
Abstract
To compare the levels of agreement and the survival rates of sealant retention for different sealing materials over a 2-year period assessed using the visual clinical examination and replica methods, sealant retention data were obtained by visual clinical examination and from replicas of the same sealed tooth at baseline and at 0.5-, 1- and 2-year evaluation points in 407 children and were compared for agreement using kappa coefficients. Survival curves of retained sealants on occlusal surfaces were created using modified categorisation (fully retained sealants and those having all pits and fissures partly covered with the sealant material versus completely lost sealants that included pit and fissure systems that had ≥1 pit re-exposed) according to the Kaplan–Meier method. The kappa coefficient for the agreement between both assessment methods over the three evaluation time points combined was 0.38 (95% confidence interval (CI): 0.35–0.41). More sealant retention was observed from replicas than through visual clinical examination. Cumulative survival curves at the three evaluation times were not statistically significantly higher when assessed from replicas (P=0.47). Using the replica method, more retained sealant material was observed than through visual clinical examination during the 2-year period. This finding did not result in a difference in the survival rates of sealants assessed by the two assessment methods. When replicas cast in die stone are used for assessing sealant retention, the level of reliability of the data is higher than that of data obtained through the commonly used visual clinical examination, particularly if such assessments are conducted over time.
Similar content being viewed by others

Introduction
Sealants are effective not only in preventing carious lesion development,1 but also in stopping its progression.2 To maximize their effectiveness, sealants should be fully retained as long as possible.3,4,5 Retention of a sealant is dependent upon the material used,6 the preparation of pits and fissures7 and the training and experience of the operator, among other factors.8 The method predominantly used to assess sealant retention is visual clinical examination.
Despite being conducted by trained and calibrated evaluators using artificial light, mirrors and probes, visual clinical examination has a few shortcomings. The most conspicuous one is the inability to recall/reassess an observation made earlier.9 This limitation is particularly frustrating in the evaluation of sealant retention over time. Other shortcomings include the relatively short time in which the sealants are assessed, the light reflection by some materials that hinders proper visibility10 and evaluator fatigue over time, which may cause unreliable observations.9
One way to overcome these shortcomings is to apply the replica method using die stone, which has been used successfully for evaluating restorations,11,12 detecting developmental enamel defects13 and measuring the cement thickness of placed crowns.14 However, this method has rarely been used for assessing dental sealant retention.15 Cast in epoxy resin, the replica method has been used to detect remnants of sealant materials in pits and fissures in a restricted number of sealed teeth.16 The main advantage of using the replica method is the permanent availability of a set of models that allows the evaluator to assess the level of retention at leisure, at a convenient time.13 This method is thought to reduce operator fatigue and consequently, observation bias.
Therefore, the replica method may be more sensitive than visual clinical examination in measuring the levels of retention and degradation of dental sealants over time. However, only a few studies have compared the two methods with regard to the assessment of sealant retention over time.17,18 In these studies, the casts were fabricated using epoxy resin. No study appears to be available in which the casts have been fabricated using die stone.
This study aimed to compare the level of agreement and the survival rates of sealant retention with different sealing materials over a 2-year period as assessed by visual clinical examination and the replica method using die stone.
Materials and methods
Study background
Clinical data were obtained from a sealant trial in which four different sealant procedures were compared. The trial was conducted amongst 407 children (age: 7.0–9.1 years) at high risk of developing caries in Wuhan, China in 2008. In accordance with the study inclusion criteria, three operators (dentists) selected and sealed a total of 1 352 first permanent molars. For more information on this trial, the reader is referred to the paper by Chen et al.6 Parents or guardians of all included children received and signed the informed consent form. The sealant study was approved by the Research Ethics Committee of Wuhan University (Reference No. 200704) and was registered at the Dutch Trial Registration Centre (Reference No. 1411).
Clinical procedures
The four sealant procedures are outlined as presented before.6
Group 1—Glass ionomer: Ketac Molar Easymix (3M ESPE, Seefeld, Germany)
This group was a test group. Sealant application followed the atraumatic restorative treatment (ART) sealant procedure.19 The occlusal surfaces and the pits and fissures were cleaned with wet cotton wool pellets and a no. 6 explorer followed by drying with dry cotton wool pellets. Subsequently, the surfaces were conditioned with a moist pellet dipped in the glass-ionomer liquid for 10 s, washed twice with wet cotton wool pellets and dried with dry ones. Glass-ionomer powder and liquid were mixed within 30 s, applied to the surface with an applier/carver ART instrument (Henry Schein, Chicago, IL, USA) and firmly pressed into place for 5–10 s with a petroleum jelly-coated index finger (press-finger technique). Excess material and the petroleum jelly-coated top layer were removed using the applier/carver ART instrument. The surface was burnished using the smooth curved angle of the ART applier instrument and finally covered with a new layer of petroleum jelly. Children were advised not to eat or bite for at least 1 h.
