
Abstract
Objective:
Inhaled nitric oxide (iNO) is a potential new therapy for prevention of bronchopulmonary dysplasia and brain injury in premature infants. This study examined dose-related effects of iNO on NO metabolites as evidence of NO delivery.
Study Design:
A subset of 102 premature infants in the NO CLD trial, receiving 24 days of iNO (20 p.p.m. decreasing to 2 p.p.m.) or placebo, were analyzed. Tracheal aspirate (TA) and plasma samples collected at enrollment and at intervals during study gas were analyzed for NO metabolites.
Result:
iNO treatment increased NO metabolites in TA at 20 and 10 p.p.m. (1.7- to 2.3-fold vs control) and in plasma at 20, 10, and 5 p.p.m. (1.6- to 2.3-fold). In post hoc analysis, treated infants with lower metabolite levels at entry had an improved clinical outcome.
Conclusion:
iNO causes dose-related increases in NO metabolites in the circulation as well as lung fluid, as evidenced by TA analysis, showing NO delivery to these compartments.
Similar content being viewed by others


Introduction
Improved survival among preterm infants over recent decades has been associated with increased morbidities related to prematurity, in particular bronchopulmonary dysplasia (BPD) or chronic lung disease of prematurity.1 The pathophysiology of this disease involves lung injury secondary to hyperoxia and mechanical ventilation of an immature lung with associated inflammation leading to increased airway resistance, impaired alveolarization, and later interstitial fibrosis and enlarged airspaces.2, 3
Under certain circumstances, inhaled nitric oxide (iNO) is a promising new therapy for prevention of BPD.4, 5, 6, 7 We earlier reported clinical results for the NO CLD trial in which iNO was administered at decreasing doses for 24 days, beginning between 7 and 21 days of life, to ventilated infants of 500 to 1250 g birth weight. Treated infants had a significant reduction in the incidence of BPD at 36 weeks postmenstrual age, less severe lung disease at 40 and 44 weeks, and better pulmonary outcome at 1 year of age.6, 7, 8 In the three trials with prolonged iNO therapy, there was no increase in the incidence of the common morbidities of prematurity and evidence of neuroprotection in two trials.4, 5
At present, there is no information regarding distribution and metabolism of iNO in the premature infant. NO is rapidly oxidized in vivo, and the concentrations of metabolites, primarily nitrite and nitrate, serve as biomarkers for NO.9 The objective of this study was to investigate the effect of iNO, as dosed in the NO CLD study, on delivery of NO to the lung and absorption into the circulation. We determined the relationship between levels of total NO metabolites (NOx) in the tracheal aspirate (TA) and plasma at different iNO doses, and investigated possible associations between metabolite levels and infant outcome.
Methods
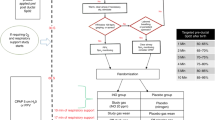
Studies were performed on a subset of infants enrolled in the randomized, placebo-controlled trial (NO CLD) evaluating the effect of iNO in preventing BPD.6 The study enrolled infants of 500 to 1250 g birth weight who were between 7 and 21 days of age and required ventilatory support (mechanical ventilation or nasal continuous positive airway pressure in infants 500 to 799 g). Treated infants received decreasing concentrations of iNO (INOmax, IKARIA, Clinton, NJ, USA) delivered using INOvent (Datex-Ohmeda, Madison, WI, USA), beginning at 7 to 21 days of age according to the following schedule: 20 p.p.m. × 3 days, 10 p.p.m. × 7 days, 5 p.p.m. × 7 days, 2 p.p.m. × 7 days, for a minimum duration of 24 days. Respiratory severity score was used as an index of respiratory support and is calculated as mean airway pressure × fraction of inspired oxygen.
Samples of TA fluid and plasma were obtained at baseline (before starting study gas) and within 24 h of each change of dose of study gas (study days 1, 4, 11, and 18) or until the infant was extubated. TA samples were obtained from 90 infants (47 placebo treated and 43 iNO treated) and plasma samples were obtained from 102 infants (50 placebo treated and 52 iNO treated) from four centers (Children's Hospital of Philadelphia, Hospital of the University of Pennsylvania, Westchester Medical Center, and Children's Mercy Hospitals and Clinics in Kansas City, MO, USA). Approval from the IRB at all participating institutions and informed consent were obtained before patient enrollment and sample collection.
