
Abstract
Owing to lack of data from multiple air quality monitoring stations, studies about spatial association between concentrations of ambient pollutants and mortality in China are rare. To investigate the spatial variation of association between concentrations of particulate matter less than 10 μm in aerodynamic diameter (PM10), nitrogen dioxide (NO2) and carbon monoxide (CO) and cardiovascular mortality in Beijing, China, we collected data including daily deaths, concentrations of PM10, NO2 and CO, and meteorological factors from 1 January 2009 to 31 December 2010 in all 16 districts of Beijing. Generalized additive model (GAM) and generalized additive mixed model (GAMM) were used to examine the citywide and district-specific effects of PM10, NO2 and CO on cardiovascular mortality. The citywide effect derived from GAMM was lower than that derived from GAM, and the strongest effects were identified for 2-day moving average lag 0–1. The interquartile increases in concentrations of PM10, NO2 and CO were associated with 2.46 (95% confidence interval (CI), 1.22–3.72), 4.11 (95%CI, 2.82–5.42) and 2.23 (95%CI, 1.14–3.33) percentage increases in daily cardiovascular mortality by GAMM, respectively. The relative risk of each district compared with reference district was generally statistically significant. The death risk associated with air pollutants varies across different geographic districts in Beijing. The data indicate that the risk is high in suburban areas and rural counties. We found significant and spatially varied adverse effects of air pollution on cardiovascular deaths across the rural and urban areas in Beijing.
Similar content being viewed by others

Introduction
Association of air pollution with human health has been evaluated in numerous time-series studies by fitting Poisson regression model at community or city level.1, 2, 3, 4, 5, 6, 7 Results of these studies suggest that short-term exposure to ambient air pollution is associated with increased mortality from cardiovascular diseases. Meanwhile, extensive clinical and toxicological studies have also provided evidence for stronger association between air pollution and deaths from cardiovascular diseases.8, 9, 10, 11 However, most of these studies were conducted in developed countries and there were limited amount of research done in China.
From 2003 to 2012, annual average levels of particulate matter less than 10 μm in aerodynamic diameter (PM10) in the 31 provincial capitals in China were significantly reduced (Figure 1); however, they were still at the higher end of air pollution level in the world. In 2013, the report on Global Environmental Competitiveness ranked the air quality of China 87th out of 133 countries.12 Beijing, the capital of China, experienced rapid urban expansion and transportation development and hence, led to a serious air pollution problem in the past 10 years,13 during which the number of its resident population increased from 14.56 million in 2003 to 21.15 million in 2013.14 Over the same period, the number of automobiles, a major source of ambient air carbon monoxide (CO) and nitrogen oxides (NOX) emissions, increased by 2.5 times, totaling 5.4 million at the end of 2013.15 Beijing is still facing a substantial challenge of balancing economic growth and environmental protection.

Annual average ambient levels of PM10 and NO2 in 31 provincial capitals (including Beijing) of China 2003–2012. The gray-dotted line indicates air quality as Class II based on its annual levels by the National Ambient Air Quality Standards (NAAQS) in China. Data source: China Statistic Yearbook 2004–2013.
Concerns about effects of air pollution on population health, for example, cardiovascular diseases,6, 16 respiratory diseases16, 17, 18 and emergency hospital visits19, 20, 21, 22 have been increasing in Beijing. However, most of the existing studies characterized exposures using citywide average ambient concentrations of pollutant, which ignored the within-city spatial variation in concentrations of ambient air pollutants because of lacking data from multiple air quality monitoring (AQM) stations. In fact, exposure levels vary greatly across the whole area of Beijing.23 A study showed that air quality in the southern part was worse than that in the northern part in Beijing.24 And from the southeast plain to the northwest mountain area in Beijing, pollution levels presented a decreasing trend. Chen et al.25 pointed that the spatial variation in the effects of PM10 on health outcomes needs to be considered in assessing the health effect of air pollution, particularly for big cities. The study by Zhang et al.26 applied district-specific PM10 concentrations to quantify the impact of PM10 on population health. However, the study did not include the suburban and rural districts and examined the effects of nitrogen dioxide (NO2) and CO. In our study, we aimed to apply the generalized additive mixed model (GAMM) to investigate the spatial characteristics of association between air concentrations of PM10, NO2 and CO and daily cardiovascular mortality in the whole area of Beijing.