Group 2—Glass ionomer plus added energy: Ketac Molar Easymix plus light-emitting diode (LED) high-energy curing light, Elipar Freelight 2 (3M ESPE, Seefeld, Germany), producing light intensity of 850 mW⋅cm−2
This group was a test group. The sealant application procedure described for Group 1 was followed, except that the surface was cured for 60 s after burnishing and before placement of the layer of petroleum jelly. The light intensity of the LED curing light was checked every week to ensure that it was always maintained above 750 mW⋅cm−2.
Group 3—Glass carbomer: Glass Carbomer (First Scientific Dental, Elmshorn, Germany)
This group was a test group. The occlusal surfaces and the pits and fissures were cleaned as described for Group 1 using cotton wool rolls for isolation. Thereafter, a cotton pellet dipped in Glass Carbomer Tooth Cleaner (First Scientific Dental, Elmshorn, Germany) was wiped over the tooth surface for 20 s for further cleaning. Cleaning was followed by washing and drying of the surface with two wet and dry cotton pellets, respectively. The Glass Carbomer capsule was activated and mixed for 15 s in a Rotomix (3M ESPE, Seefeld, Germany). The compound was then extruded onto the tooth surface within 1 min from the start of mixing, spread into a thin film, covered with Glass Carbomer Surface Gloss (First Scientific Dental, Elmshorn, Germany) and held under finger pressure for 5–10 s. The applier/carver ART instrument was used to remove excess material, and its smooth curved angle was used for burnishing the surface. Thereafter, the material was light-cured for 75 s using the same LED light as used in Group 2, and the same advice was given as children in Group 1 received.
Group 4—Resin composite, Clinpro (3M ESPE, St. Paul, MN, USA)
This group was the control group. The occlusal surfaces and the pits and fissures were cleaned with a Prophy Angle rotating brush (3M ESPE Wuhan, China) and a no. 6 explorer using cotton wool rolls for isolation. After thorough rinsing and drying, the occlusal surface was acid-etched using Scotchbond etchant (3M ESPE, St. Paul, MN, USA) for 20 s, rinsed and dried. The sealant material was placed in the pits and fissures, manipulated with an explorer to eliminate potential air bubbles and cured for 20 s with the LED curing light held 1 mm above the surface. Bite adjustment was performed using carbon paper and rotary instruments.
Visual clinical examination
The coverage of the pits and fissures with sealant material was recorded at baseline. The same two calibrated and experienced independent evaluators (dentists) performed clinical evaluations after 0.5, 1 and 2 years.6 The sealant retention criteria used are presented in Table 1. In addition to the usual criteria for assessing the retention of sealant materials, two codes were added for assessing the presence or absence of remnants in the deeper parts of pits and fissure systems. The criteria were applied to assess each of the three sections (mesial–central–distal) of mandibular teeth and each of the two sections (central and distal) of maxillary teeth into which the occlusal surface was arbitrarily divided. Before the examination, the sealed tooth surfaces were dried using a piece of cotton tightly attached to the end of a stick. The examination site was well illuminated by an intra-oral light attached to a mirror handle (Kudos, Hong Kong, China).
Evaluation using replica models
At baseline and at each evaluation point, an impression was made of the right mandibular first molar, as this tooth had been sealed most often. If that tooth had not been sealed, an impression of the left mandibular first molar was made. This impression was made to standardize the evaluation of sealed teeth as much as possible. If none of these teeth had been sealed, an impression of a sealed maxillary tooth was made.
