
Abstract
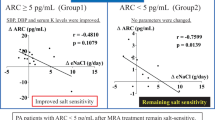
Experimental and human data suggest that adverse cardiovascular (CV) and renal effects of aldosterone excess are dependent on concomitant dietary salt intake. Increased urinary protein (Uprot) is an early sign of nephropathy independently associated with CV risk. We have previously reported a positive association between Uprot and urinary sodium (UNa) in patients with hyperaldosteronism, but not in patients with normal aldosterone levels. We aimed to determine whether Uprot is related to UNa in patients with aldosterone-producing adenoma (APA) and whether the degree of Uprot and strength of this relationship is reduced following correction of hyperaldosteronism. Subjects with APA (n=24) underwent measurement of 24 h Uprot and UNa before and after unilateral adrenalectomy (follow-up 15.0±11.9 months). Following surgery, mean clinic systolic blood pressure fell (150.4±18.2 vs 134.5±14.5 mm Hg, P=0.0008), despite a reduction in number of antihypertensive medications, and Uprot (211.2±101.6 vs 106.0±41.8 mg per day, P<0.0001) decreased. There was a positive correlation between Uprot and UNa both before (r=0.5477, P=0.0056) and after (r=0.5097, P=0.0109) adrenalectomy. Changes in UNa independently predicted Uprot reduction (P=0.0189). These findings suggest that both aldosterone levels and dietary salt contribute to renal damage, and that once glomerular damage occurs it is not completely resolved following correction of hyperaldosteronism. Our study suggests that treatment strategies based on reduction of aldosterone effects, by adrenalectomy or mineralocorticoid receptor blockade, in conjunction with low-salt diet would provide additional target-organ protection in patients with primary aldosteronism.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Conn JW . Presidential address. I. Painting background. II. Primary aldosteronism, a new clinical syndrome. J Lab Clin Med 1955; 45 (1): 3–17.
Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F, Stowasser M et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2008; 93 (9): 3266–3281.
Pimenta E, Calhoun DA . Primary aldosteronism: diagnosis and treatment. J Clin Hypertens (Greenwich) 2006; 8 (12): 887–893.
Stowasser M, Gordon RD, Gunasekera TG, Cowley DC, Ward G, Archibald C et al. High rate of detection of primary aldosteronism, including surgically treatable forms, after ‘non-selective’ screening of hypertensive patients. J Hypertens 2003; 21 (11): 2149–2157.
Lim PO, Dow E, Brennan G, Jung RT, MacDonald TM . High prevalence of primary aldosteronism in the Tayside hypertension clinic population. J Hum Hypertens 2000; 14 (5): 311–315.
Mosso L, Carvajal C, Gonzalez A, Barraza A, Avila F, Montero J et al. Primary aldosteronism and hypertensive disease. Hypertension 2003; 42 (2): 161–165.
Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C et al. A prospective study of the prevalence of primary aldosteronism in 1125 hypertensive patients. J Am Coll Cardiol 2006; 48 (11): 2293–2300.
Stowasser M, Gordon RD, Rutherford JC, Nikwan NZ, Daunt N, Slater GJ . Diagnosis and management of primary aldosteronism. J Renin Angiotensin Aldosterone Syst 2001; 2 (3): 156–169.
Stowasser M, Gordon RD . Primary aldosteronism—careful investigation is essential and rewarding. Mol Cell Endocrinol 2004; 217 (1–2): 33–39.
Sukor N, Kogovsek C, Gordon RD, Robson D, Stowasser M . Improved quality of life, blood pressure, and biochemical status following laparoscopic adrenalectomy for unilateral primary aldosteronism. J Clin Endocrinol Metab 2010; 95 (3): 1360–1364.
Stowasser M, Klemm SA, Tunny TJ, Storie WJ, Rutherford JC, Gordon RD . Response to unilateral adrenalectomy for aldosterone-producing adenoma: effect of potassium levels and angiotensin responsiveness. Clin Exp Pharmacol Physiol 1994; 21 (4): 319–322.