Materials and methods
The study was based on Causes of Death Registry (CDR) of the China Centers for Disease Control and Prevention (China CDC), but did not access any individually identifiable patient data. The study was approved by the Institutional Review Board of institute of Basic Medical Sciences, Chinese Academy of Medical Sciences.
Study Area and Period
Beijing is located in the North China Plain with an area of approximate 16,807 km2 and a population of 21.15 million by the end of 2013.14 The study area covered 16 administrative districts of Beijing, including six urban districts (Dongcheng, Xicheng, Chaoyang, Fengtai, Shijingshan and Haidian), eight suburban districts (Mentougou, Fangshan, Tongzhou, Shunyi, Changping, Daxing, Huairou and Pinggu) and two rural counties (Yanqing and Miyun) (Figure 2). The study was carried out from 1 January 2009 to 31 December 2010.

Distribution of 16 administrative districts and 12 air quality monitoring stations in Beijing.
Data Collection
The data here include the number of daily cardiovascular deaths, air quality, road density and meteorological conditions.
Cardiovascular mortality data were obtained from CDR of China Centers for Disease Control and Prevention (CDC). All deaths in CDR were coded according to the International Classification of Diseases, version 10 (ICD-10), with codes I00-I99 used as deaths from cardiovascular diseases.
Air quality data, including the concentrations of PM10, NO2 and CO, were generated by district AQM stations at 12 fixed sites in Beijing (Figure 2). All district AQM stations are operated by the Chinese National Monitoring Network for Air Quality Control. The hourly average concentrations for each pollutant were presented. Data from one AQM station (Dingling station in Changping district) were excluded because it was used as the background station for calibration. For the districts having two AQM stations, arithmetic mean of the concentrations of the two stations was used. For the districts without AQM station, a generalized linear model was used to project their pollutant concentrations. The method was described in detail elsewhere.27
To adjust the effect of weather condition on mortality,28, 29 data on meteorological conditions, including mean daily temperature, relative humidity, wind speed and barometric pressure during the same period were obtained from the Beijing Municipal Meteorological Bureau.
Data Analysis
We used the district-level daily cardiovascular deaths as the dependent variable and the corresponding district-level daily PM10, NO2 and CO as the main independent variables. Generalized additive model (GAM) was used to associate the mortalities and the pollutants,30 and GAMM to account for overdispersion and random effect of district to the additive predictor,31 under the assumption that the number of daily deaths from cardiovascular diseases follows a Poisson distribution. Natural splines were used to fit the non-linear time trend of the mortality, adjusting for potential confounders, such as day of week (DOW) and meteorological conditions.32 The full GAMM included smoothing function for variables time, temperature and humidity, categorical variable DOW and random effect of district, which can be expressed as:

where E(Yi,t) refers to the expected count in district i on day t, DOW is dummy variable for day of week, and Zi is a random intercept for districts i. s(.) is the smoothing function realized by natural spline with 2 degrees of freedom (d.f.) per year for time to adjust for seasonal and long-term trends and 5 degrees of freedom for temperature and 2 for relative humidity. The most appropriate degrees of freedom of the time, temperature and relative humidity were determined by minimizing Akaike Information Criterion (AIC).31
We also compared the citywide effects derived from GAMM and those from GAM. The GAM and GAMM models include the same non-parametric smoothing function for PM10, NO2 and CO and other confounding factors. The GAM can be expressed as:

Furthermore, we examined the associations with different lag structures, including single-day lags (from lag 0 to lag 4) and multiday lags (moving average lag 0–1 to lag 0–4).
Sensitivity analyses were conducted to investigate the robustness of the citywide associations by changing degree of freedom per year for time trend, using penalized spline for time trends and adding barometric pressure.
All statistical tests were two-sided. The effects of pollutants were presented as percentage changes and corresponding 95% confidence intervals (CIs) of mean number of daily deaths per interquartile ranges (IQR) increment in daily concentrations of PM10, NO2 and CO. Incidence rate ratios (IRRs) were calculated to evaluate the relative risk of other districts compared with the reference district. All the analyses were conducted by using “mgcv” package available in the R software (version 3.0.2).
Results
Descriptive Statistics
Descriptions of pollutant concentrations, meteorological conditions and cardiovascular mortality in Beijing from 1 January 2009 to 31 December 2010 are given in Table 1.
