
Abstract
Diagnosis of Hirschsprung disease (HD) is quite entirely based on the histopathological analysis of suction rectal biopsies. This hematoxylin and eosin approach has some limitations, despite the help of acetylcholinesterase staining. The aim of this study was to assess the diagnostic value of calretinin immunochemistry as a simple and reliable method in the diagnosis of HD. A total of 131 initial rectal biopsies carried out for suspicion of HD in children were retrieved, and calretinin immunohistochemistry was carried out on paraffin-embedded biopsies. Diagnosis of HD was made when no staining was observed. The results were statistically analyzed in comparison with our standard method (histology and acetylcholinesterase staining). 130 biopsies were accurately diagnosed on the basis of the positivity or negativity of calretinin staining. The senior pathologists diagnosed all cases of HD with no false positives. Furthermore, 12 additional cases initially considered as doubtful for HD using the standard method, were accurately diagnosed using calretinin immunohistochemistry. The false negative was a case of HD with a calretinin-positive biopsy. We also demonstrate the ease of calretinin interpretation compared with acetylcholinesterase for the junior pathologist. Calretinin immunohistochemistry overcomes most of the difficulties encountered using the combination of histology and acetylcholinesterase staining, and detects almost all cases of HD with confidence, with no false positives. Thus, we demonstrate that calretinin is superior to acetylcholinesterase to complete histology and could advantageously substitute for acetylcholinesterase.
Similar content being viewed by others

Main
The diagnosis of Hirschsprung disease (HD) is based on a combination of clinical features, radiological appearance of the bowel and histological features on suction rectal biopsies, 1 ,2 that is, aganglionosis and abnormally large nerves. In practice, a definite diagnosis of HD, leading to surgical treatment, is quite entirely based on histological results.3, 4 Several efficient approaches have been devised to assess the diagnosis of HD using a combination of standard histology and histochemistry. Standard histology obtained from rectal suction biopsies that sample mucosa and underlying submucosa, demonstrating rectal aganglionosis, requires the analysis of 100 or more histological sections to ensure good specificity, and is therefore time consuming. Moreover, difficulties in analysis may arise in several situations: (1) when the site of biopsy is too distal, because of the physiological paucity of ganglion cells; (2) when the sample is too superficial with not enough submucosa; and (3) when there is difficulty in identifying ganglion cells with confidence, particularly in neonates.
For these reasons, standard histology is frequently supplemented with acetylcholinesterase histochemistry. 5, 6 This technique, showing staining of extrinsic nerve fibers, provides quick results but requires frozen tissue samples. The last reports show good specificity of an abnormal acetylcholinesterase staining (up to 100%) but insufficient sensibility (as low as 85%). 7, 8, 9, 10 Variability in cholinergic innervation may contribute to false-negative evaluations for HD and, less frequently, to false positives. False-negative results are primarily related to the young age of patients, 8 to short or long segments of aganglionosis 11, 12, 13 and to HD associated with Down's syndrome. 7 Furthermore, besides typical abnormal staining, several subtle abnormal patterns of acetylcholinesterase staining have been described. 10 Thus, acetylcholinesterase staining can be difficult to carry out and interpret even for pathologists experienced in diagnosing HD. In practice, these difficulties may lead to sequential rectal biopsies and delay in surgical treatment.
Several immunohistochemical markers such as S-100 protein, neurone-specific enolase 14 or glial fibrillar acid 15 have been tried in the past years, but none have been demonstrated to be superior to acetylcholinesterase. Calretinin is a vitamin D-dependent calcium-binding protein involved in calcium signaling, which has an important role in the organization and functioning of the central nervous system. 16 In 2004, Barshack et al 17 showed that the absence of calretinin expression in nerve fibers was correlated to aganglionosis in 10 excision colon samples from patients with HD. Recently, Kapur et al 18 assessed the diagnostic value of calretinin immunohistochemistry in HD on a small series of rectal biopsies showing promising results. Calretinin immunohistochemistry holds several advantages, such as: it is carried out on a formol-embedded superficial rectal biopsy and its staining pattern is simple and not doubtful; and it is either positive or negative.
In this work, we evaluated the value of calretinin immunostaining as a primary diagnostic tool on a large series of suction rectal biopsies. We retrieved 131 biopsies carried out for suspicion of HD in children and infants to compare the accuracy of a new simplified diagnosis technique based on primary calretinin staining analysis in comparison with the standard method (histology and acetylcholinesterase staining).