Children brushed their teeth under supervision of a dentist at the school compound before the impression was made, approximately 1 week after completion of the visual clinical examination. In the chair, any remaining visible plaque was wiped away with a piece of gauze. The impression material was handled according to the Directions of Use provided by the manufacturer. The light body impression material Express (3MESPE, Seefeld, Germany) was syringed onto the dried occlusal surface, carefully avoiding the inclusion of air bubbles. At the same time, an assistant hand-mixed the silicone impression material Express STD Putty (3MESPE, Seefeld, Germany) and placed it in a partial dental impression tray. The tray was then positioned over the sealed tooth over which the light body impression material had been syringed. After removal of the tray, two examiners checked the impressions for the presence of voids, defects or air bubbles. If these defects were found, a new impression was made. Thereafter, impressions were rinsed under tap water and cast using dental gypsum powder FUJIROCK EP (GC, Tokyo, Japan) according to the manufacturers’ Directions of Use. A community periodontal index (CPI) probe was placed on several spots in the gypsum to reduce air bubbles.
All replicas from the same teeth taken at baseline and at the three evaluation points were lined up in time sequence for examination, which was performed over the course of 1 week by two trained and calibrated examiners, who were not the same as the examiners who performed the visual clinical examination. Training and calibration sessions covered 1 day and were held in the well-illuminated Key Laboratory of the School of Stomatology of Wuhan University under supervision of two senior scientists. The examiners were considered calibrated after the agreement exceeded a kappa coefficient of 0.80. The criteria used for assessing sealant retention from replicas were the same as the criteria used in the clinical examination, excluding codes 5 and 6 (Table 1). These codes required air blowing, which is not relevant when examining replicas. When necessary, evaluators used a loupe with a magnification factor of 3 to assess the presence of sealant material.
Quality of the data collected
Evaluators were recalibrated three times during the examination period, using 40 pairs of replicas randomly selected each time for estimating intra-evaluator and inter-evaluator consistency. For the two evaluators, the kappa coefficient values for the intra-evaluator consistency related to the assessment of sealant retention from replicas were 0.72 and 0.80, and the kappa coefficient value for the inter-evaluator consistency was 0.67. The kappa coefficient values for the intra-evaluator consistency of visual clinical examinations of the sealant trials were 0.89 and 0.93, while the value for the inter-evaluator consistency was 0.62.20
Statistical analysis
Retention codes 5 and 6, scored in the visual clinical examination, were recoded as code 4 for the analyses. The Kaplan–Meier method was used for creating survival curves, dichotomized into ‘completely and partially retained’ and ‘completely lost’, for the four types of sealants. This analysis was performed according to a modification of the commonly used traditional dichotomisation. This modification consists of ‘completely lost’ (combinations having at least a section with code 4), ‘completely retained’ (retention code 1 for all three sections) and ‘partially retained’ sealants (retention codes with all other combinations in the sections).6 The t-test was used to test for the presence of significant differences between survival rates as determined by visual clinical examination and the replica methods. A statistically significant difference was set at α=5%.
Results
Agreement between the two assessment methods
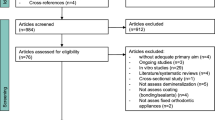
Overall, out of the 407 children enrolled in the trial, 370 children in whom it was possible to observe the same sealed tooth during the three evaluation times were analysed. The sample of replicas consisted of 81.3% right mandibular first molars, 10.8% left mandibular first molars and 7.9% maxillary first molars. Missed observations occurred 15 times during the evaluation period. The kappa coefficient values and 95% confidence intervals for the scoring levels of retention of occlusal sealants by the two assessment methods in terms of the time of evaluation are presented in Table 2 and are presented in terms of the sealant procedure in Table 3. All kappa coefficient values were substandard, indicating low levels of agreement between the two assessment methods after 0.5, 1 and 2 years.
A higher level of sealant retention was observed from replicas than through visual clinical examination. Our results showed that partially retained sealants were scored in only 6% of the cases by visual clinical examination in comparison to 39% from the replicas, while 15% of the sealants clinically scored as ‘completely lost’ were scored as ‘partially retained’ from the replicas.
Survival of sealants
The cumulative survival rates and standard errors of fully and partially retained occlusal sealants according to the two assessment methods are presented in Table 4. There was no statistically significant difference in cumulative survival curves between the two assessment methods (P=0.47).
The cumulative survival rates and standard errors of sealant retention by group over the 2-year assessment period are presented in Table 5. The retention rate for resin-composite sealants was statistically significantly higher when assessed through the replica method than through visual clinical examination at 2 years (P<0.0001). No differences between the methods were observed for the other three groups at 2 years. Although not statistically significantly different, except for Group 2 at year 0.5, survival rates of retention for the glass-ionomer sealant groups were higher when assessed through visual clinical examination than from replicas. The opposite was observed for the glass-carbomer and the resin-composite sealants.