During the 2-year study period, annual mean concentrations of the three air pollutants were 121.0 μg/m3, 55.0 μg/m3 and 1.5 mg/m3 for PM10, NO2 and CO, respectively. Annual mean concentrations of PM10 and NO2 were above the Class II limits of the National Ambient Air Quality Standards of China (100 μg/m3 for PM10 and 40 μg/m3 for NO2, respectively).33 Average temperature was 12.98 °C ranging from −12.5 °C to 34.5 °C, and average relative humidity was 50.98% ranging from 13.0% to 92.0% during the same time period, showing a typical sub-humid warm continental monsoon climate of Beijing. In the study period, a total of 74,775 cardiovascular deaths occurred within the whole area of Beijing, with average daily deaths of 102.4.
District-specific median concentrations and their IQRs of PM10, NO2 and CO are shown in Table 2. Median daily concentrations of PM10, NO2 and CO range from 82.5 to 129.0 μg/m3, 30.0 to 59.0 μg/m3 and 0.90 to 1.40 mg/m3, respectively, with the highest levels in Shijingshan, Xicheng and three central urban districts (Shijingshan, Dongcheng and Xicheng), respectively. The highest number of daily deaths from cardiovascular diseases was found in Chaoyang district.
In six districts of Beijing, the daily average concentrations of the three air pollutants in most of the days exceeded the limits of Class II in the National Ambient Air Quality Standards of China (Table 3).33 For the whole area of Beijing, the number of days with daily 24-h average concentration of PM10 higher than the limit accounted for about one quarter of the period, which was observed in five urban districts (Shijingshan, Dongcheng, Haidian, Xicheng and Chaoyang) and one suburban district (Shunyi).
Citywide Effects of Air Pollutions
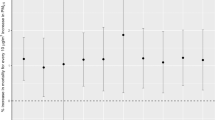
Figure 3 shows that the point estimates and relevant 95% CIs for the percentage increase in number of citywide daily deaths per IQR increase in concentrations of PM10, NO2 and CO. Results of GAM fitting indicate the effects of PM10, NO2 and CO on current day (lag 0), the previous day (lag 1), the moving average 2 days (lag 0–1), the moving average 3 days (lag 0–2) and the moving average 4 days (lag 0–3) are statistically significant. The statistically significant association of cardiovascular mortality with NO2 is also found on the moving average 5 days (lag 0–4). Generally, strong single-day effect occurs on lag 1; the strong accumulated effect occurs when 2-day average is used. The cumulative exposure on lag 0–1 has the largest effect. An IQR increase in pollutant concentration was associated with 2.87 (95% CI, 1.66–4.09), 5.02 (95% CI, 3.54–6.52) and 4.11 (95% CI, 2.84–5.40) percentage increase in daily cardiovascular deaths for PM10, NO2 and CO, respectively.

Percentage increase in daily cardiovascular deaths associated with an IQR increase in air pollutant concentrations from GAMM (dotted lines) and GAM (solid lines) in Beijing from 2009 to 2010.
We found the largest effects at lag 0–1 by using both GAMM and GAM. However, the estimated effects of air pollutions derived from GAM are higher than those derived from GAMM (Figure 3). An IQR increase in concentrations of PM10, NO2 and CO is associated with 2.46 (95%CI, 1.22–3.72), 4.11 (95%CI, 2.82–5.42) and 2.23 (95%CI, 1.14–3.33) percentage increase in daily cardiovascular deaths, respectively.
District-Specific Effects of Air Pollutions
Because the largest effect of pollutants is generally found on lag 0–1, only the relationship between concentrations of PM10, NO2 and CO and cardiovascular deaths on lag 0–1 is shown in Figure 4.

The district-specific relative risks (Changping as a reference district) of cardiovascular mortality of air pollutants based on GAMM in Beijing from 2009 to 2010.
The relative risks of every other district compared with Changping are ranked and the same ranking patterns are found for the three pollutants (Figure 4). All districts but Haidian have statistically significant higher risk. Haidian shows a lower significant risk (IRR=0.88, 95%CI, 0.85–0.92).
Each district was used as a reference district in turn, and we compared death risk of district with the reference district respectively. The relative risks are presented in Supplementary eFigure 1. For the three pollutants, the lowest risk of death from cardiovascular disease is in one urban district Haidian, and the highest risk is in one suburban district Pinggu. The death risks in the suburban and rural areas appeared to be stronger than those in the urban areas under the same level of pollutants.
