysis of histopathological and molecular factors predicting lymph node metastasis. Mod Pathol 30, 113–122 (2017). https://doi.org/10.1038/modpathol.2016.166
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2016.166
This article is cited by
-
A proposal for grading the risk of lymph node metastasis after endoscopic resection of T1 colorectal cancer
International Journal of Colorectal Disease (2023)
-
Tumor budding as a predictive marker for 5-fluorouracil response in adjuvant-treated stage III colorectal cancer
International Journal of Clinical Oncology (2021)
-
Discohesive growth pattern (Disco-p) as an unfavorable prognostic factor in lung adenocarcinoma: an analysis of 1062 Japanese patients with resected lung adenocarcinoma
Modern Pathology (2020)
-
Re-examining the 1-mm margin and submucosal depth of invasion: a review of 216 malignant colorectal polyps
Virchows Archiv (2020)
-
Tumor budding is an adverse prognostic marker in intestinal-type sinonasal adenocarcinoma and seems to be unrelated to epithelial-mesenchymal transition
Virchows Archiv (2020)