Rutherford JC, Taylor WL, Stowasser M, Gordon RD . Success of surgery for primary aldosteronism judged by residual autonomous aldosterone production. World J Surg 1998; 22 (12): 1243–1245.
Weber KT, Brilla CG . Pathological hypertrophy and cardiac interstitium. Fibrosis and renin-angiotensin-aldosterone system. Circulation 1991; 83 (6): 1849–1865.
Young M, Fullerton M, Dilley R, Funder J . Mineralocorticoids, hypertension, and cardiac fibrosis. J Clin Invest 1994; 93 (6): 2578–2583.
Rocha R, Stier Jr CT, Kifor I, Ochoa-Maya MR, Rennke HG, Williams GH et al. Aldosterone: a mediator of myocardial necrosis and renal arteriopathy. Endocrinology 2000; 141 (10): 3871–3878.
Rocha R, Chander PN, Zuckerman A, Stier Jr CT . Role of aldosterone in renal vascular injury in stroke-prone hypertensive rats. Hypertension 1999; 33 (1 Part 2): 232–237.
Blasi ER, Rocha R, Rudolph AE, Blomme EA, Polly ML, McMahon EG . Aldosterone/salt induces renal inflammation and fibrosis in hypertensive rats. Kidney Int 2003; 63 (5): 1791–1800.
Sato A, Saruta T . Aldosterone-induced organ damage: plasma aldosterone level and inappropriate salt status. Hypertens Res 2004; 27 (5): 303–310.
Abbate M, Benigni A, Bertani T, Remuzzi G . Nephrotoxicity of increased glomerular protein traffic. Nephrol Dial Transplant 1999; 14 (2): 304–312.
Hillege HL, Janssen WM, Bak AA, Diercks GF, Grobbee DE, Crijns HJ et al. Microalbuminuria is common, also in a nondiabetic, nonhypertensive population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity. J Intern Med 2001; 249 (6): 519–526.
Adler AI, Stevens RJ, Manley SE, Bilous RW, Cull CA, Holman RR . Development and progression of nephropathy in type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int 2003; 63 (1): 225–232.
Irie F, Iso H, Sairenchi T, Fukasawa N, Yamagishi K, Ikehara S et al. The relationships of proteinuria, serum creatinine, glomerular filtration rate with cardiovascular disease mortality in Japanese general population. Kidney Int 2006; 69 (7): 1264–1271.
Tonelli M, Jose P, Curhan G, Sacks F, Braunwald E, Pfeffer M . Proteinuria, impaired kidney function, and adverse outcomes in people with coronary disease: analysis of a previously conducted randomised trial. BMJ 2006; 332 (7555): 1426.
Hillege HL, Fidler V, Diercks GF, van Gilst WH, de Zeeuw D, van Veldhuisen DJ et al. Urinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general population. Circulation 2002; 106 (14): 1777–1782.
Rossi GP, Bernini G, Desideri G, Fabris B, Ferri C, Giacchetti G et al. Renal damage in primary aldosteronism: results of the PAPY Study. Hypertension 2006; 48 (2): 232–238.
Halimi JM, Mimran A . Albuminuria in untreated patients with primary aldosteronism or essential hypertension. J Hypertens 1995; 13 (12 Part 2): 1801–1802.
Ribstein J, Du Cailar G, Fesler P, Mimran A . Relative glomerular hyperfiltration in primary aldosteronism. J Am Soc Nephrol 2005; 16 (5): 1320–1325.
Pimenta E, Gaddam KK, Pratt-Ubunama MN, Nishizaka MK, Aban I, Oparil S et al. Relation of dietary salt and aldosterone to urinary protein excretion in subjects with resistant hypertension. Hypertension 2008; 51 (2): 339–344.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42 (6): 1206–1252.