Materials and methods
For this retrospective study, 131 initial suction rectal biopsies carried out for suspicion of HD were selected from the pathology repository at Robert Debré's hospital over a period of 15 years. The gold standard by which the test was measured was either resection in affected patients (n=54) or follow-up in unaffected patients (n=77).
As the standard method in our laboratory for all suspected cases of HD, rectal biopsy was evaluated for acetylcholinesterase activity on frozen sections and at least four hematoxylin and eosin sections (1–5-15–20) were analyzed on paraffin-embedded sections to screen for the presence or absence of ganglion cells. Additional hematein–eosin sections were requested if no ganglion cell was found.
Only results obtained with this standard method at the actual time of the first biopsy were used for this study.
Acetylcholinesterase Histochemistry
Frozen samples were cut at a microtome setting at 7 μm on poly-L-Lysin slides and the acetylcholinesterase method of Lake was performed as previously described. 19
Calretinin Immunohistochemisty
Paraffin wax-embedded, 4 μm-thick sections of rectal biopsy for each patient were thaw mounted on to Fisherbrand Super Frost, Menzel Gmbh, Braunschweig, Germany and anonymized. Immunohistochemistry was carried out using a monoclonal mouse antibody (Calret 1, Dako, Glostrup, Denmark) at a dilution of 1:100. After a 30 min incubation, unmasking was carried out in a pH 9 buffer heated up to 120°C. Pure Envision dual link (Dako) was then applied for 30 min. Negative control involved the omission of primary antibody and positive control was a juvenile cystic granulosa cell tumor of the testis.
Immunohistochemistry Analysis
Calretinin staining was analyzed without knowledge of the diagnosis. This analysis was independently performed by two pathologists experienced in diagnosing HD (DB and MP) and by a pathologist who was unaccustomed to handling HD cases (VGS). Calretinin was considered as positive if any specific staining (excluding mast cells staining) was present either within the submucosae's nerve plexus, or in the muscularis mucosae or in the lamina propria. On the basis of results of the calretinin immunohistochemistry, an algorithm was constructed and patients were classified as having HD or non-HD. Results were compared with our gold standard and to the initial diagnosis made on the first rectal biopsy using our standard method as detailed in Table 1. The pathologist who was unaccustomed to HD also retrospectively analyzed acetylcholinesterase activity.
Statistical Analysis
We used Cohen's κ coefficient 20 to assess the agreement between the tested technique and the gold standard and between the analysis carried out by pathologists experienced in diagnosing HD and that by the pathologist unaccustomed to diagnosing HD.
Results
Patients
The patients were aged from 3 days–9 years (mean 1.3 years) and there were 61 females and 70 males. The diagnosis based on our standard method was typical HD in 42 cases, non-HD in 73 cases and suspicious for HD in 16 cases (Table 2). In the suspicious cases, no ganglionic cells were found, neither was nerve hypertrophy nor a normal acetylcholinesterase pattern observed.
Calretinin Expression
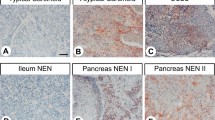
As expected, calretinin immunohistochemistry gave two main results: a total absence of staining (Figure 1a) and a positive staining. Positive staining of nerves was present in submucosae, in muscularis mucosae and frequently in the lamina propria (Figures 1b and c). In the submucosal nerve plexus, a strong nuclear staining was present, highlighting the ganglion cells usually accompanied by a positivity of Schwann cells (Figure 1d). In one case, only focally weak staining was observed in some large submucosal nerve fibers without any staining elsewhere (Figure 1e).

(a): Rectal suction biopsy for suspicion of Hirschsprung disease (HD) showing a total absence of staining after calretinin immunohistochemistry either in submucosae, muscularis mucosae or lamina propria. Insert shows an unstained abnormally large nerve fiber. Original magnification × 400 and × 600 (insert). This pattern diagnosis HD. (b, c and d): Calretinin immunohistochemistry on a rectal suction biopsy for suspicion of HD shown in (b) and (c), positive staining easily detectable at low magnification in submucosae (in b, × 250), in muscularis mucosae (in c, × 400) or sometimes extended to the lamina propria (in d, × 400). This pattern excludes HD. (e): Calretinin immunohistochemistry on a rectal suction biopsy for suspicion of HD showing positivity in Schwann cells and nuclear expression by ganglion cells (insert) in nerve plexus ( × 1000). This pattern excludes HD. (f): Calretinin immunohistochemistry on a rectal suction biopsy for suspicion of HD showing a similar pattern than in Figure 1a but with a slight positivity in large nerve fibers (insert). Original magnification × 250 and × 600 in insert. This case represents an authentic case of HD.
