
Abstract
Objective:
To assess if neonatologists detect and count unplanned extubations (UEs) uniformly.
Study Design:
An Institutional Review Board-exempted anonymous web-based survey of neonatology attending and fellow members of the AAP Neonatal-Perinatal Medicine section was administered. Respondents were queried on practices concerning UE; they were then presented with different case scenarios and asked if they would count the event as a UE.
Results:
Of the 509 respondents, 61% track UE rates. Of those who track UE rates, 53% reported rates of 1–3 per 100 ventilator days. The top two factors perceived as causing UEs were endotracheal tube (ETT) dislodgement by patient (65%) and failure of ETT holding system at attachment to the face (56%). In the various scenarios where ETT was urgently removed by staff, only 19 to 62% of respondents counted the event as a UE, including 23% if the ETT was removed by the attending. There was consensus on the scenarios representing self-extubation and elective change of the ETT.
Conclusions:
There is wide variation in methods for detecting and counting UE events among neonatologists, which precludes comparison of UE rates across institutions. We speculate that a standardized definition and classification of events will enable benchmarking among neonatal intensive care units, which should accelerate collaborative improvement efforts towards reducing UEs in neonates.
Similar content being viewed by others

Introduction
Unplanned extubation (UE) requiring reintubation ranks as the fourth most common adverse event in the neonatal intensive care unit (NICU).1 Sixty-two percent of all emergent intubations occur as a result of UE and there is a fourfold increase in the odds of an adverse event occurring during an emergent intubation.2 Hazardous events previously associated with UE include airway trauma, ventilator associated pneumonia, hypoxia, hypercapnia and intraventricular hemorrhage.3
The U.S. News & World Report Best Children’s Hospitals Survey from 2015 to 2016 Survey used unintended removal of the breathing tube as one of the quality measures to rank hospitals.4 UE was defined simply as ‘invasive airway loss’ and also as ‘breathing tube that is removed by a patient or inappropriately by care provider’ by the U.S. News & World Report Survey.4 Others have defined UE as ‘any endotracheal tube removal at a time or fashion, not specifically intended or ordered by a physician’5 or ‘dislodgement or removal of the endotracheal tube (ETT) from the trachea in a patient receiving invasive mechanical ventilation at a time that was not specifically intended or ordered by a physician.’6
These definitions might seem straightforward and equivalent, but based on observations within the four regional perinatal centers in the Upstate New York Collaborative to Reduce Unplanned Extubations (CRUE), it was evident that they are susceptible to individual interpretation. Similar observations were made in the NICU at Albany Medical Center, wherein we observed disagreements among providers on which extubations to classify as unplanned, even after standardizing the definition.
In a commentary on UE in NICU patients, Meyers et al.7 used case scenarios to highlight the fact that these definitions may be subject to individual interpretation, and thus proposed a broad definition of UE be adopted, for example, ‘any extubation that was not intended for that time, or not carried out electively.’
Inconsistency in methods for counting and reporting UEs diminishes the validity of this metric for quality improvement efforts and precludes its use for benchmarking purposes. It may underlie the striking range in monthly UE rates reported in the literature, from <0.5 to about 50 UEs per 100 ventilator days.6, 8 Therefore, we developed a survey questionnaire to better understand how providers count UEs. We hypothesized that neonatologists in the United States do not count UEs uniformly.
Methods
We created and administered an anonymous online survey to neonatology attending and fellow members of the American Academy of Pediatrics Section on Neonatal-Perinatal Medicine through SurveyMonkey (www.surveymonkey.com). A group e-mail was distributed to approximately 3000 addresses with a link to the survey; a reminder e-mail was sent after 1 month. The survey project was deemed exempt by the Institutional Review Board at Crouse Hospital (Syracuse, NY, USA). The survey contained questions that targeted common practices and opinions on UE. Respondents were asked if their institution currently tracks UEs, what systems are in place to track UEs and to share their local UE rate if known. Respondents were also presented with different case scenarios and asked if they would count each event as a UE.