Gordon RD . Primary aldosteronism. J Endocrinol Invest 1995; 18 (7): 495–511.
Jonsson JR, Klemm SA, Tunny TJ, Stowasser M, Gordon RD . A new genetic test for familial hyperaldosteronism type I aids in the detection of curable hypertension. Biochem Biophys Res Commun 1995; 207 (2): 565–571.
Stowasser M, Gordon RD . The aldosterone-renin ratio in screening for primary aldosteronism. Endocrinologist 2004; 14 (5): 267–276.
Haber E, Koerner T, Page LB, Kliman B, Purnode A . Application of a radioimmunoassay for angiotensin I to the physiologic measurements of plasma renin activity in normal human subjects. J Clin Endocrinol Metab 1969; 29 (10): 1349–1355.
Ferrari P, Shaw SG, Nicod J, Saner E, Nussberger J . Active renin versus plasma renin activity to define aldosterone-to-renin ratio for primary aldosteronism. J Hypertens 2004; 22 (2): 377–381.
Mayes D, Furuyama S, Kem DC, Nugent CA . A radioimmunoassay for plasma aldosterone. J Clin Endocrinol Metab 1970; 30 (5): 682–685.
Perschel FH, Schemer R, Seiler L, Reincke M, Deinum J, Maser-Gluth C et al. Rapid screening test for primary hyperaldosteronism: ratio of plasma aldosterone to renin concentration determined by fully automated chemiluminescence immunoassays. Clin Chem 2004; 50 (9): 1650–1655.
Sechi LA, Novello M, Lapenna R, Baroselli S, Nadalini E, Colussi GL et al. Long-term renal outcomes in patients with primary aldosteronism. JAMA 2006; 295 (22): 2638–2645.
Catena C, Colussi G, Sechi LA . Renal function in primary aldosteronism. Hypertension 2006; 48 (6): e110; author reply e111.
Fox CS, Larson MG, Hwang SJ, Leip EP, Rifai N, Levy D et al. Cross-sectional relations of serum aldosterone and urine sodium excretion to urinary albumin excretion in a community-based sample. Kidney Int 2006; 69 (11): 2064–2069.
Weir MR, Dengel DR, Behrens MT, Goldberg AP . Salt-induced increases in systolic blood pressure affect renal hemodynamics and proteinuria. Hypertension 1995; 25 (6): 1339–1344.
Bigazzi R, Bianchi S, Baldari D, Sgherri G, Baldari G, Campese VM . Microalbuminuria in salt-sensitive patients. A marker for renal and cardiovascular risk factors. Hypertension 1994; 23 (2): 195–199.
Sanders PW . Vascular consequences of dietary salt intake. Am J Physiol Renal Physiol 2009; 297 (2): F237–F243.
Sanders PW . Dietary salt intake, salt sensitivity, and cardiovascular health. Hypertension 2009; 53 (3): 442–445.
Rocha R, Rudolph AE, Frierdich GE, Nachowiak DA, Kekec BK, Blomme EA et al. Aldosterone induces a vascular inflammatory phenotype in the rat heart. Am J Physiol Heart Circ Physiol 2002; 283 (5): H1802–H1810.
Geerling JC, Loewy AD . Central regulation of sodium appetite. Exp Physiol 2008; 93 (2): 177–209.
Hollenberg NK . Aldosterone in the development and progression of renal injury. Kidney Int 2004; 66 (1): 1–9.
Arima S, Kohagura K, Xu HL, Sugawara A, Abe T, Satoh F et al. Nongenomic vascular action of aldosterone in the glomerular microcirculation. J Am Soc Nephrol 2003; 14 (9): 2255–2263.
Uhrenholt TR, Schjerning J, Hansen PB, Norregaard R, Jensen BL, Sorensen GL et al. Rapid inhibition of vasoconstriction in renal afferent arterioles by aldosterone. Circ Res 2003; 93 (12): 1258–1266.
