
Abstract
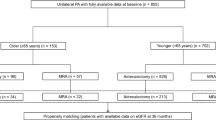
Hyperkalemia is an important complication of adrenalectomy for patients with primary aldosteronism (PA). The frequency of hyperkalemia after medication using mineralocorticoid receptor antagonists (MRAs) for PA is unclear. The aim of this study is to investigate the frequency and the risk factors of hyperkalemia after surgery and medication for PA. The data of 376 patients with PA registered in a multicentre-collaborative study in Japan, including surgically treated patients (group A; n=142) and medically treated patients with MRAs (group B; n=234) were studied. The prevalence of hyperkalemic patients (serum potassium >5.0 mEq l−1) after treatment was higher in group A than group B (9.9 vs 3.8%, P<0.01). At diagnosis, the hyperkalemic patients were older and had a poorer renal function than the non-hyperkalemic patients in both groups (P<0.05). The hyperkalemic patients had severer PA in group A and milder PA in group B. The independent risk factor by a logistic regression analysis was only age in both groups. After treatment, the percentages of patients withdrawing antihypertensive drugs and the normalization of aldosterone renin ratio were not different between hyperkalemic and non-hyperkalemic patients in group A. The type and dose of MRAs and the combination of other antihypertensive drugs were not different between hyperkalemic and non-hyperkalemic patients in group B. In conclusion, the potential occurrence of hyperkalemia should be considered after medical as well as surgical treatment for PA, especially in patients with older age (>60 years) and impaired renal function (estimated glomerular filtration rate <70 ml min−1 per 1.73 m2) at diagnosis.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others


References
Young WF . Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf) 2007; 66: 607–618.
Hannemann A, Wallashofski H . Prevalence of primary aldosteronism in patient’s cohorts and in population-based studies - a review of the current literature. Horm Metab Res. 2012; 44: 157–162.
Mulatero P, Monticone S, Bertello C, Viola A, Tizzani D, Iannaccone A et al. Long-term cardio and cerbo-vascular events in patients with primary aldosteronism. J Clin Endocrinol Metab. 2013; 98: 4826–4833.
Rossi GP . Diagnosis and treatment of primary aldosteronism. Rev Endocr Metab Disord. 2011; 12: 27–36.
Park KS, Kim JH, Ku EJ, Hong AR, Moon MK, Choi SH et al. Clinical risk factors of postoperative hyperkalemia after adrenalectomy in patients with aldosterone-producing adenoma. Eur J Endocrinol. 2015; 172: 725–731.
Fischer E, Hanslik G, Pallauf A, Degenhart C, Linsenmaier U, Beuschlein F et al. Prolonged zona glomerulosa insufficiency causing hyperkalemia in primary aldosteronism after adrenalectomy. J Clin Endocrinol Metab. 2012; 97: 3965–3973.
Chiang W-F, Cheng C-J, Wu S-T, Sun G-H, Lin M-Y, Sung C-C et al. Incidence and factors of post-adrenalectomy hyperkalemia in patients with aldosterone producing adenoma. Clin Chim Acta. 2013; 424: 114–118.
Bauersachs J, Jaisser F, Toto R . Mineralocorticoid receptor activation and mineralocorticoid receptor antagonist treatment in cardiac and renal diseases. Hypertension 2015; 65: 257–263.
Nishikawa T, Omura M, Satoh F, Shibata H, Takahashi K, Tamura N et al. Guidelines for the diagnosis and treatment of primary aldosteronism –The Japan Endocrine Society 2009. Endocr J 2011; 58: 711–721.
Shimamoto K, Ando K, Fujita T, Hasebe N, Higaki J, Horiuchi M et al. The Japanese Society of Hypertension Guidelines for the management of hypertension (JSH2014). Hypertens Res. 2014; 37: 253–390.
Umakoshi N, Wada N, Ichijo T, Kamemura K, Matsuda Y, Fujii Y et al. Optimum position of left adrenal vein sampling for subtype diagnosis in primary aldosteronism. Clin Endocrinol (Oxf) 2015; 83: 768–773.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kid Dis 2009; 53: 982–992.
Karagiannis A, Tziomalos K, Papageorgiou A, Kakafika AI, Pagourelias ED, Anagnostis P et al. Spironolactone versus eplerenone for the treatment of idiopathic hyperaldosteronism. Expert Opin Pharmacother 2008; 9: 509–515.
Pitt B, Zannad F, Remme W, Cody R, Castaigne A, Perez A et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. New Engl J Med 1999; 341: 709–717.
Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. New Engl J Med 2003; 348: 1309–1321.
Vardeny O, Claggett B, Anand I, Rossignol P, Desai AS, Zannad F et al. Incidence, predictors, and outcomes related to hypo- and hyperkalemia in patients with severe heart failure treated with a mineralocorticoid receptor antagonist. Circ heart fail 2014; 7: 573–579.
Pitt B, Bakris G, Ruilope LM, DiCarlo L, Mukherjee R, EPHESUS investigators. Serum potassium and clinical outcomes in the eplerenone post-acute myocardial infarction heart failure efficacy and survival study (EPHESUS). Circulation 2008; 118: 1643–1650.
Acknowledgements
This study was supported in part by grants-in-aid for the study of primary aldosteronism in Japan (JPAS), including a Practical Research Project for Rare/Intractable Diseases from the Japan Agency for Medical Research and Development (AMED) (15Aek0109122) and a Grant for National Center for Global Health and Medicine (26–111).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Wada, N., Shibayama, Y., Umakoshi, H. et al. Hyperkalemia in both surgically and medically treated patients with primary aldosteronism. J Hum Hypertens 31, 627–632 (2017). https://doi.org/10.1038/jhh.2017.38
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhh.2017.38
This article is cited by
-
Practical consensus for the treatment and follow-up of primary aldosteronism: a multidisciplinary consensus document
Endocrine (2024)
-
Primary aldosteronism in elderly, old, and very old patients
Journal of Human Hypertension (2020)
-
Salt intake in mineralocorticoid receptor antagonist-treated primary aldosteronism: foe or ally?
Hormones (2020)