TA samples were collected as described earlier10 using saline lavage according to the schedule noted above. Aspirated samples were placed in sterile tubes, centrifuged at 500 g for 10 min, and the supernatants were stored at −70 °C. After thawing, samples were centrifuged at 27 000 g for isolation of the large aggregate surfactant fraction; results of the surfactant studies have been reported.11 The remaining TA fluid was analyzed for NOx and nitrite as well as analyses of inflammatory and oxidative stress biomarkers that have been reported separately.12, 13 Total NO metabolites, consisting of nitrite, nitrate, S-nitroso, and N-nitroso adducts as well as metal–NO complexes, were determined using the Sievers Nitric Oxide Analyzer Model i280, which is based on a gas-phase chemiluminescent reaction between NO and ozone using vanadium chloride at 95 °C as the reducing agent.14 Concentrations of nitrite were determined using potassium iodide in acetic acid as the reducing agent at 37 °C. To account for dilution of epithelial lining fluid by saline lavage during collection, TA results were normalized to total protein as determined by Bradford assay.15
Blood samples were obtained from the same subset of NO CLD infants. Plasma was obtained by centrifugation, stored at −70 °C, and analyzed for NOx using the Nitric Oxide Analyzer with vanadium chloride reduction as described above. Plasma samples were not stored in an adequate manner for separate analysis of nitrite. Total NOx are reported as μM concentration.
Statistics were performed using STATA V9.2 (College Station, TX, USA). We used the Mann–Whitney test for comparison of nonparametric data such as normalized TA NOx and nitrite comparisons and plasma NOx comparisons at each time point. For continuous or normally distributed data such as severity score, gestational age, and birth weight, the unpaired t-test was used. The two-sample test for equality of proportions with continuity correction was used when analyzing association between entry-level NOx and outcome (by quartile).
Results
We obtained TA samples from 90 infants and plasma samples from 102 infants from a cohort of subjects enrolled in the NO CLD trial.6 There was no difference with respect to gestational age, birth weight, age at entry, or entry severity score in the treatment or control groups for infants with either TA samples or plasma samples (Table 1). These demographics do not differ significantly from those of the entire population of infants in the parent trial (Table 1).
At study entry, before receiving study gas, there was no difference in either TA or plasma NOx levels between control and iNO-treated infants. Furthermore, there was no significant correlation between gestational age, birth weight, age at entry, or respiratory severity score at entry with NOx in plasma or TA at entry (data not shown).
In control infants, there was no change in concentrations of TA NOx or nitrite during the study period (Figures 1a and b, respectively). iNO administration was associated with a 2.3-fold increase in median TA NOx at 20 p.p.m. (51.7 vs 22.5 nmol mg–1 protein, P=0.0003) and a 1.7-fold increase at 10 p.p.m. (35.4 vs 20.4 nmol mg–1, P=0.012). There were no significant differences in NOx at either 5 p.p.m. (Figure 1) or 2 p.p.m. (data not shown). The pattern was similar for nitrite concentrations, with significant increases of 1.8-fold (6.3 vs 3.6 nmol mg–1, P=0.22) at 20 p.p.m. and 2.0-fold (7.8 vs 3.8 nmol mg–1, P=0.017) at 10 p.p.m. for iNO-treated infants. Nitrite as a percentage of total metabolites was similar for both groups at all doses of study gas (mean was 14.2 and 14.4% for iNO and control infants, respectively).

Box and whisker plot of TA NOx (a) and TA nitrite (b) measurements in iNO-treated infants and control infants by dose of study gas. The box represents 25th and 75th percentile with a median bar. The whiskers represent the 10th and 90th percentiles and the heavy bar represents the mean of the samples. Statistical significance was shown at 20 and 10 p.p.m. between the iNO-treated and control infants for both NOx and nitrite. N=34 and 36 at study entry, 37 and 42 at 20 p.p.m., 30 and 30 at 10 p.p.m., 19 and 23 at 5 p.p.m. for treated and control infants, respectively. Only 11 samples for each group were available at 2 p.p.m. and median NOx values were 32.9 and 28.6 nmol mg–1 protein and nitrite values were 5.7 and 3.7 nmol mg–1 for treated and controls, respectively (not shown).