Matavelli LC, Zhou X, Varagic J, Susic D, Frohlich ED . Salt loading produces severe renal hemodynamic dysfunction independent of arterial pressure in spontaneously hypertensive rats. Am J Physiol Heart Circ Physiol 2007; 292 (2): H814–H819.
Yu HC, Burrell LM, Black MJ, Wu LL, Dilley RJ, Cooper ME et al. Salt induces myocardial and renal fibrosis in normotensive and hypertensive rats. Circulation 1998; 98 (23): 2621–2628.
Milliez P, Girerd X, Plouin PF, Blacher J, Safar ME, Mourad JJ . Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol 2005; 45 (8): 1243–1248.
Tuomilehto J, Jousilahti P, Rastenyte D, Moltchanov V, Tanskanen A, Pietinen P et al. Urinary sodium excretion and cardiovascular mortality in Finland: a prospective study. Lancet 2001; 357 (9259): 848–851.
Fallo F, Veglio F, Bertello C, Sonino N, Della Mea P, Ermani M et al. Prevalence and characteristics of the metabolic syndrome in primary aldosteronism. J Clin Endocrinol Metab 2006; 91 (2): 454–459.
Bochud M, Nussberger J, Bovet P, Maillard MR, Elston RC, Paccaud F et al. Plasma aldosterone is independently associated with the metabolic syndrome. Hypertension 2006; 48 (2): 239–245.
Matrozova J, Steichen O, Amar L, Zacharieva S, Jeunemaitre X, Plouin PF . Fasting plasma glucose and serum lipids in patients with primary aldosteronism: a controlled cross-sectional study. Hypertension 2009; 53 (4): 605–610.
Pimenta E, Calhoun DA . Aldosterone and metabolic dysfunction: an unresolved issue. Hypertension 2009; 53 (4): 585–586.
Catena C, Colussi G, Nadalini E, Chiuch A, Baroselli S, Lapenna R et al. Cardiovascular outcomes in patients with primary aldosteronism after treatment. Arch Intern Med 2008; 168 (1): 80–85.
Catena C, Colussi G, Lapenna R, Nadalini E, Chiuch A, Gianfagna P et al. Long-term cardiac effects of adrenalectomy or mineralocorticoid antagonists in patients with primary aldosteronism. Hypertension 2007; 50 (5): 911–918.
Young Jr WF . Primary aldosteronism--one picture is not worth a thousand words. Ann Intern Med 2009; 151 (5): 357–358.
Kempers MJ, Lenders JW, van Outheusden L, van der Wilt GJ, Schultze Kool LJ, Hermus AR et al. Systematic review: diagnostic procedures to differentiate unilateral from bilateral adrenal abnormality in primary aldosteronism. Ann Intern Med 2009; 151 (5): 329–337.
Freel M, Ingram M, Fraser R, Dominiczak A, Davies E, Connell J . Aldosterone and sodium excess associate with albuminuria and glomerular hyperfiltration in a severely hypertensive cohort from the MRC BRIGHT Study. Hypertension 2009; 54 (4): e51.
Acknowledgements
This work was supported by a Clinical Centre of Research Excellence in Cardiovascular Disease and Metabolic Disorders Grant awarded by the National Health and Medical Research Council of Australia.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Pimenta, E., Gordon, R., Ahmed, A. et al. Unilateral adrenalectomy improves urinary protein excretion but does not abolish its relationship to sodium excretion in patients with aldosterone-producing adenoma. J Hum Hypertens 25, 592–599 (2011). https://doi.org/10.1038/jhh.2010.102
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhh.2010.102
Keywords
This article is cited by
-
Aldosterone Excess and Resistant Hypertension: Investigation and Treatment
Current Hypertension Reports (2014)
-
The mitochondrial SIRT1–PGC-1α axis in podocyte injury
Kidney International (2012)