Cardiovascular mortality risks associated with PM10 exposure, shown in Supplementary eFigure 1, have statistically significant difference between different districts except Daxing and Shijingshan (IRR=1.04, 95%CI: 0.99–1.11), Yangqing and Dongcheng (IRR=1.05, 95%CI, 0.99–1.11), Yanqing and Xingcheng (IRR=1.01, 95%CI, 0.95–1.07), Fangshan and Yanqing (IRR=1.03, 95%CI, 0.97–1.10), Shunyi and Fangshan (IRR=1.02, 95%CI, 0.98–1.07), Huairou and Shunyi (IRR=1.03, 95%CI, 0.97–1.09) and Miyun and Mentougou (IRR=1.03, 95%CI, 0.97–1.10). The cardiovascular mortality risks associated with NO2 (Supplementary eFigure 2) and CO (Supplementary eFigure 3) exposure are similar to that of PM10. In general, the effects of PM10, NO2 and CO on cardiovascular mortality were different among districts.
Sensitivity Analysis
The change in degree of freedom per year for time trend dose not substantially affect the estimated effects of air pollutants within the range of two to eight degrees of freedom. Different smoothing approaches do not change the effect estimates significantly (results not shown). The analyses suggest that our findings are robust with respect to these issues. Adding barometric pressure to the models result in almost identical estimates.
Discussion
In this multi-site time-series study of excess cardiovascular mortality risk attributable to air pollution, we investigated the spatial variation in associations between short-term exposure to ambient PM10, NO2 and CO and daily deaths from cardiovascular diseases. It is worth noting that there is significant spatial variation in the estimated effects of PM10, NO2 and CO on cardiovascular mortality across the 16 districts in Beijing.
We observed the highest levels of PM10 and CO in Shijingshan district, and the highest levels of NO2 and CO in Xicheng district, where the level of NO2 was nearly twice as much as that in Huairou district. Shijingshan district is a heavily industrialized zone with iron and steel production industry, metal smelting industry and thermal power plants. Smaller particles and organic pollutants produced during coal combustion and transportation might be the main contributor of the much higher concentrations of PM10 and CO in this district than in other districts.34 Xicheng district is located at the center of Beijing, with high road density and more serious vehicle traffic jams, which leads to higher emission level of oxynitride and carbon from automobile exhaust.
Many studies provided evidence linking air pollutants with adverse health effects based on the assumption that exposure is uniform within each region or city. Such an assumption might result in errors in estimation of exposure, especially for pollutants with important local sources.35 However, previous studies have suggested that using data from a single AQM station or average concentrations from a few stations might not accurately represent citywide exposure and might lead to bias,23 as the air pollution levels often vary across the study area.36 Confounding factors that vary between districts might also distort their relation with air pollution. In our study, we modeled PM10, NO2 and CO at a district level to evaluate their citywide effects on cardiovascular mortality using GAMM. Treating district as a random effect enabled us to account for lack of independence between observations for each district, which might generate more accurate estimates compared with using citywide averaged concentrations. We found significant effects of PM10, NO2 and CO on cardiovascular mortality, which are similar to those found in the previous studies in the United States,37 Europe38, 39 and China.3, 6, 16
Meanwhile, we also fitted a GAM that used average concentration of air pollutants in 16 districts of Beijing. Results show that the estimated effects of PM10, NO2 and CO derived from GAM are higher than those derived from GAMM (Figure 3), which is contradicted to findings by Zhang et al. and Xu et al.26, 40 However, Zhang`s and Xu`s studies were conducted in 2008–2009. Annual mean concentration of PM10 in 2008–2009 was slightly higher than that in 2009–2010 (127.7 vs 121.0 μg/m3). Different time periods and pollution levels might also be potential reasons of the inconsistence. Furthermore, the spatial characteristics of association of gaseous pollutants, such as NO2and CO, were not investigated in Zhang’s and Xu`s studies.