Discussion
Assessment methods
This study showed that more retained sealant material was observed from replicas than through visual clinical examination. Whether this finding reflects the true situation cannot be ascertained as, in the absence of a gold standard, neither assessment method can be validated. The fact that ample time was spent in assessing retention of sealant material from replicas, if needed, and that scoring of retention was facilitated by the availability of four replica models per tooth, adds weight to the assumption that the evaluators were able to assess the sealant retention patterns with high levels of precision.
The evaluators who performed the visual clinical evaluations were different from those who performed the assessments from replicas. The extent to which the differences in evaluators contributed to the differences in scores obtained from both assessment methods is not known. As the intra- and inter-evaluator consistency tests for both assessment methods showed substantial reliability, we believe that this study’s findings reflect the true situation within the limits described above.
Sealant retention survival
Traditionally, survival of sealant retention is dichotomized into ‘no sealant material present’ and ‘material present independent of the extent of its coverage of the pits and fissures’. This implies that a pit and fissure system that is covered by sealant over a small portion is given the same value as a pit and fissure system that is fully covered with sealant material. Obviously, the risk for developing a carious lesion in an occlusal surface whose pits and fissures are barely covered is higher than in those surfaces whose pits and fissures are fully covered with sealant material. This difference in caries risk in the two situations is too large to justify the use of the traditional dichotomisation. Therefore, a different cutoff point for determining the dichotomy in sealant retention has been proposed.6 The guiding factor was the extent of the re-exposure of pits and fissures to the oral environment. A carious lesion usually develops in places where cariogenic plaque is stagnant for a sufficiently long time. In a pit and fissure system, this condition is more frequently observed in pits and fossae than in connecting fissures.21 As the occlusal surface was divided into three sections, and as each section commonly contains a pit with some major fossae, it was argued that one fully re-exposed section would make the occlusal surface vulnerable to demineralisation; a seal with one section lacking sealant material no longer provided sufficient protection was therefore considered ‘completely lost’.
The change in the dichotomy of what is and is not considered ‘retained’ is important in retention survival analyses, as it emphasizes the importance of the biological impact of sealants rather than the mechanical presence of a sealant material. This change resulted in rather low sealant survival rates. Using this modified categorisation, there was no significant difference between the two assessment methods in terms of survival rates for all sealants over 2 years and for the two glass-ionomer sealant groups. Remarkably, a significant difference was observed in the two methods with respect to the survival rates of the resin-based sealants assessed.
The replica method has a place in the assessment of sealant retention, particularly in longitudinal studies. Dental technicians can make the impressions, which is less costly than when dentists make the impressions. Whether this method is less costly than visual clinical examination is not known. It is also dependent on the frequency and number of impressions that have to be made. Judging all dentinal carious lesions from models may be difficult, but the lesions can be judged from pictures with a higher level of sensitivity than through visual clinical examination.22 A combined use of replicas for sealant retention and colour pictures for carious lesion assessment might increase the level of reliability of the data collected compared to data obtained through visual clinical examination. Further research is required to determine whether sealant retention might also be reliably assessed from pictures.
Conclusions
More retained sealant material was observed using the replica method than through visual clinical examination during the 2-year study period. This finding did not result in a difference in the survival rates of sealants assessed by the two assessment methods. The modified dichotomisation of determining partial retention and complete loss of sealant material is more appropriate for calculating the sealant survival rate than the traditional method.
References
Ahovuo-Saloranta A, Hiiri A, Nordblad A et al. Pit and fissure sealants for preventing dental decay in the permanent teeth of children and adolescents. Cochrane Database Syst Rev 2008; (4): CD001830.
Griffin SO . Caries risk in formerly sealed teeth. J Am Dent Assoc 2009; 140( 4): 415–423.
Mertz-Fairhurst EJ, Fairhurst CW, Williams JE et al. A comparative clinical study of two pit and fissure sealants: 7-year results in Augusta GA. J Am Dent Assoc 1984; 109( 2): 252–255.
Ripa LW . Sealants revisited: an update of the effectiveness of pit-and-fissure sealants. Caries Res 1993; 27( Suppl 1): 77–82.