NOx concentrations in plasma of placebo infants had no apparent change during administration of study gas; the median value for 270 samples from 50 infants collected over multiple time points was 36.4 μM. In iNO-treated infants, plasma NOx levels (medians) were significantly increased compared with control infants at 20 p.p.m. (95.9 vs 42.1 μM, P<0.001), 10 p.p.m. (80.9 vs 35.5 μM, P<0.001), and 5 p.p.m. (55.0 vs 34.6 μM, P=0.0016), but not at 2 p.p.m. (44.0 vs 38.7 μM, P=0.37) (Figure 2a). As infants administered control study gas had no apparent time-dependent changes in plasma NOx, we examined the changes in plasma NOx in iNO-treated infants as a function of NO gas doses. Figure 2b shows that when these data are plotted as fold-increase compared with the median control value, a clear dose–response relationship is evident (Figure 2b). To measure the extent of change in plasma NOx after iNO administration, we compared values on days 1 and 3 (equivalent to 20 and recently switched to 10 p.p.m. NO, respectively) to the individual infant's pre-gas value. Plasma NOx increased 2.9±0.2- and 3.6±0.3-fold (mean±s.e., n=37 and 28 on days 1 and 3, respectively). These were significantly (P<0.05) greater than the changes seen in infants receiving placebo gas (1.1±0.1- and 1.2±0.1-fold on days 1 and 3).

(a) Box and whisker plot of plasma NOx in iNO-treated and control infants by dose of study gas. NOx concentrations were significantly elevated in treated infants compared with control at 20, 10, and 5 p.p.m. N=48 and 47 at study entry, 46 and 44 at 20 p.p.m., 42 and 45 at 10 p.p.m., 33 and 35 at 5 p.p.m., and 18 and 22 at 2 p.p.m. for treated and control infants, respectively. (b) Plasma NOx concentrations in iNO-treated infants vs control infants by increasing dose of study gas. The median NOx value for treated infants at each dose of iNO as a percent of the median value of the relevant control infants is presented. NOx values did not change with dose of study gas in control infants. N values at each dose of iNO as noted in (a). Error bars represent the proportional 25th and 75th percentile values.
To elucidate the association between NO metabolite levels and outcome, we first compared TA NOx, TA nitrite, or plasma NOx and outcome in both the treatment and control group at all treatment dose after therapy was initiated and found no significant improvement or deterioration in outcome (data not shown). However, in post hoc analysis, we tested for a possible relationship between TA NOx levels at study entry, which reflects endogenous NO levels, and the clinical outcome of survival without BPD at 36 weeks postmenstrual age (Table 2). Infants were divided into four quartiles based on their NOx concentration in TA related to the median of the entire group. In control infants, outcome was not related to level of NOx at study entry. For treated infants, outcome was better (87.5% survival without BPD) among infants with the lowest quartile of NOx compared with the combined outcome for the other three quartiles (34.6%, P=0.027). The infants in the lowest quartile of NOx did not differ from the remaining infants from whom we received samples as well as those in the parent trial6 with respect to gestational age (25.3 weeks), birth weight (739 g), age at entry (16 days), or entry respiratory severity score (3.5). For comparison, the infants in the highest quartile of NOx had an average gestational age of 25.5 weeks, birth weight of 766 g, age at entry of 17.6 days, and entry respiratory severity score of 5.03. Regarding race, there were three Caucasian and five African–American infants in the lowest quartile compared with five Caucasian, two African American, and one Asian infant in the highest quartile.
Discussion
The use of iNO in premature infants has only recently been investigated in a series of randomized, controlled clinical trials.4, 5, 6, 16 Most trial protocols for the use of iNO to prevent BPD have used <14 days of treatment at ⩽10 p.p.m. iNO. The NO CLD trial was unique in its use of decreasing concentrations of iNO starting at 20 p.p.m. and in continuing treatment for 24 days by nasal cannulae when an infant was extubated. This protocol provided the opportunity to monitor NOx at different iNO doses over an extended period. We report a dose-related effect of iNO on levels of NOx in both TA and plasma, indicating effective delivery of NO to the injured lung and systemic uptake of exogenous NO and/or its metabolites. To our knowledge, this is the first description of metabolites related to use of iNO in the infant. In addition, we provide new information on endogenous NO levels, as reflected by metabolite concentrations, in premature infants. At study entry during the second or third postnatal week, before receiving study gas, total metabolite levels were not associated with degree of prematurity or severity of lung disease. However, a sub-population of the study infants with lower metabolite levels seemed to have a better clinical response to iNO, consistent with the concept of iNO as replacement therapy for a developmental deficiency of endogenous NO production.3, 17
In the premature baboon model of BPD, iNO at 5 p.p.m. for 2 weeks beginning at birth improved respiratory function and lung structure.3 The level of total NOx in TA fluid did not change, consistent with our observations in the human infant at this dose.18 Plasma NOx levels were increased ∼twofold in treated animals throughout the time of iNO administration, which is similar to the findings at 5 to 10 p.p.m. iNO in this study of human infants.