Our findings indicate that there is a spatial variation in estimated effects of PM10, NO2 and CO on cardiovascular mortality across the 16 districts of Beijing. Consistent with previous reports,41 we found that suburban and rural residents expose to a greater risk of cardiovascular death correlated with air pollution than urban residents in Beijing. Because of the different emission sources, physicochemical characteristics, weather conditions, geographical factors, industry and transportation infrastructures, and traffic densities, the composition of air pollutants might differ between urban and rural districts.34, 42 Insufficiency of protection awareness and measures and emergent medical assistance might contribute to this difference.41 In addition, the population structure might be another factor that may contribute to this spatial variation. For example, the higher proportion of elderly people and children in some rural areas because of young population migration to urban areas leads higher morbidity and mortality of respiratory and cardiovascular diseases in these areas.43 Access to quality health care could be another potential contributor to spatial variation. High quality hospitals mainly concentrate in urban areas. According to the Beijing Health Development Statistical Bulletin 2009, the number of health institutions in urban areas accounted for 58.8%, and those in rural areas only accounted for 4.5%.44
To make our results comparable to those of other Asian cities, we converted our percent increase in daily cardiovascular mortality associated with an IQR increase in pollutant concentrations into 10 μg/m3 increase for PM10 and NO2. Using 2-day moving average of the air pollutant concentrations, an increase of 10 μg/m3 of PM10 was associated with 0.35 (95%CI, 0.21–0.50) percentage increases in cardiovascular mortality, and the corresponding number was 1.97 (95%CI, 1.39–2.55) for 10 μg/m3 increase in NO2. A study of PM10 and ischemic heart disease mortality in Beijing from 2008 to 2009 indicates that a 10 μg/m3 increase in PM10 is associated with an increase of 0.33 (95%CI, 0.13–0.52) percentage.40 Our estimate is similar to the result. PAPA study estimates that an increase of 10 μg/m3 in 2-day moving average concentrations of PM10 and NO2 corresponded to 0.27 (95%CI, 0.10–0.44) percentage and 1.01 (95%CI, 0.55–1.47) percentage in Shanghai, 0.57 (95%CI, 0.31–0.84) percentage and 2.21 (95%CI, 1.18–3.06) percentage in Wuhan, 1.9 (95%CI, 0.8–3.0) percentage and 1.8 (95%CI, 0.5–3.1) percentage in Bangkok.45 There is little difference between our estimates in Beijing and PAPA results in the other megacities in East Asia. And our results could serve as a complement to the PAPA study.
To our knowledge, our study is the largest study that examined the spatial variation in effects of ambient PM10, NO2 and CO concentrations on cardiovascular mortality across the whole area in Beijing. The air quality data measured from 12 fixed AQM stations represented the comprehensive air pollution level across the whole area of Beijing. Fitted GAMM used additive non-parametric functions to describe covariate effects that accounted for between-district heterogeneity and within-district correlation by adding random effects to the additive predictors.46 However, there are limitations in our study. First, ambient AQM results can differ from personal exposure to air pollutants.47 Numerous factors, such as air conditioning, ventilation between indoor and outdoor air, may affect monitoring results from fixed stations as surrogates of personal exposure to air pollutants.48 In addition, as a requirement, AQM stations are located away from the major roads and industrial emission sources; therefore, underestimation and misclassification of exposure might exist. Second, district-specific data of meteorological conditions were unavailable. The use of citywide meteorological data may not reveal their confounding on effects of district level of air pollutants. Third, age structure of study population in each district is different and not adjusted. Population aged more than 60 years old (the older polulation) in Changping and Daxing districts accounted for the least (less than 10%) and those in Dongcheng and Xicheng district the most (more than 16%). In addition, the proportion of populations aged over 60- are higher in Pinggu, Miyun and Yanqing districts (about 15%) than those in Chaoyang, Fengtai and Shijingshan districts (about 13%). The differences in ratio of the older popularion might confound the estimates of effects as well. We conducted stratified analyses by age (45–64 years and ≥65 years) to examine potential effect modification. We observed that the effects of PM10, NO2 and CO on cardiovascular mortality are different among districts both in residents aged 45 or older and in aged 65 years or older.
In addition, socioeconomic status is also a factor that may contribute to the spatial variation. We tried to include gross domestic product per capita and number of health institutions per 1000 people of 16 districts in 2009 and 2010 to adjust for potential confounding from socioeconomic factors, however, because these indicators were measured annually in a district level, only 32 values of these indicators corresponding to 730 × 16 observations resulted in problem of singularity in backsolve in GAM and GAMM. We are collecting individual socioeconomic information form an ongoing cohort and will investigate this issue in future studies.