On the basis of calretinin immunohistochemistry results, non-HD diagnosis was made when specific calretinin staining was present and HD was diagnosed when there was no staining. Experienced pathologists made non-HD diagnosis in 78 cases and HD diagnosis in 53 cases, with no discrepancy between the two experienced pathologists, whereas the unaccustomed pathologist made non-HD diagnosis in 79 cases and HD diagnosis in 52 cases.
Statistical Analysis
These calretinin results were first compared with the gold standard: the senior pathologists diagnosed all cases of HD with no false positives. The concordance between calretinin and the gold standard was statistically excellent (κ=0.98, 95% CI (0.95–1.00)). We also compared these results with our standard technique. Calretinin immunohistochemistry enabled the diagnosis of all HD diagnosed by standard technique, except one patient who gave a weak positive immunostaining in some nerve fibers. It is important to note that 12 additional cases initially considered as suspicious for HD using the standard technique was accurately diagnosed by calretinin immunohistochemistry. The concordance between the standard technique and the gold standard was good (κ=0.80, 95% CI (0.70–0.91)).
Using calretinin results, the unaccustomed pathologist failed to diagnose three cases of HD and made one false-positive diagnosis. The concordance between calretinin and the gold standard was statistically excellent: κ=0.94 95% CI (0.88–1.00). Finally, the concordance for calretinin between the experienced pathologists and the unaccustomed pathologist in diagnosing HD was excellent: κ=0.95, 95% CI (0.90–1.00).
Acetylcholinesterase Expression by the Unaccustomed Pathologist in Diagnosing HD
Acetylcholinesterase expression was analyzed by the junior pathologist: 43 biopsies were found, by the junior pathologist, to have abnormal acetylcholinesterase pattern and were thus classified as HD. The remaining biopsies were considered to have a normal pattern and were classified as non-HD. There were 15 false negatives (undiagnosed HD) and 4 false positives. The concordance between acetylcholinesterase and the gold standard was average: κ=0.69 (0.57–0.82).
Discussion
Simple suction rectal biopsy is widely used to obtain tissue for histological examination and to diagnose HD. The hematoxylin and eosin is still the diagnostic method of choice for identifying ganglion cells in submucosae in many centers. Diagnosis of HD can be very difficult, particularly for pathologists who encounter this disease infrequently. Ease of diagnosis has been improved with the use of acetylcholinesterase staining, but the main drawbacks of this method are difficulties in staining interpretation and lack of sensibility in neonates or in long-segment HD. Thus, many specimens are still difficult to evaluate and may require repeat rectal biopsies. In a recent study, children suspected of having HD were submitted to rectal suction and there were inadequate procedures leading to repeated biopsies in 6% of patients. 21 Nerve cell bodies in both submucosa and myenteric ganglia of guinea pig 22, 23 and in the human gastrointestinal tract are immunopositive for calretinin, a calcium-binding protein. 24 Recently, it has been suggested that calretinin might be more accurate than acetylcholinesterase in detecting aganglionosis 18 in a small series of rectal biopsy. Our study demonstrates for the first time in a large series of rectal suction biopsies that pathologists can diagnose all cases of HD with no false positives using the sole immunohistochemistry with calretinin antibody, and that the concordance between calretinin and the gold standard (ie, surgery for HD patients) is statistically excellent, whereas the concordance between the standard technique and the Gold standard is only good. It is interesting to note that even senior pathologists failed to diagnose with assurance 12 cases of HD using the standard method (combination of histology and acetylcholinesterase histochemistry), and repeat biopsies were required to confirm or exclude HD. Calretinin immunohistochemistry was able to easily discriminate all these cases and could thus avoid repeat biopsies in these children. Furthermore, we demonstrate that the concordance between calretinin and the gold standard is also excellent, even for the pathologist unaccustomed to HD diagnosis, and that calretinin is more accurate than acetylcholinesterase in the diagnosis of HD. Abnormal distribution and abnormal intensity of staining reaction in the lamina propria, muscularis mucosae, numerical excess of small submucosal nerves and the presence or absence of large submucosal nerves obtained with acetylcholinesterase histochemistry 7 are much more difficult to interpret for an unaccustomed pathologist than is the ‘black and white pattern’ of calretinin staining. In addition, calretinin histochemistry overcomes most of the difficulties encountered using the combination of histology and acetylcholinesterase and detects almost all cases of HD with confidence, with no false positives and an excellent concordance for calretinin between the senior pathologists and the unaccustomed pathologist.