The seven clinical scenarios of UE varied by seniority of clinician who decided to remove the ETT as well as urgency and location of extubation. The eighth scenario was intended as a control and represented a planned extubation. Respondents were then asked to share their opinion on whether they would count each scenario as a UE. For the purpose of the survey, we defined UE as ‘any extubation that was not performed electively or not previously intended for that time.’ A dislodged tube was defined as any ETT that was found to be out of the trachea. If there was no clear evidence that the ETT was already out of the trachea, it was classified as a removed tube. Simple descriptive statistical analyses were performed with Excel (Microsoft Corporation, Redwood, WA, USA), and correlation analyses were carried out with Stata 13 (StataCorp, LLC, College Station, TX, USA). The survey questionnaire is detailed in Supplementary Appendix SA1.
Results
There were 509 survey respondents. Attending neonatologists comprised 89% and fellows 11%. Forty-nine percent of the respondents practiced in a level III NICU, 46% in a level IV NICU and 5% in a level II NICU. Ninety-four percent of the respondents have an obstetrics/delivery service and 82% have a neonatal transport team.
Eighty-nine percent of neonatologists surveyed believe the frequency of UEs should be routinely tracked. Sixty-one percent of the respondents currently have a system in place to track UEs. Fifty-three percent of those who have a system in place to track UEs reported rates of 1 to 3 per 100 ventilator days in their NICU setting.
The primary data source for tracking UE events was a paper-based system (42%), followed by web-based (26%) and electronic medical record (20%). Respondents could indicate one or more method used to secure ETTs in their NICU setting. The most commonly used device was tape (65%), followed by NeoBar (Neotech, Valencia, CA, USA) (48%) and NEO-fit (Cooper Surgical, Trumbull, CT, USA) (10%). Respondents surmised that the top two factors that contributed to UE were ETT dislodgement by patient and failure of ETT holding system at attachment to the face (Table 1).
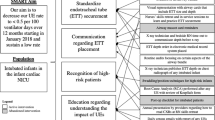
The clinical scenarios explored how respondents would count an extubation if the ETT was dislodged or removed (Figure 1). In the various extubation scenarios where the ETT was urgently removed by staff, the event was counted as a UE by 19 to 62% of respondents. In the scenario in which a baby acutely decompensated and the ETT was urgently removed by the attending neonatologist, only 23% counted the event as a UE.

Responses to clinical scenarios, regarding when a UE would be counted. ETT, endotracheal tube; Rx, treatment; UE, unplanned extubation.
For UEs occurring at a location outside the NICU, 76% of respondents would count a UE if it occurs in the delivery room, 73% if the UE happens in the operating room and 85% if it takes place on transport. If the baby remains extubated after a UE, 15% of the respondents would not count the event as a UE.
There was no correlation between the UE detection and reporting method (paper-based, web-based, electronic medical record, other) and the reported UE rate (continuity corrected Kendall’s tau-b=−0.045, P=0.5). However, the reported UE rate was significantly correlated with the ETT holding method, with rates <1/100 ventilator days being reported more frequently in association with securement by tape than with commercial or other devices (Kendall’s tau-b=−0.256, P=0.002) (Supplementary Table S2).
Discussion
Our survey confirms that there is wide heterogeneity in how neonatologists count UEs. This variation likely stems from the use of commonly cited definitions of UE that are not explicit operational definitions and are thus subject to individualized interpretations. Meyers et al.7 brought attention to the fact that providers may not be counting UEs similarly given the same clinical scenarios. A potential reason for this disparity might be ambiguity in the commonly cited definitions of UE. The interchange among terms such as ‘unintended extubation,’ ‘unplanned extubation’ and ‘self-extubation,’ each with subtly different connotations, likely contributes to the inconsistency in counting and reporting UEs.