In general, the results from this study are meaningful for the present situation in Beijing. The yearly average PM2.5 concentration observed by US Embassy in Beijing was about 91–104 μg/m3 from 2009 to 2014 without obvious trend.49 And the yearly average PM10 concentration of the whole Beijing during this period was about 108–121 μg/m3 according to Beijing Environmental Statement 2009–2014.50 Therefore the study period, 2009 and 2010, showed similar pollution level with the most recent years, and the findings may have implication for current public health policy decision making. Almost all the existing studies conducted in Beijing that analyzed the effects of air pollution took pollution of the city as a whole. However, our study reveals the spatial variation of such effects across the whole area of the city, which provides important evidence to help identify and explain the inequality in health status between different districts of Beijing in the context of high air pollution level. The findings drive our future efforts toward the further analysis to discover potential interaction between air pollution and socioeconomic factors.
Conclusions
In summary, we found significant adverse effects of ambient PM10, NO2 and CO on deaths from cardiovascular diseases. There were spatial variations in ambient concentrations of PM10, NO2 and CO and relative higher mortality risk of cardiovascular diseases in rural areas in Beijing. Further researches that identify personal exposure and sources of pollutions are needed to confirm our findings and to promote effective strategy of air quality management and public health protection.
References
Middleton N, Yiallouros P, Kleanthous S, Kolokotroni O, Schwartz J, Dockery DW et al. A 10-year time-series analysis of respiratory and cardiovascular morbidity in Nicosia, Cyprus: the effect of short-term changes in air pollution and dust storms. Environ Health 2008; 7: 39.
Chen R, Chu C, Tan J, Cao J, Song W, Xu X et al. Ambient air pollution and hospital admission in Shanghai, China. J Hazard Mater 2010; 181: 234–240.
Chen R, Pan G, Zhang Y, Xu Q, Zeng G, Xu X et al. Ambient carbon monoxide and daily mortality in three Chinese cities: the China Air Pollution and Health Effects Study (CAPES). Sci Total Environ 2011; 409: 4923–4928.
Dominici F, Peng RD, Zeger SL, White RH, Samet JM . Particulate air pollution and mortality in the United States: did the risks change from 1987 to 2000? Am J Epidemiol 2007; 166: 880–888.
Breitner S, Stolzel M, Cyrys J, Pitz M, Wolke G, Kreyling W et al. Short-term mortality rates during a decade of improved air quality in Erfurt, Germany. Environ Health Perspect 2009; 117: 448–454.
Wong CM, Ou CQ, Chan KP, Chau YK, Thach TQ, Yang L et al. The effects of air pollution on mortality in socially deprived urban areas in Hong Kong, China. Environ Health Perspect 2008; 116: 1189–1194.
Kim H, Kim Y, Hong Y . The lag-effect pattern in the relationship of particulate air pollution to daily mortality in Seoul, Korea. Int J Biometeorol 2003; 48: 25–30.
Jevtic M, Dragic N, Bijelovic S, Popovic M . Cardiovascular diseases and air pollution in Novi Sad, Serbia. Int J Occup Med Environ Health 2014; 27: 153–164.
Ibald-Mulli A, Timonen KL, Peters A, Heinrich J, Wolke G, Lanki T et al. Effects of particulate air pollution on blood pressure and heart rate in subjects with cardiovascular disease: a multicenter approach. Environ Health Perspect 2004; 112: 369–377.
Brook RD, Rajagopalan S, Pope CR, Brook JR, Bhatnagar A, Diez-Roux AV et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation 2010; 121: 2331–2378.
Pun VC, Yu IT, Qiu H, Ho KF, Sun Z, Louie PK et al. Short-term associations of cause-specific emergency hospitalizations and particulate matter chemical components in Hong Kong. Am J Epidemiol 2014; 179: 1086–1095.
Jianping L, Minrong L, Jinnan W, Jianjian L, Hongwen S, Maoxing H et al. Report on Global Environment Competitiveness of China. Springer: Berlin Heidelberg. 2014. Report No.: 978-3-642-54677-8; 2194–7937.
Cai J, Zhao A, Zhao J, Chen R, Wang W, Ha S et al. Acute effects of air pollution on asthma hospitalization in Shanghai, China. Environ Pollut 2014; 191: 139–144.
Beijing Statistical Yearbook 2013. Available from http://www.bjstats.gov.cn/nj/main/2013-tjnj/index.htm.
Statistical Bulletin of National Economy and Social Development of Beijing in 2013. Available from http://www.bjstats.gov.cn/xwgb/tjgb/ndgb/201402/t20140213_267744.htm.