As NO cannot be directly measured in stored biological samples, levels of nitrite and total NO oxidative metabolites were used as surrogate markers for NO. Nitrite represented ∼14% of NOx in TA fluid, indicating that nitrate and potentially other NO metabolites constitute most of NO species present. Although it is clear from both this study and the baboon model that iNO can lead to an increase in plasma-borne NOx, it is uncertain whether NO and/or its metabolites diffuse across the lung. Studies in mice and rabbits showed that within 10 min after intratracheal instillation of nitrite, the levels in lung and plasma were equal.19 Nitrite represents a portion of the bioactive pool of NO metabolites and has been shown to provide protection after ischemia–reperfusion injury in a variety of tissues, including the brain, in animal studies.9 In this regard, it is noteworthy that Kinsella et al.5 showed on head ultrasound an overall decrease in the combined outcome of grade 3 or 4 intraventricular hemorrhage, periventricular leukomalacia, and ventriculomegaly in their iNO-treated group. Furthermore, Mestan et al.20 described an improvement in neurodevelopmental outcome, specifically in the cognitive portion of the Bayley Scale of Infant Development, in the iNO-treated infants compared with control in the Schreiber trial,4 which persisted after adjustment for the decrease in severe intraventricular hemorrhage and periventricular leukomalacia. The observations of elevated NOx support the possibility for extrapulmonary effects of iNO in infants that may be independent of improved pulmonary status.
There were no associations observed between TA or plasma NOx concentrations at study entry and measures of prematurity or severity of lung disease. Infant baboons delivered prematurely (at the end of the second trimester) are deficient in endogenous NO production, and NO synthase activity remains suppressed after birth.17 Our observations suggest that endogenous NO production in sick preterm human infants does not increase appreciably between 24 and 30 weeks, or, alternatively, that developmental changes are not observed within the postnatal timeframe of this study. The concentration of plasma NOx in control infants (36.4 μM) is somewhat lower than the level reported for healthy full-term infants on day 5 (55.2 μM), perhaps reflecting an effect of gestational age.21
Infants with lower TA NOx levels at entry seemed to have a better clinical response to iNO therapy (survival without BPD) than infants with higher entry NOx, consistent with the concept that insufficiency of endogenous NO contributes to BPD. An alternative hypothesis is that the infants in the lowest quartile have a lesser degree of inflammation or oxidative stress at study entry. To support this hypothesis, we examined the 8-epi PGF 2α levels in these infants and found them to be lower (86 ng mg–1 protein) than what we have earlier reported in a larger group of iNO responders,12 but there was wide variability in this measurement (0.35 to 534 ng mg–1 protein). These results should be interpreted with caution and need confirmation because of the relatively small number of infants in each quartile of NOx concentration.
Conversely, we did not find an association with NOx levels and adverse outcome at any dose in either the iNO-treated or control infants in this study. Specific NO metabolites have been described before in relation to BPD and response to therapy. Banks et al. showed that a specific NO metabolite, 3-nitrotyrosine, is elevated in plasma in the first month of life in infants who develop BPD. Furthermore, increased levels of 3-nitrotyrosine after the first month of life correlated with the fraction of inspired oxygen the infant was receiving.22 Lorch et al. described the plasma levels of 3-nitrotyrosine in infants with BPD who were receiving iNO. A significant decrease within the first 72 h after starting therapy was observed in those infants who were weaned off mechanical ventilation compared with those who remained on mechanical ventilation at discharge or who expired.23 These data suggest that markers of nitrative and oxidative stress are associated with both BPD and response to therapy. We have previously reported from data in the NO CLD trial that 3-nitrotyrosine did not change in infants with and without BPD, whether they were receiving iNO or placebo.13 This discrepancy may be explained by differences in study population, severity of illness, progression of clinical course, when samples were taken, or differences in assay techniques. However, given that 3-nitrotyrosine is a small component of total NOx metabolites, it is not surprising that we did not see changes in this study.