As suggested by previous studies, we expected that a positive staining with the calretinin antibody was strictly correlated to the presence of ganglion cells in submucosae and that, in HD, calretinin immunostaining was always negative in nerve fibers. This hypothesis seemed partially wrong, as calretinin immunohistochemistry may indeed give a slight positive staining of some nerve fibers but with no other staining (ie, muscularis mucosae, lamina propria or nuclear staining) in authentic HD, thus explaining our false-negative case using the sole immunohistochemistry with calretinin antibody. It is interesting enough to note that surgery revealed a short-segment HD with only 2 cm of aganglionosis in this patient. We extrapolate that in short-segment HD, a slight calretinin positivity can be observed in some large nerve bundles and could indicate the beginning of a transitional zone as previously observed by Barshack et al. 17 To avoid this potential and exceptional pitfall, calretinin should be used in combination with standard histology.
For Kapur RP, 25 an ideal immunohistochemical marker would be easy to use and interpret, it works with paraffin section and circumvents the need to analyze large numbers of histological hematein–eosin levels. Calretinin seems to achieve all these properties when combined with a limited analysis of hematein–eosin levels to confirm the absence of ganglion cells.
In conclusion, this study demonstrates for the first time in a large series of rectal suction biopsies that calretinin immunohistochemistry seems to be a valuable diagnostic tool for HD on rectal suction biopsy, as the absence of staining in the superficial submucosa and muscularis mucosae is pathognomonic of the disease. In these cases, only five hematein–eosin sections could be performed to ensure the absence of ganglion cells instead of the 100 hematein–eosin sections usually required. We also show that calretinin immunohistochemistry is more accurate than acetylcholinesterase to complete histology and advantageously substitutes for acetylcholinesterase. This binary pattern of interpretation (positive/negative) gives the technique distinctive ease and reproducibility, avoiding the need for repeated biopsies and delayed treatment. But because of the phenotypically heterogeneous nature of HD as provided by Kapur, 18 the utility of calretinin immunohistochemistry, in particular in circumstances such as ultra-short segment HD or transitional zone assessments, remains to be determined, and calretinin immunohistochemistry should always be used in addition to limited hematoxylin and eosin sections.
Disclosure/conflict of interest
The authors declare no conflict of interest.
References
Haricharan RN, Georgeson KE . Hirschsprung disease. Semin Pediatr Surg 2008;17:266–275.
Yunis EJ, Dibbins AW, Sherman FE . Rectal suction biopsy in the diagnosis of Hirschsprung disease in infants. Arch Pathol Lab Med 1976;100:329–333.
de Lorijn F, Kremer LC, Reitsma JB, et al. Diagnostic tests in Hirschsprung disease: a systematic review. J Pediatr Gastroenterol Nutr 2006;42:496–505.
Martucciello G, Pini Prato A, Puri P, et al. Controversies concerning diagnostic guidelines for anomalies of the enteric nervous system: a report from the fourth International Symposium on Hirschsprung's disease and related neurocristopathies. J Pediatr Surg 2005;40:1527–1531.
Kessmann J . Hirschsprung's disease: diagnosis and management. Am Fam Physician 2006;74:1319–1322.
Meier-Ruge WA, Bruder E . Current concepts of enzyme histochemistry in modern pathology. Pathobiology 2008;75:233–243.
Pacheco MC, Bove KE . Variability of acetylcholinesterase hyperinnervation patterns in distal rectal suction biopsy specimens in Hirschsprung disease. Pediatr Dev Pathol 2008;11:274–282.