The U.S. News and World Report Best Children’s Hospitals defines unintended removal of the breathing tube as a ‘breathing tube that is removed by a patient or inappropriately by a care provider.’4 When the above definition is applied, all ‘self extubations’ should be counted as UEs. Our survey results support this concept, as almost all respondents counted an extubation as unplanned when the ETT was dislodged by the patient. However, this definition also leaves room for individual interpretation as to what is considered ‘inappropriate’ removal of the ETT by a care provider. This ambiguity may have translated into the dissimilarities observed in how respondents counted UEs when the ETT was removed by a provider. The majority of neonatologists in our survey did not count an extubation as unplanned when the ETT was removed by a care provider.
Loughead et al.5 defined UE as ‘any endotracheal tube removal at a time, or fashion, not specifically intended or ordered by a physician.’ Most providers will agree that an ETT that is dislodged while being secured or found to be out of the trachea is a UE. Disagreement is observed, however, with ETTs that are or might be intentionally removed from the trachea when a patient is decompensating. In our survey, 71% of respondents failed to count an extubation as a UE if the ETT was removed by the provider. Applying the above definition by Loughead et al., any ETT that was removed in the setting of patient decompensation should be a UE because it was not planned for that time a priori. However, an argument can also be made not to count the removal of the ETT as a UE if the physician gave the order. The word ‘ordered’ in the definition by Loughead et al. might be inferred to entail a planned decision. Removal of the ETT in an acutely decompensating patient, although possibly necessary and appropriate, represents a reaction by the clinician, rather than an action planned before the onset of the event.
A majority of our respondents did not count extubations as UEs when the decision was made by the attending neonatologist. Perhaps this logic is similar to the interpretation of Loughead et al., wherein if the ETT is intentionally removed by a physician it is not a UE. If the ETT was removed at a time not previously planned, even though the decision to remove the ETT was made (and implicitly ordered) by a physician, we would argue that this should be counted as a UE.
Including ‘physician’ in the definition of UE is also problematic because many other healthcare providers, including trainees, nurse practitioners, physician assistants, respiratory therapists, nurses and others, are also involved in making decisions regarding removal of ETTs. Although it may seem reasonable to assume that a more experienced attending physician is less likely to remove an ETT inappropriately, attending physicians are often secondary responders to airway-related crises, and they may have little time to fully evaluate the airway before acting. Hence, it is not clear that the classification of a UE should be dependent on the rank or experience of the provider making the emergent decision to remove the ETT.
Based on our survey results, an ETT that was removed as a result of patient decompensation during surfactant administration was almost universally not counted as a UE by the respondents. In this scenario, ETT removal may possibly be life-saving for the patient. However, the pre-procedure plan would certainly not have been to remove the ETT urgently before the end of surfactant administration, even if there was an intention to extubate after the procedure was completed, such as in the INSURE approach.9
Fontánez-Nieves et al. did not include ETTs that were removed emergently as UE events in their quality improvement work out of concern for ETT occlusion. Of note, among the five patients whose ETT was removed due to fear of plugging, only one of the ETTs was confirmed to be plugged; consequently, the other four ETTs were, in retrospect, removed unnecessarily.8 Similarly, only 1 of 95 UE events was attributed to actual ETT occlusion at the Albany Medical Center NICU.7 Since ETTs are frequently removed by fear of occlusion, having criteria that help distinguish occlusive from non-occlusive contents of the ETT lumen is essential to estimate the proportions of life-saving versus ultimately unnecessary ETT removals.
The location where the extubation event occurred also appeared to contribute to whether survey respondents would count it as a UE. Our survey shows that over 70% of respondents would count UEs that occur outside the NICU, for example on transport, in the delivery room or operating room. However, we did not inquire about the systems used for reporting or identifying those events. The definitions commonly used for UE do not place restrictions on the location of the events, but extubations occurring outside the NICU require specific systems (often separate from an electronic record or from paper forms designed for the NICU or delivery room settings) to ensure that they are not missed.