Zhang F, Li L, Krafft T, Lv J, Wang W, Pei D . Study on the association between ambient air pollution and daily cardiovascular and respiratory mortality in an urban district of Beijing. Int J Environ Res Public Health 2011; 8: 2109–2123.
Li P, Xin J, Wang Y, Wang S, Li G, Pan X et al. The acute effects of fine particles on respiratory mortality and morbidity in Beijing, 2004-2009. Environ Sci Pollut Res 2013; 20: 6433–6444.
Chang G, Pan X, Xie X, Gao Y . Time-series analysis on the relationship between air pollution and daily mortality in Beijing(in chinese). Wei Sheng Yan Jiu 2003; 32: 565–568.
Guo Y, Tong S, Zhang Y, Barnett AG, Jia Y, Pan X . The relationship between particulate air pollution and emergency hospital visits for hypertension in Beijing, China. Sci Total Environ 2010; 408: 4446–4450.
Guo Y, Tong S, Li S, Barnett AG, Yu W, Zhang Y et al. Gaseous air pollution and emergency hospital visits for hypertension in Beijing, China: a time-stratified case-crossover study. Environ Health 2010; 9: 57.
Guo Y, Jia Y, Pan X, Liu L, Wichmann HE . The association between fine particulate air pollution and hospital emergency room visits for cardiovascular diseases in Beijing, China. Sci Total Environ 2009; 407: 4826–4830.
Zhang F, Wang W, Lv J, Krafft T, Xu J . Time-series studies on air pollution and daily outpatient visits for allergic rhinitis in Beijing, China. Sci Total Environ 2011; 409: 2486–2492.
Yanosky JD, Paciorek CJ, Schwartz J, Laden F, Puett R, Suh HH . Spatio-temporal modeling of chronic PM10 exposure for the Nurses’ Health Study. Atmos Environ 2008; 42: 4047–4062.
Dong F WXWZ . A study of the north-south differences of the air quality in Beijing (in chinese). Climatic Environ Res 2013; 1: 63–70.
Chen L, Mengersen K, Tong S . Spatiotemporal relationship between particle air pollution and respiratory emergency hospital admissions in Brisbane, Australia. Sci Total Environ 2007; 373: 57–67.
Zhang Y, Guo Y, Li G, Zhou J, Jin X, Wang W et al. The spatial characteristics of ambient particulate matter and daily mortality in the urban area of Beijing, China. Sci Total Environ 2012; 435-436: 14–20.
Yang Y, Cao Y, Li W, Li R, Wang M, Wu Z et al. Multi-site time series analysis of acute effects of multiple air pollutants on respiratory mortality: a population-based study in Beijing, China. Sci Total Environ 2015; 508: 178–187.
Park AK, Hong YC, Kim H . Effect of changes in season and temperature on mortality associated with air pollution in Seoul, Korea. J Epidemiol Commun Health 2011; 65: 368–375.
Liu L, Breitner S, Pan X, Franck U, Leitte AM, Wiedensohler et al. Associations between air temperature and cardio-respiratory mortality in the urban area of Beijing, China: a time-series analysis. Environ Health 2011; 10: 51.
Lin X, Zhang D . Inference in generalized additive mixed modelsby using smoothing splines. J R Stat Soc Series B Stat Methodol 1999; 61: 381–400.
Yang L, Qin G, Zhao N, Wang C, Song G . Using a generalized additive model with autoregressive terms to study the effects of daily temperature on mortality. BMC Med Res Methodol 2012; 12: 165.
Yang Y, Li R, Li W, Wang M, Cao Y, Wu Z et al. The association between ambient air pollution and daily mortality in Beijing after the 2008 olympics: a time series study. PLoS One 2013; 8: e76759.
China National Ambient Air Quality Standard (GB 3095-1996). Available from http://www.chinaenvironment.com/view/viewnews.aspx?k=19961001160624453.
Dominici F, McDermott A, Zeger SL, Samet JM . National maps of the effects of particulate matter on mortality: exploring geographical variation. Environ Health Perspect 2003; 111: 39–44.
Hoek G, Brunekreef B, Goldbohm S, Fischer P, van den Brandt PA . Association between mortality and indicators of traffic-related air pollution in the Netherlands: a cohort study. Lancet 2002; 360: 1203–1209.
Peng RD, Bell ML . Spatial misalignment in time series studies of air pollution and health data. Biostatistics 2010; 11: 720–740.