Feigal RJ, Donly KJ . The use of pit and fissure sealant. Pediatr Dent 2006; 28( 2): 143–150.
Chen X, Du M, Fan M et al. Effectiveness of two new types of sealants: retention after two years. Clin Oral Investig 2012; 16( 5): 1443–1450.
Khoqli AE, Cauwels R, Vercruysse C et al. Microleakage and penetration of a hydrophilic sealant and a conventional resin-based sealant as a function of preparation techniques: a laboratory study. Int J Paediatr Dent 2013; 23( 1): 13–22.
Frencken JE, Makoni F, Sithole WD . Atraumatic restorative treatment and glass-ionomer sealants in a school oral health programme in Zimbabwe: evaluation after 1 year. Caries Res 1996; 30( 6): 428–433.
Wong HM, McGrath C, Lo EC et al. Photographs as a means of assessing developmental defects of enamel. Community Dent Oral Epidemiol 2005; 33( 6): 438–446.
Rock WP, Potts AJ, Marchment MD et al. The visibility of clear and opaque fissure sealants. Br Dent J 1989; 167( 11): 395–396.
Ho TF, Smales RJ, Fang DT . A 2-year clinical study of two glass ionomer cements used in the atraumatic restorative treatment (ART) technique. Community Dent Oral Epidemiol 1999; 27( 3): 195–201.
Farag A, van der Sanden WJ, Abdelwahab H et al. 5-year survival of ART restorations with and without cavity disinfection. J Dent 2009; 37( 6): 468–474.
Golkari A, Sabokseir A, Pakshir HR et al. A comparison of photographic, replication and direct clinical examination methods for detecting developmental defects of enamel. BMC Oral Health 2011; 11: 16.
Rahme HY, Tehini GE, Adib SM et al. In vitro evaluation of the “replica technique” in the measurement of the fit of procera crowns. J Contemp Dent Pract 2008; 9( 2): 25–32.
Mejàre I, Mjor IA . Glass ionomer and resin-based fissure sealants: a clinical study. Scand J Dent Res 1990; 98( 4): 345–350.
Frencken JE, Wolke J . Clinical and SEM assessment of ART high-viscosity glass-ionomer sealants after 8–13 years in 4 teeth. J Dent 2010; 38( 1): 59–64.
Futatsuki M, Kubota K, Yeh YC et al. Early loss of pit and fissure sealant: a clinical and SEM study. J Clin Pediatr Dent 1995; 19( 2): 99–104.
Aranda M, Garcia-Godoy F . Clinical evaluation of the retention and wear of a light-cured pit and fissure glass ionomer sealant. J Clin Pediatr Dent 1995; 19( 4): 273–277.
Beiruti N, Frencken JE, Mulder J . Comparison between two glass-ionomer sealants placed using finger pressure (ART approach) and a ball burnisher. Am J Dent 2006; 19( 3): 159–162.
Wang JD, Chen X, Frencken J et al. Dental caries and first permanent molar pit and fissure morphology in 7- to 8-year-old children in Wuhan, China. Int J Oral Sci 2012; 4( 3): 157–160.
Carvalho JC, Ekstrand KR, Thylstrup A . Dental plaque and caries on occlusal surfaces of first permanent molars in relation to stage of eruption. J Dent Res 1989; 68( 5): 773–779.
Boye U, Walsh T, Pretty IA et al. Comparison of photographic and visual assessment of occlusal caries with histology as the reference standard. BMC Oral Health 2012; 12: 10.
Acknowledgements
We thank the children and parents for their participation in the study and for their trust in the research team. We are grateful to the heads and staff of the primary schools for their kind reception and enthusiastic collaboration. We thank Professor W Rong and Professor E Lo for performing the visual clinical examination, the dental assistants and final-year dental students for their pleasant cooperation and their valuable contributions in making the impressions and casting the models and Jan Mulder for analysing the data. This study was financed by grants from the Ministry of Science and Technology, China (2007BA128B00), the Netherlands Academy of Science (08CDP011) and the Radboud University, the Netherlands (R0000463). We also thank 3M ESPE (Seefeld, Germany) and First Scientific Dental for providing sealant materials at no cost.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Hu, X., Chen, X., Ye, L. et al. Comparison between visual clinical examination and the replica method for assessments of sealant retention over a 2-year period. Int J Oral Sci 6, 111–115 (2014). https://doi.org/10.1038/ijos.2014.8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijos.2014.8