There are several limitations to this study. First, TA samples could not be obtained after infants were extubated, which reduced the number of samples available at 5 and 2 p.p.m. and accordingly reduced the power of our study at these points. In general, variability in the TA data was greater than in plasma values, which reflects in part the necessity to use an imperfect denominator (total protein) to correct for dilution of epithelial lining fluid by the lavage saline. Second, infants from whom samples were received were from a subset of NO CLD trial sites enrolling patients. Although their demographics were the same as infants in the parent trial, and, therefore, representative of the entire cohort, this remains a limitation. Third, although infants in this study had similar nutritional management strategies, there was no specific control over or measurement of nitrate intake, which may influence the measurement of NOx within plasma. Lastly, as NO cannot be directly measured within these samples, one must rely on measurements of its most abundant metabolites as markers of NO content.
In conclusion, we have shown that iNO therapy for premature infants results in dose-related increases in NOx in both lung fluid and the circulation. These findings indicate the efficiency and quantitative nature of NO delivery to infants with lung disease and raise the possibility of increased delivery of NO to other tissues with iNO therapy. As iNO treatment is not associated with increased incidence of co-morbidities of prematurity, and may offer neuroprotection, uptake of NO and metabolites into the circulation may represent an additional benefit of iNO for the at-risk premature infant.
Conflict of interest
RAB and PLB have received research grant support and advisor fees from IKARIA (formerly INO Therapeutics). SGG has received speaker's fees from IKARIA. IKARIA provided study gas and masked delivery systems for the primary NO CLD trial, but did not financially support or have a role in the design, analysis, interpretation, or reporting of this study. MAP wrote the first draft of the paper.
References
Wilson-Costello D, Friedman H, Minich N, Fanaroff AA, Hack M . Improved survival rates with increased neurodevelopmental disability for extremely low birth weight infants in the 1990s. Pedatrics 2005; 115: 997–1003.
Bland RD . Neonatal chronic lung disease in the post-surfactant era—lessons learned from authentic animal models. Biol Neonate 2005; 88: 181–191.
McCurnin DC, Pierce RA, Chang LY, Gibson LL, Osborne-Lawrence S, Yoder BA et al. Inhaled NO improves early pulmonary function and modifies lung growth and elastin deposition in a baboon model of neonatal chronic lung disease. Am J Physiol Lung Cell Mol Physiol 2005; 288 (3): L450–L459.
Schreiber MD, Gin-Mestan K, Marks JD, Huo D, Lee G, Srisuparp P . Inhaled nitric oxide in premature infants with the respiratory distress syndrome. N Engl J Med 2003; 349 (22): 2099–2107.
Kinsella JP, Cutter GR, Walsh WF, Gerstmann DR, Bose CL, Hart C et al. Early inhaled nitric oxide therapy in premature newborns with respiratory failure. N Engl J Med 2006; 355 (4): 354–364.
Ballard RA, Truog WE, Cnaan A, Martin RJ, Ballard PL, Merrill JD et al. Inhaled nitric oxide in preterm infants undergoing mechanical ventilation. N Engl J Med 2006; 355 (4): 343–353.
Ballard RA . Inhaled nitric oxide in preterm infants—correction. New Engl J Med 2007; 357 (14): 1444–1445.
Hibbs AM, Walsh MC, Martin RJ, Truog WE, Lorch SA, Alessandrini E et al. One year respiratory outcomes of preterm infants enrolled in the nitiric oxide (to prevent) chronic lung disease trial. J Pediatr 2008; 153 (4): 525–529; Epub ahead of print.
Dezfulian C, Raat N, Shiva S, Gladwin MT . Role of the anion nitrite in ischemia-reperfusion cytoprotection and therapeutics. Cardiovasc Res 2007; 75: 317–338.
Ballard PL, Merrill JD, Godinez RI, Godinez MH, Truog WE, Ballard RA . Surfactant protein profile of pulmonary surfactant in premature infants. Am J Respir Crit Care Med 2003; 168 (9): 1123–1128.