In our survey, the most commonly reported UE rate range was 1 to 3 UEs per 100 ventilator days. In a systematic review on neonatal UE by da Silva et al.,10 a target benchmark for UE rate was suggested to be <1 UE per 100 ventilator days. However, the CRUE network adopted a goal rate of ⩽2 UE per 100 ventilator days after participating in the Vermont Oxford Network’s iNICQ Collaborative on Controversies in Respiratory Care in 2012. An even lower rate of ⩽1 UE per 100 ventilator days was targeted by Merkel et al.6 in their quality improvement work. Knowing that the frequently used definitions of UE are subject to bias, the UE rates reported by survey respondents likely underrepresent the incidence of UE under a more inclusive definition. It is challenging to accurately compare UE rates from one NICU to another for benchmarking purposes if each uses a different version or interpretation of the current UE definitions. Both a uniformly applied definition and reporting systems that capture UE events with similar sensitivity will be required if UE rates are to be compared across NICUs or over time. Nevertheless, even an inaccurate enumeration of these events may yield useful information to guide the minimization of UEs in individual NICUs and thereby enhance patient safety. For regulatory or payment purposes, the existence of a local program to minimize UEs should be noted, but it would be premature to compare UE rates across NICUs without further qualification, at the present time.
Survey respondents perceived ETT dislodgement by the patient and failure of ETT holding system at the attachment to the face as the top two factors contributing to UE. These are the same factors that have been identified by the CRUE, although the proportion of ETTs removed by staff varies across centers (unpublished observations). Understanding these factors will help design interventions that can be implemented to potentially reduce UE rates such as staff education on effective use of the particular holding device used in that NICU. Fontánez-Nieves et al. identified loose tape exacerbated by excessive secretions as the primary driver that led to UEs. In addition to staff education, they standardized the method of securing the ETT which led to a decreased UE rate.8
Finally, although more than two-thirds of respondents agreed that an extubation should be counted as a UE even if the baby did not require immediate reintubation, a significant proportion would excuse these events, presumably because they are less consequential. The small proportion of respondents who would count a planned, elective ETT change as a UE may reflect the importance given by some practitioners to reintubation as the most undesirable component of UE events. There is evidence that multiple intubation attempts is associated with higher adjusted risk of severe intraventricular hemorrhage11 and neurodevelopmental impairment or death in extremely low birth weight infants when compared with a single successful intubation.12
From a patient’s perspective, a UE may occasionally be life-saving but it can also lead to significant morbidity in cases where there is cardiorespiratory decompensation and the need for emergent reintubation. Therefore, even the rare necessary UE due to a plugged ETT indicates a risk to the patient. Furthermore, unobstructed ETTs removed by providers due to fear of plugging are in retrospect unnecessary UEs. Thus, we suggest that a standardized operational definition of UE should capture all the events where the ETT is dislodged or removed at a time or in a manner not planned, regardless of whether or not it leads to reintubation. Further characterization of the subtypes of UE will enable NICUs to not only compare rates but also discern ways by which they can most effectively decrease their local UE rates. From the perspectives of both patients and individual NICUs, it may be more important to have a formal system designed to identify and reduce local, cause-specific rates of UE and their associated sequelae than to aim for a benchmark rates derived from heterogeneous and dissimilarly measured events.
This study has limitations inherent to any survey study. Despite the large number of respondents and their valuable responses, there is potential response bias which cannot be further evaluated since we have no information on the non-responders. We cannot precisely calculate the response rate, since we cannot exclude invalid e-mail addresses, but it is probably not much greater than 20%. It should be noted that the unit of analysis was the individual respondent, not the institution—anonymity precluded analysis at the institutional level. Another limitation is that non-physician providers were not polled. It would also have been useful to include the perspective of families on safety-related events such as UEs. Finally, the responses relied on the memories and opinions of the survey respondents, which may be subjective and might not accurately represent the reality in their respective NICUs. Nevertheless, these limitations do not invalidate the heterogeneity of interpretation of UEs reflected in the responses to this survey.