Nakao M, Suita S, Taguchi T, et al. Fourteen-year experience of acetylcholinesterase staining for rectal mucosal biopsy in neonatal Hirschsprung's disease. J Pediatr Surg 2001;36:1357–1363.
Wakely Jr PE, McAdams AJ . Acetylcholinesterase histochemistry and the diagnosis of Hirschsprung's disease: a 31/2-year experience. Pediatr Pathol 1984;2:35–46.
Chentanez V, Chittmittrapap S, Cheepsoonthorn P, et al. New classification of histochemical staining patterns of acetylcholinesterase activity in rectal suction biopsy in Hirschsprung's disease. J Med Assoc Thai 2000;83:1196–1201.
Meier-Ruge WA, Bruder E, Holschneider AM, et al. Diagnosis and therapy of ultrashort Hirschsprung's disease. Eur J Pediatr Surg 2004;14:392–397.
Goto S, Ikeda K, Nagasaki A, et al. Histochemical acetylcholinesterase reactions in total colonic aganglionosis. Jpn J Surg 1984;14:305–310.
Jasonni V, Martucciello G . Total colonic aganglionosis. Semin Pediatr Surg 1998;7:174–180.
Taguchi T, Tanaka K, Ikeda K . Immunohistochemical study of neuron specific enolase and S-100 protein in Hirschsprung's disease. Virchows Arch A Pathol Anat Histopathol 1985;405:399–409.
Kawana T, Nada O, Ikeda K, et al. Distribution and localization of glial fibrillary acidic protein in colons affected by Hirschsprung's disease. J Pediatr Surg 1989;24:448–452.
Baimbridge KG, Celio MR, Rogers JH . Calcium-binding proteins in the nervous system. Trends Neurosci 1992;15:303–308.
Barshack I, Fridman E, Goldberg I, et al. The loss of Calretinin expression indicates aganglionosis in Hirschsprung's disease. J Clin Pathol 2004;57:712–716.
Kapur RP, Reed RC, Finn L, et al. Calretinin immunohistochemistry versus acetylcholinesterase histochemistry in the evaluation of suction rectal biopsies for Hirschsprung disease. Pediatr Dev Pathol 2009;12:6–15.
Lake BD, Puri P, Nixon HH, et al. Hirschsprung's disease: an appraisal of histochemically demonstrated acetylcholinesterase activity in suction rectal biopsy specimens as an aid to diagnosis. Arch Pathol Lab Med 1978;102:244–247.
Cohen J . A coefficient of agreement for nominal scales. Int Educ Psychol Meas 1960;20:37–46.
Santos MM, Tannuri U, Coelho MC . Study of acetylcholinesterase activity in rectal suction biopsy for diagnosis of intestinal dysganglionoses: 17-year experience of a single center. Pediatr Surg Int 2008;24:715–719.
McConalogue K, Furness JB . Calretinin immunoreactivity of motor neurons in the guinea-pig distal colon and tinia coli. Cell Tissue Res 1996;284:367–372.
Messenger JP, Bornstein JC, Furness JB . Electrophysiological and morphological classification of myenteric neurons in the proximal colon of guinea-pig. Neuroscience 1994;60:227–244.
Walters JR, Bishop AE, Facer P, et al. Calretinin and calbindin-D28k immunoreactivity in the human gastrointestinal tract. Gastroenterology 1993;104:1381–1389.
Kapur RP . Can we stop looking? Immunohistochemistry and the diagnosis of Hirschsprung disease. Am J Clin Pathol 2006;126:9–12.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guinard-Samuel, V., Bonnard, A., De Lagausie, P. et al. Calretinin immunohistochemistry: a simple and efficient tool to diagnose Hirschsprung disease. Mod Pathol 22, 1379–1384 (2009). https://doi.org/10.1038/modpathol.2009.110
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2009.110
Keywords
This article is cited by
-
Diagnostic accuracy of calretinin and acetylcholinesterase staining of rectal suction biopsies in Hirschsprung disease examined by unexperienced pathologists
Virchows Archiv (2022)
-
ERNICA guidelines for the management of rectosigmoid Hirschsprung’s disease
Orphanet Journal of Rare Diseases (2020)
-
Digital pathology imaging and computer-aided diagnostics as a novel tool for standardization of evaluation of aganglionic megacolon (Hirschsprung disease) histopathology
Cell and Tissue Research (2019)