Bell ML, Peng RD, Dominici F, Samet JM . Emergency hospital admissions for cardiovascular diseases and ambient levels of carbon monoxide: results for 126 united states urban counties, 1999-2005. Circulation 2009; 120: 949–955.
Samoli E, Touloumi G, Schwartz J, Anderson HR, Schindler C, Forsberg B et al. Short-term effects of carbon monoxide on mortality: an analysis within the APHEA project. Environ Health Perspect 2007; 115: 1578–1583.
Fischer PH, Marra M, Ameling CB, Janssen N, Cassee FR . Trends in relative risk estimates for the association between air pollution and mortality in The Netherlands, 1992-2006. Environ Res 2011; 111: 94–100.
Xu M, Guo Y, Zhang Y, Westerdahl D, Mo Y, Liang F et al. Spatiotemporal analysis of particulate air pollution and ischemic heart disease mortality in Beijing, China. Environ Health 2014; 13: 109.
Zhou M, He G, Fan M, Wang Z, Liu Y, Ma J et al. Smog episodes, fine particulate pollution and mortality in China. Environ Res 2015; 136: 396–404.
Lin G, Fu J, Jiang D, Hu W, Dong D, Huang Y et al. Spatio-temporal variation of PM2.5 concentrations and their relationship with geographic and socioeconomic factors in China. Int J Environ Res Public Health 2014; 11: 173–186.
Hwang JS, Chan CC . Effects of air pollution on daily clinic visits for lower respiratory tract illness. Am J Epidemiol 2002; 155: 1–10.
Beijing Municipal Commission of Health and Family Planning. Available from http://www.phic.org.cn/tonjixinxi/weishengtongjijianbian/2009nianjianbian/.
Wong CM, Vichit-Vadakan N, Vajanapoom N, Ostro B, Thach TQ, Chau PY et al. Part 5. Public health and air pollution in Asia (PAPA): a combined analysis of four studies of air pollution and mortality. Res Rep Health Eff Inst 2010; 154: 377–418.
Coull BA, Schwartz J, Wand MP . Respiratory health and air pollution: additive mixed model analyses. Biostatistics 2001; 2: 337–349.
Sarnat JA, Brown KW, Schwartz J, Coull BA, Koutrakis P . Ambient gas concentrations and personal particulate matter exposures. Epidemiology 2005; 16: 385–395.
Janssen NAH, Schwartz J, Zanobetti A, Suh HH . Air conditioning and source-specific particles as modifiers of the effect of PM10 on hospital admissions for heart and lung disease. Environ Health Perspect 2001; 110: 43–49.
US Department of State Air Quality Monitoring Program. Available from http://www.stateair.net/web/historical/1/1.html.
Beijing Municipal Environmental Protection Bureau. Available from http://www.bjepb.gov.cn/bjepb/413526/413663/413717/413719/index.html.
Acknowledgements
We thank all the following sectors for their assistances: the China National Environmental Monitoring Centre for providing air pollution data, the Beijing Municipal Meteorological Bureau for providing meteorology data, the China Center for Disease Control and Prevention for providing mortality data and the Beijing Municipal Traffic Management Bureau for providing road information data. This study is supported by the Special Scientific Research Fund for Public Welfare of Environmental Protection from the Ministry of Environmental Protection of China (Grant No. 200909016), Peking Union Medical College Graduate Student Innovation Fund in 2013, the Public Welfare Research Program of National Health and Family Planning Commission of China (Grant No. 201402022), and Opening Project of Shanghai Key Laboratory of Atmospheric Particle Pollution and Prevention (LAP3).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Journal of Exposure Science and Environmental Epidemiology website
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Li, W., Cao, Y., Li, R. et al. The spatial variation in the effects of air pollution on cardiovascular mortality in Beijing, China. J Expo Sci Environ Epidemiol 28, 297–304 (2018). https://doi.org/10.1038/jes.2016.21
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jes.2016.21
Keywords
This article is cited by
-
Increasing mortality caused by chronic obstructive pulmonary disease (COPD) in relation with exposure to ambient fine particulate matters: an analysis in Southeastern China
Environmental Science and Pollution Research (2021)
-
Effects of ambient carbon monoxide on daily hospitalizations for cardiovascular disease: a time-stratified case-crossover study of 460,938 cases in Beijing, China from 2013 to 2017
Environmental Health (2018)

{kind=link}
{kind=link}
{kind=link}