Conclusions
There is presently marked variation in how neonatologists count UEs. We postulate that many of these differences occur because current definitions of UE are ambiguous. We therefore suggest a more simplified standardized definition of UE that will not be susceptible to individuals’ interpretations. An example of such a definition is ‘any extubation that was not performed electively, or not previously intended for that time.’ A standardized definition will allow benchmarking and enable better comparisons of UE rates within and among NICUs. Further classification of UE as dislodged or removed ETTs (with or without obstruction) should aid providers in identifying solutions targeted to the predominant types of UEs in their practice setting.
References
Sharek PJ, Horbar JD, Mason W, Bisarya H, Thurm CW, Suresh G et al. Adverse events in the neonatal intensive care unit: development, testing, and findings of an NICU-focused trigger tool to identify harm in North American NICUs. Pediatrics 2006; 118 (4): 1332–1340.
Hatch LD, Grubb PH, Lea AS, Walsh WF, Markham MH, Whitney GM et al. Endotracheal intubation in neonates: a prospective study of adverse safety events in 162 infants. J Pediatr 2016; 168: 62–66 e66.
Brown MS . Prevention of accidental extubation in newborns. Am J Dis Child 1988; 142 (11): 1240–1243.
Olmsted M, Geisen E, Murphy J . Methodology: US News & World Report Best Children’s Hospitals 2015–16. 2015 [cited 6/23/2016]. Available at http://www.usnews.com/pubfiles/BCH_Methodology_2015.pdf.
Loughead JL, Brennan RA, DeJuilio P, Camposeo V, Wengert J, Cooke D . Reducing accidental extubation in neonates. Jt Comm J Qual Patient Saf 2008; 34 (3): 164–170 125.
Merkel L, Beers K, Lewis MM, Stauffer J, Mujsce DJ, Kresch MJ . Reducing unplanned extubations in the NICU. Pediatrics 2014; 133 (5): e1367–e1372.
Meyers JM, Pinheiro J, Nelson MU . Unplanned extubation in NICU patients: are we speaking the same language? J Perinatol 2015; 35 (9): 676–677.
Fontanez-Nieves TD, Frost M, Anday E, Davis D, Cooperberg D, Carey AJ . Prevention of unplanned extubations in neonates through process standardization. J Perinatol 2016; 36 (6): 469–473.
Verder H, Albertsen P, Ebbesen F, Greisen G, Robertson B, Bertelsen A et al. Nasal continuous positive airway pressure and early surfactant therapy for respiratory distress syndrome in newborns of less than 30 weeks' gestation. Pediatrics 1999; 103 (2): E24.
da Silva PS, Reis ME, Aguiar VE, Fonseca MC . Unplanned extubation in the neonatal ICU: a systematic review, critical appraisal, and evidence-based recommendations. Respir Care 2013; 58 (7): 1237–1245.
Sauer CW, Kong JY, Vaucher YE, Finer N, Proudfoot JA, Boutin MA et al. Intubation attempts increase the risk for severe intraventricular hemorrhage in preterm infants—a retrospective cohort study. J Pediatr 2016; 177: 108–113.
Wallenstein MB, Birnie KL, Arain YH, Yang W, Yamada NK, Huffman LC et al. Failed endotracheal intubation and adverse outcomes among extremely low birth weight infants. J Perinatol 2016; 36 (2): 112–115.
Acknowledgements
We thank the staff of CRUE member NICUs for helping to test and improve the draft versions of the questionnaire. CRUE team members who supported this work, including contributing authors, are listed in Supplementary Appendix SA2. We acknowledge Jim Couto for distributing the surveys to the AAP Perinatal Section membership. We appreciate the enthusiastic responses and helpful insights from so many colleagues, who made this survey project an enjoyable learning experience and who helped broaden our perspectives on patient safety.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Journal of Perinatology website
Rights and permissions
About this article

Cite this article
Mbi Ndakor, S., Nelson, M., Pinheiro, J. et al. Counting unplanned extubations: marked variation among neonatologists. J Perinatol 37, 698–701 (2017). https://doi.org/10.1038/jp.2016.273
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2016.273