Ballard PL, Merrill JD, Truog WE, Godinez RI, Godinez MH, McDevitt TM et al. Surfactant function and composition in premature infants treated with inhaled nitric oxide. Pediatrics 2007; 120 (2): 346–353.
Truog WE, Ballard PL, Norberg M, Golombek S, Savani RC, Merrill JD et al. Inflammatory markers and mediators in tracheal fluid of premature infants treated with inhaled nitric oxide. Pediatrics 2007; 19 (4): 670–678.
Ballard PL, Truog WE, Merrill JD, Gow A, Posencheg M, Golombek SG et al. Plasma biomarkers of oxidative stress: relationship to lung disease and inhaled nitric oxide therapy in premature infants. Pedatrics 2008; 121: 555–561.
Gow AJ, Thom SR, Brass C, Ischiropoulos H . Electrochemical detection of nitric oxide in biological systems. Microchem J 1997; 56: 146–154.
Bradford MM . A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal Biochem 1976; 72: 248–254.
Van Meurs KP, Wright LL, Ehrenkranz RA, Lemons JA, Ball MB, Poole WK et al. Inhaled nitric oxide for preterm infants with severe respiratory failure. New Engl J Med 2005; 353: 13–22.
Shaul PW, Afshar S, Gibson LL, Sherman TS, Kerecman JD, Grubb PH et al. Developmental changes in nitric oxide synthase isoform expression and nitric oxide production in fetal baboon lung. Am J Physiol Lung Cell Mol Physiol 2002; 283: L1192–L1199.
Munson DA, Grubb PH, Kerecman JD, McCurnin DC, Yoder BA, Hazen SL et al. Pulmonary and systemic nitric oxide metabolites in a baboon model of neonatal chronic lung disease. Am J Respir Cell Mol Biol 2005; 33 (6): 582–588.
Parks NJ, Krohn KA, Mathis CA, Chasko JH, Geiger KR, Gregor ME et al. N-13-labeled nitrite and nitrate—distribution and metabolism after intra-tracheal administration. Science 1981; 212: 58–61.
Mestan KK, Marks JD, Hecok K, Huo D, Schreiber MD . Neurodevelopmental outcomes of premature infants treated with inhaled nitric oxide. New Engl J Med 2005; 353: 13–22.
Endo A, Izumi H, Ayusawa M, Minato M, Takahashi S, Harada K . Spontaneous labor increases nitirc oxide synthesis during the early neonatal period. Pediatr Int 2001; 43: 340–342.
Banks BA, Ischiropoulos H, McClelland M, Ballard PL, Ballard RA . Plasma 3-nitrotyrosine is elevated in premature infants who develop bronchopulmonary dysplasia. Pediatrics 1998; 101 (5): 870–874.
Lorch SA, Banks BA, Christie J, Merrill JD, Althaus J, Schmidt K et al. Plasma 3-nitrotyrosine and outcome in neonates with severe bronchopulmonary dysplasia after inhaled nitric oxide. Free Radic Biol Med 2003; 34 (9): 1146–1152.
Acknowledgements
We thank the nurses, respiratory therapists, and physicians at participating hospitals, the NO CLD study coordinators, S Wadlinger and C Coburn, the families and infants who participated in this study, Y Ning, T McDevitt, M Norberg, and C Castor for technical assistance, H Ischiropoulos for assistance with specimen analysis, S Lorch and M Segal for statistical assistance, L Parton and J Merrill for patient recruitment, and IKARIA for providing study equipment and gas. This investigation was supported by grants from the National Institutes of Health: #U01 HL62514; P50 HL56401; P30 HD26979; MRDDRC P30 HD26979; R01 HL70560, HL62472, HL62868, HL75930, and HL 73896; and from General Clinical Research Centers Program: M01 RR00240; M01 RR00084; M01 RR00425; M01 RR001271; M01 RR00064; and M01 RR00080.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Posencheg, M., Gow, A., Truog, W. et al. Inhaled nitric oxide in premature infants: effect on tracheal aspirate and plasma nitric oxide metabolites. J Perinatol 30, 275–280 (2010). https://doi.org/10.1038/jp.2009.155
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2009.155
Keywords
This article is cited by
-
Dietary intake and bio-activation of nitrite and nitrate in newborn infants
Pediatric Research (2015)
-
Late administration of surfactant replacement therapy increases surfactant protein-B content: a randomized pilot study
Pediatric Research (2012)
